Hemoptysis: Key principles and management
- Oct 10th, 2016
- Patrick Ng
- categories:
Authors: Patrick C Ng, MD (EM Chief Resident, SAUSHEC Emergency Medicine Department) and Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC Emergency Medicine Department) // Edited by: Jennifer Robertson, MD, MSEd and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW Medical Center / Parkland Memorial Hospital)
Case 1
After being discharged from your hospital after a three-day stay for a bowel obstruction, a 76- year old male presents with two days of cough productive of green sputum with red streaks. He reports no relief with the use of his inhalers that he normally uses for his chronic obstructive pulmonary disease (COPD). Upon reviewing his chart, you notice that he had no cough during his hospital stay. His review of systems is positive for chills, intermittent nausea, and chest discomfort when actively coughing.
On examination, his vital signs are blood pressure (BP) 170/90, heart rate (HR) 110 beats per minute (bpm), respiratory rate (RR) 30 per minute, oxygen saturation (Sat) of 92% on room air (RA), and temperature (temp) of 101.6°Farenheit (F). He is actively coughing and is in mild distress. He coughs up about 1 cc of purulent material with red streaks in it. His right lower lung fields have significant crackles. Cardiac examination reveals tachycardia. Laboratory tests are significant for a white blood cell count of 16 x 109/L, a creatinine of 1.5mg/dL, and lactate of 2.5. Chest x-ray reveals a right lower lobe (RLL) infiltrate.
You make the diagnosis of hospital acquired pneumonia, start antibiotics and intravenous (IV) fluids and admit the patient for further management.
Case 2
An 80-year-old female presents to your emergency department (ED) with a sudden onset of shortness of breath. She recently completed a trans-Atlantic flight from London. Upon arrival to her room, you notice that she is in respiratory distress. She has never had anything like this before, and has no relief with oxygen supplementation. Her review of systems is positive for cough productive of reddish sputum.
Physical examination is significant for a swollen right calf. Her vital signs are: BP 80/60, HR 140, RR 46, Sat 88% on room air, and a Temp 100.3°F. Her EKG shows sinus tachycardia, and a bedside echocardiogram shows a dilated right ventricle (RV).
Suddenly, the patient goes into cardiac arrest. You start standard advanced cardiac life support (ACLS) protocol, intubate the patient, and call for tissue plasminogen activator (tPA) because you suspect a massive pulmonary embolism (PE) as the diagnosis. After rounds of chest compressions and a dose of tPA, you achieve return of spontaneous circulation (ROSC). You start post arrest hypothermia protocol and admit the patient to the medical intensive care unit (MICU).
Introduction
Hemoptysis is defined as the expectoration of blood originating from the tracheobronchial tree or lung parenchyma1. A common source of the bleeding is the bronchial artery1,2. Blood coming from other sources, including but not limited to the oral cavity, upper gastrointestinal (GI) tract, or esophagus can sometimes be mistaken for hemoptysis and is categorized as pseudohemoptysis. There are numerous causes of hemoptysis. Ong et al divides such etiologies into 5 main categories: infective, neoplastic, vascular, autoimmune, and drug/other related.
Examples of infectious causes include tuberculosis, lung abscesses, and pneumonia. Primary and metastatic cancer are examples of neoplastic causes. Pulmonary embolism is a vascular cause of hemoptysis. Lupus and various vasculitic diseases are examples of autoimmune causes of hemoptysis. Anticoagulants and trauma can cause hemoptysis as well1. According to a retrospective population based study conducted by Abdulmalak et al from 2008-2012, 15,000 adults were admitted for hemoptysis each year. The investigators found hemoptysis is associated with a 27% mortality at three years2.
There are two main categories of hemoptysis: massive and non-massive. The initial evaluation should try to focus on this differentiation. Most cases of hemoptysis are non-massive (95%) and self-limited3. Massive hemoptysis is described as a large enough volume of blood expectorated to cause hemodynamic instability, abnormal gas exchange, or a significant threat to life. According to Yoon et al, most deaths that occur secondary to massive hemoptysis are due to asphyxiation, rather than exanguination4. There is no consensus on the volume of blood that needs to be expectorated to be categorized as massive hemoptysis. Some reports define massive hemoptysis as expectorating >300 cc of blood in 24 hours5. Other sources have described massive hemoptysis as expectorating >100 to >1000 cc of blood in 24 hours4-6. With no clear definition on what volume of blood must be lost to meet the diagnosis of massive hemoptysis, the emergency physician must target his/her evaluation to determine the risk of death with the patient’s clinical presentation, regardless of how much blood is expectorated.
