An Approach to Bradycardia in the Emergency Department
- Nov 4th, 2016
- Patrick Ng
- categories:
Authors: Patrick C Ng, MD (EM Chief Resident, SAUSHEC Emergency Medicine Department) and Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC Emergency Medicine Department) // Edited by: Jennifer Robertson, MD, MSEd and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW Medical Center / Parkland Memorial Hospital)
Case
A 15-year-old male is brought to the emergency department (ED) via ambulance with a chief complaint of syncope. He reports that he was washing his hands in the bathroom at approximately 4:00 AM and the next thing he remembers, he was waking up to paramedics putting him on a stretcher. He denies preceding symptoms and does not report any relieving or exacerbating features. This has never happened to him before.
His review of systems is positive for recent rhinorrhea, cough, mild chest discomfort, and a low grade fever. His primary care physician was treating him symptomatically with a working diagnosis of an upper respiratory infection. The patient states that his symptoms had been improving.
Emergency medical services (EMS) reports the following vital signs on scene: blood pressure of 70/40 mm Hg, a heart rate of 36 beats per minute (bpm), a respiratory rate (RR) of 16/minute, a temperature of 100.6°Fahrenheit (F), an oxygen saturation of 98% on room air (RA), and a glucose level of 120. The patient’s vital signs upon arrival to your ED were similar and did not change despite intravenous (IV) fluids. A STAT echocardiogram was ordered and revealed decreased cardiac function. Laboratory tests were significant for an elevated troponin and white blood cell (WBC) count. A respiratory viral panel is positive for Coxsackie virus.
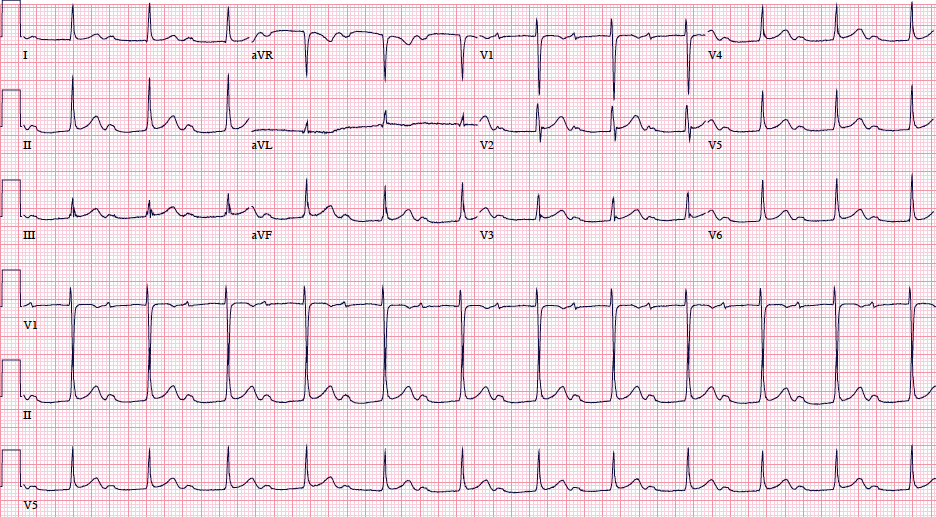
The patient’s electrocardiogram (EKG) is as follows:

(Image reproduced from: http://www.revespcardiol.org/; last accessed 10/19/2016)
You place pacing pads on the patient and start him on a dobutamine drip. He gets admitted to the pediatric intensive care unit and receives IV immunoglobulin (IVIG) for 3 days. He is downgraded to the floor and is discharged a week later with a discharge diagnosis of bradycardia and sick sinus syndrome, likely secondary to viral myocarditis.
This article will evaluate the ED approach to bradycardia. Before we get to the evaluation and management of the sick bradycardic patient, a little background in conduction is necessary…
Introduction
The cardiac conduction system consists of the His-Purkinje system. Electrical impulses are generated in the sinoatrial (SA) node, conducted down to the atrioventricular (AV) node, and then conducted down to the ventricles via the left and right bundle branches (Figure 1). A normal heart rate is typically between 60-100 bpm. Bradycardia is defined according to some sources as a heart rate below 60 bpm1.

