practice updates
- Nov 24th, 2016
- Jennifer Robertson
- leave a comment
- categories:
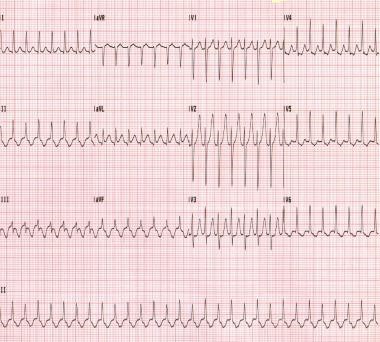
Cardiac arrhythmias are not common in pregnancy, but they can occur. While the workup and management is quite similar to the non-pregnant patient, there are subtle differences. This is a brief review of the ED management of unstable and stable tachycardic arrhythmias in pregnancy.