Figure 1: Electrical conduction system of the heart. Image reproduced from: (http://1.bp.blogspot.com/-SfYtiDdSvC8/Tw2HuHJZ3ZI/AAAAAAAAALM/xkXHDdlt_Wk/s1600/conduction+system+of+the+heart.png) – Last Accessed 10/19/2016.
Bradycardia can be organized into two main categories: symptomatic and asymptomatic. Bradycardia can be normal in various individuals, particularly in children and well-conditioned athletes2,3. Some reports describe asymptomatic individuals with profound bradycardia defined as a HR <35 bpm. Findings of bradycardia in these individuals may not require any intervention, as long as the patient does not experience symptoms.
This is the opposite of patients with symptomatic bradycardia. The signs and symptoms of bradycardia are not specific and may include syncope, dizziness, chest pain, shortness of breath, and fatigue4. A slow heart rate can lead to heart failure and/or hemodynamic instability 5. Upon initial presentation, it is imperative the ED provider focus the history on determining if the patient is symptomatic.
The differential for symptomatic bradycardia is broad. One way to look at the differential is by broad categories which includes but is not limited to: structural/electrophysiological, infectious, endocrine, toxicology/iatrogenic, and other (Table 1).
Table 1 – Etiologies of Bradycardia
| Category | Possible Etiologies |
| Structural/Electrophysiological | -Sick Sinus Syndrome
-AV Block -Ischemia -Congenital Heart Disease -Prior Cardiac Surgery -Cardiomyopathy -Arterial Dissection (Aorta, Coronary, Carotid) |
| Infectious | -Myocarditis
-Lyme Disease -Bunyavirus -Dengue* -Typhoid Fever* -Legionnaires disease* -Psittacosis* -Leptospirosis* -Malaria* -Babesiosis* -Q fever* -Yellow Fever* -Rocky Mountain Spotted Fever* |
| Endocrine | -Hypothyroidism/Myxedema coma
-Bamforth syndrome -Hypothalamic dysfunction -Electrolyte Abnormalities/Malnutrition -Hashimoto’s thyroiditis |
| Toxicology/Iatrogenic | -Beta blocker**
-Calcium channel blocker** -Clonidine** -Guanfacine** -Digoxin** -Lidocaine** -Donepezil** -Organophosphate poisoning -Tacrine -Carbamate insecticide poisoning -Opioid** -Tricyclic Antidepressant Poisoning -Midodrine** -Levetiracetam overdose -Amitraz |
| Other | -Heat exhaustion/stroke
-Hypothermia -Leukomalacia -Increased Intracranial Pressure -Spinal Cord Injury -Carotid hypersensitivity syndrome -Chromosome 19p duplication syndrome -Fleisher syndrome -Young Simpson syndrome -Asphyxia neonatorum -Pneumothorax -Lupus Carditis -Oculocardiac Reflex -Dexmedetomidine -Prostaglandin |
Table 1: Causes of bradycardia8-20 (Not an all-inclusive list)
*Can cause relative bradycardia i.e. not in proportion to fever
** In overdose, and also at therapeutic dose
What are the key ED studies?
An EKG should be one of the first diagnostic tests obtained when bradycardia is recognized. Additionally, depending on the suspected etiology, a troponin, brain natriuretic peptide (BNP), electrolytes, infectious labs, chest x-ray, neuroimaging, and echocardiogram should be considered. The workup should be tailored to the initial clinical assessment. Not all patients warrant these tests.
The EKG is imperative, and examples of various heart blocks are shown below:

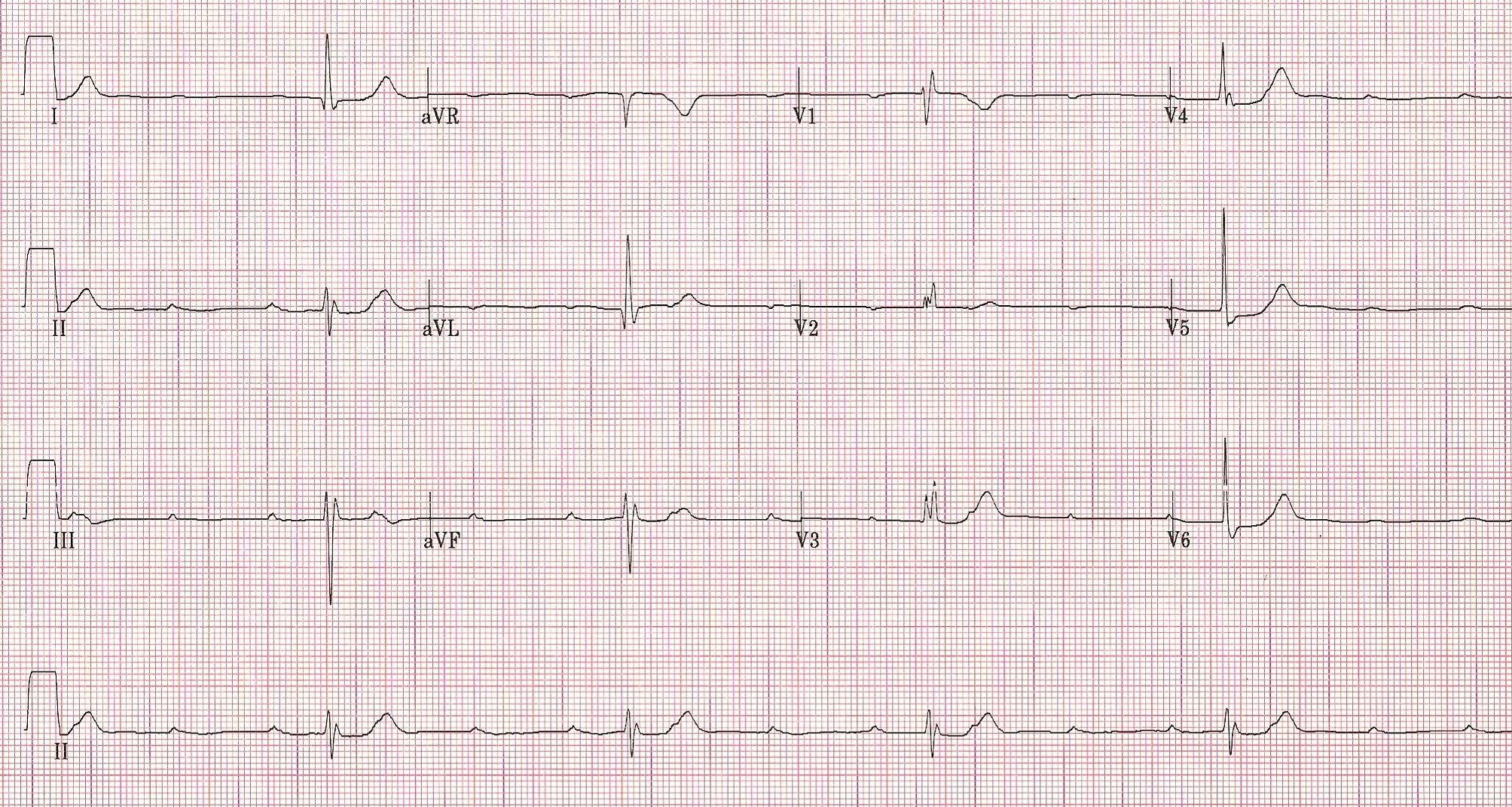
1st degree heart block- Image reproduced from: https://umem.org/files/uploads/content/ECG%20Challenge/Marked%201st%20degree%20AVB.jpg; last accessed 10/25/2016.

2nd degree block-Type I, Image reproduced from: http://www.patientcareonline.com/sites/default/files/cl/1527433.png; last accessed 10/25/2016.

2nd degree block-Type II, Image reproduced from: http://www.cardiocareconcepts.com/AV_Block_2.jpg; last accessed 10/25/2016

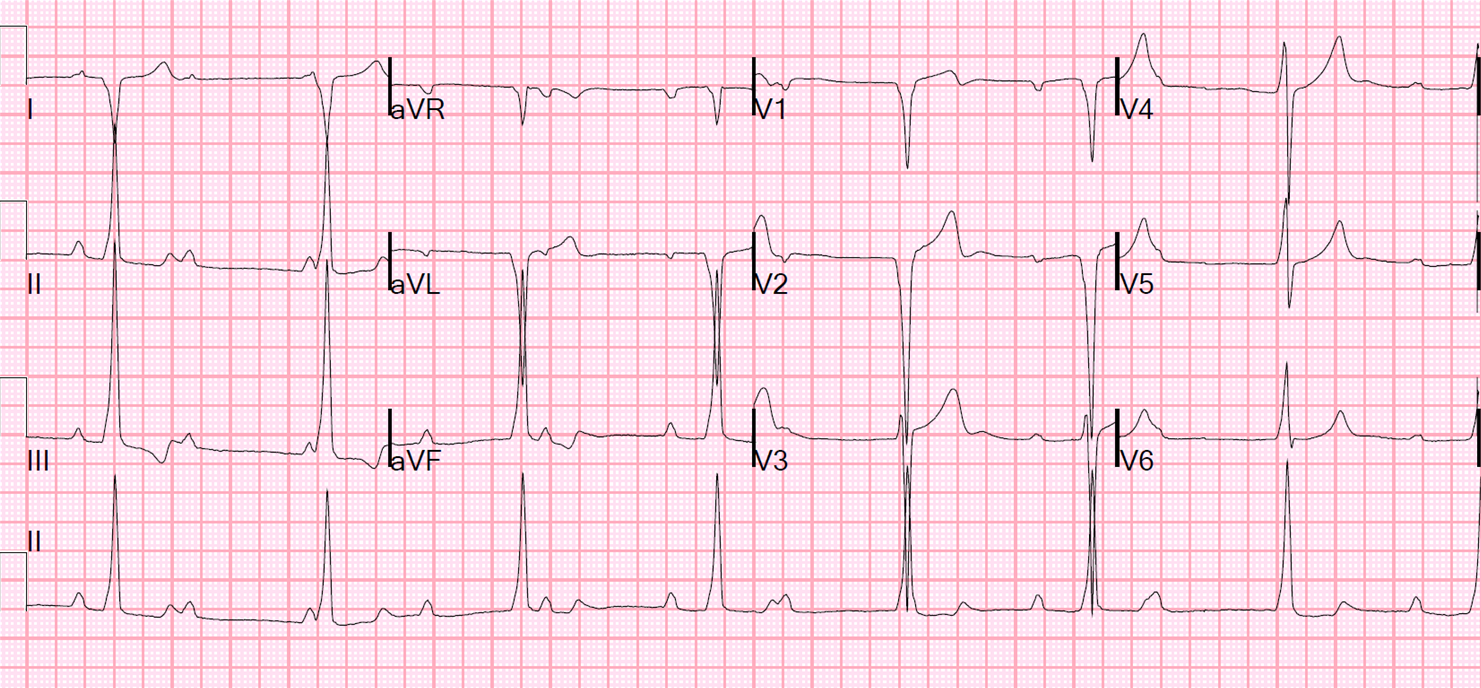
3rd degree block Image reproduced from: http://1.bp.blogspot.com/-qDCMtbuI1Zk/VFLbhSrRI-I/AAAAAAAAFRA/TqIn_yXm54I/s1600/Bradycardia%2Bwide%2BQRS%2Bthird%2Bdegree%2Bheart%2Bblock.png; last accessed 10/25/2016.

Sick Sinus-Alternating patterns of tachy- and bradyarrhythmia which can be seen with sick sinus syndrome. Image reproduced from: http://www.aafp.org/afp/2003/0415/p1725.html; last accessed 10/25/2016.
Management
As mentioned in the introduction, not all bradycardic rhythms require intervention, especially in the otherwise healthy, asymptomatic patients. If the ED provider is presented with a patient with symptomatic bradycardia, one of the first things to consider is the placement of transcutaneous pacer pads. Preparation for transvenous pacing (which requires a central line) should also be considered. Specific discussion of management plans for the different etiologies listed in Table 1 is too lengthy and out the scope of this post. General categories are mentioned below.
Structural/Electrophysiological (EP): A general way to approach potential structural/EP causes of bradycardia is to consider an abnormality that hinders the normal conduction of the heart. To address this, the emergency provider should consider transcutaneous/transvenous pacing to temporize the patient until definitive treatment can be obtained, such as percutaneous coronary intervention (PCI) for a ST elevation myocardial infarction (STEMI) or a permanent pacemaker for conduction abnormalities. An echocardiogram can assist in evaluation if a structural cause is suspected.
Infectious: Viral myocarditis is a more common cause of bradycardia in the infectious category. Myocarditis leading to hemodynamic compromise is important to consider, particular in the febrile, crashing child. Vasopressors, IVIG, and extracorporeal membrane oxygenation (ECMO) therapy have been reported in treating cardiogenic shock secondary to infectious etiologies. For further reading, consider reviewing: http://www.emdocs.net/pediatric-cardiogenic-shock/. Antibiotic therapy should be considered, particularly with tick-borne diseases such as Lyme disease.
Endocrine: Specific electrolyte and hormone abnormalities should be corrected. Thyroid disorders are a commonly reviewed topic for the emergency medicine inservice/board exam. For further management on myxedema coma, please review: http://www.emdocs.net/myxedema-aka-decompensated-hypothyroidism-an-em-primer/. An abnormal thyroid stimulating hormone can drastically change your management pathway. However, disorders such as thyrotoxicosis and myxedema coma are clinical diagnoses. The patient with myxedema coma should be given IV T4. IV T3 is an option as well, though it carries a higher risk of dysrhythmias.
Toxicology: The specific management plans for each potential toxin listed is out of the scope of this post. Beta blocker and calcium channel blocker toxicity is commonly seen in review books and examinations. Treatment includes glucagon, calcium supplementation, high dose insulin/glucose therapy, and potentially lipid emulsion therapy. For further reading on this topic, one can consider reviewing: http://www.emdocs.net/selected-toxicologic-bradycardias/
For cholinergic and hypnotic/sedative management, please review: http://www.emdocs.net/the-approach-to-the-poisoned-patient/
When reviewing medications and drug toxicity, it is vital to obtain a detailed medication reconciliation on patients with bradycardia, as a myriad of medications can cause a low heart rate.
Other: For etiologies listed in this category, there are a few management principles to consider for specific etiologies. For example, the emergency provider should understand the increased susceptibility of arrhythmias in the hypothermic patient. Warming these patients should take precedence over other interventions such as introducing a transvenous pacer. This is because without warming, hardware can cause a deadly arrhythmia.
For neurogenic/traumatic etiologies of bradycardia such as head trauma, specific interventions to decrease intracranial pressure (ICP) (head elevation, mannitol, hyperventilation, 3% saline) should be considered.
Summary
As seen, the differential for bradycardia is broad, and management depends on the suspected etiology. Not all bradycardia can be fixed with atropine and pacing. The emergency provider must focus his or her history and physical to narrow the differential to address the underlying pathology to effectively treat symptomatic bradycardia.
Overall remember that:
-Bradycardia is defined as a HR <60bpm
-Bradycardia can be benign and asymptomatic
-An EKG is essential to obtain as early as possible
-There is a broad differential for symptomatic bradycardia, and one can organize some of the causes into 5 categories: Structural/EP, Infectious, Endocrine, Toxicology/Iatrogenic, and Other
-Temporizing measures such as vasoactive drugs and pacing should be considered, but may not be effective in certain patients
References/Further Reading
- Spodick DH. Normal sinus heart rate: sinus tachycardia and sinus bradycardia redefined. Am Heart J. 1992 Oct;124(4):1119-21.
- Northcote RJ, Canning GP, Ballantyne D. Electrocardiographic findings in male veteran endurance athletes. Br Heart J. 1989 Feb; 61(2):155-60.
- Talan DA, Bauernfeind RA, Ashley WW, Kanakis C Jr, Rosen KM. Twenty-four hour continuous ECG recordings in long-distance runners. Chest 1982;82(1):19.
- Eraut D, Shaw DB. Sick sinus syndrome. Br Med J. 1973 Aug 4;3(5874):295.
- Tresch DD, Fleg JL. Unexplained sinus bradycardia: clinical significance and long-term prognosis in apparently healthy persons older than 40 years. Am J Cardiol. 1986 Nov 1;58(10):1009-13.
- Lateef A, Fisher DA, Tambyah PA. Dengue and Relative Bradycardia. Emerg Infec Dis. 2007 Apr;13(4):650-651.
- Ostergaard L, Huniche B, Andersen PL. Relative bradycardia in infectious diseases. J infect 1996;33:185-91.
- Tanriverdi S, Ulger Z, Siyah BB, Kultursay N, Yalaz M, Koroglu OA. Treatment of Congenital Complete Atrioventricular Heart Block With Permanent Epicardial Pacemaker in Neonatal Lupus Syndrome. Iran Red Crescent Med J. 2015 Sep 1;17(9):e16200
- Skog A, Lagnefeldt L, Conner P, Wahren-Herlenius M, Sonesson SE. Outcome in 212 anti-Ro/SSA-positive pregnancies and population-based incidence of congenital heart block. Acta Obstet Gynecol Scand. 2016 Jan;95(1):98-105.
- St-Onge M, Anseeuw K, Cantrell FL. Gilchrist IC, Hantson P, Bailey B, et al. Experts Consensus Recommendations for the Management of Calcium Channel Blocker Poisoning in Adults. Crit Care Med. 2016 Oct 3.
- Wong LY, Wong A, Robertson T, Burns K, Roberts M, Isbister GK. J Med Toxicol. 2016 Jul 4.
- Page CB, Mostafa A, Saiao A, Grice JE, Roberts MS, Isbister GK. Cardiovascular toxicity with levetiracetam overdose. Clin Toxicol. 2016;54(2):152-4.
- Roberts DM, Gallapatthy G, Dunuwille A, Chan BS. Pharmacological treatment of cardiac glycoside poisoning. Br J Clin Pharmacol. 2016 Mar;81(3):488-95.
- Dhooria S, Behera D, Agarwal R. Amitraz: a mimicker of organophosphate poisoning. BMJ Case Rep. 2015 Oct 1;2016.
- Graudins A, Lee HM, Druda D. Calcium channel antagonist and beta-blocker overdose: antidotes and adjunct therapies. Br J Clin Pharmacol. 2016 Mar;81(3):453-61.
- Leung AM. Thyroid Emergencies. J Infus Nurs. 2016 Sep-Oct;39(5):281-6.
- Wang FF, Xu L, Chen BX, Cui M, Zhang Y. Anorexia with sinus bradycardia: a case report. Beijing Da Xue Xue Bao. 2016 Feb 18;48(1):180-2.
- Alhussin W, Verklan MT. Complications of Long-Term Prostaglandin E1 Use in Newborns with Ductal-Dependent Critical Congenital Heart Disease. J Perinat Neonatal Nurs. 2016 Jan-Mar;30(1):73-9.
- Partida E, Mironets E, Hou S, Tom VJ. Cardiovascular dysfunction following spinal cord injury. Neural Regen Res. 2016 Feb;11(2):189-94.
- Thomsen JH, Nielsen N, Hassager C, Wanscher M, Pehrson S, Kober L, et al. Bradycardia During Targeted Temperature Management: An Early Marker of Lower Mortality and Favorable Neurologic Outcome in Comatose Out-of-Hospital Cardiac Arrest Patients. Crit Care Med. 2016 Jan;50(1):51-4.

%20-){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
5 thoughts on “An Approach to Bradycardia in the Emergency Department”