Key ED Work Up
For patients presenting with hemoptysis, the emergency medicine (EM) provider must determine whether it is massive or not and what etiology (infectious, vascular, etc) to suspect by history and physical examination. Laboratory work including a complete blood count, a basic metabolic panel, a type and screen (with cross if massive hemoptysis suspected), coagulation studies (particularly important in patients on anticoagulation) and a lactate level should be considered. Since patients with massive hemoptysis can decompensate quickly, the EM provider should not fall into a false sense of assurance if initial laboratory work and evaluation are normal. These patients should be monitored closely and labs repeated if there are signs of clinical deterioration.
Important imaging to consider includes chest radiograph and computed tomography (CT)7. Chest CT is needed in patients with history of tobacco use, age greater than 40 years, massive hemoptysis, and mass or infiltrate on radiograph. Bronchoscopy should be considered, as it can help to localize and control the source of bleeding by infusion of vasoactive drugs at the site of the bleeding. However, the performance of this procedure can be challenging secondary to a blood filled airway6-8.
Radiographs and CT can help locate the bleeding and possibly characterize an infectious, neoplastic, or other cause of the bleeding8-11. Table 1 summarizes a set of guidelines for imaging patients that present with hemoptysis.



Table 1: Imaging recommendations (Reproduced from Earwood et al. Am Fam Physician 2015)
Key ED Work Up: Non-Massive Hemoptysis
In patients determined to have pseudohemoptysis and/or non-massive hemoptysis, it may be appropriate to discharge these patients with follow up testing/imaging if indicated according to their history and physical (Figure 1). Patients should be hemodynamically stable with normal vital signs, have normal chest radiographs, possess no comorbidities, and have adequate follow-up. Repeat chest radiograph may be needed. Any concern for massive hemoptysis warrants admission for further evaluation and management.
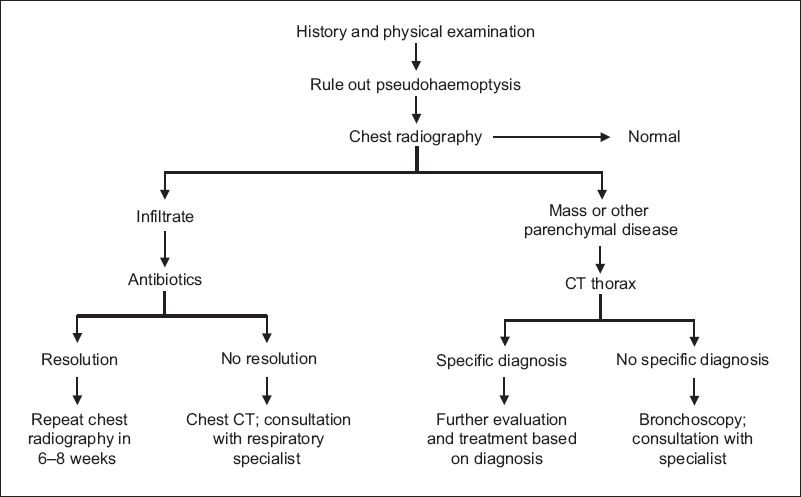
Figure 1: Evaluation of non-massive hemoptysis (Table reproduced from Ong et al. Singapore Med J 2015)
Key ED Work Up: Massive Hemoptysis
Massive hemoptysis requires immediate resuscitation with blood products, interventional radiology consultation (for bronchial artery embolization), and cardiothoracic surgery consultation. As mentioned in the introduction, asphyxiation is a cause of death in patients with hemoptysis. Early and aggressive airway management should be considered. When intubating, large (8.0) ET tubes are preferred, as smaller tubes, as well as double lumen tubes, can make bronchoscopy difficult. One should also consider the utility of selective mainstem bronchus intubation to isolate the side that is bleeding. One can accomplish this by placing the tube past the cords and then rotating the tube 90 degrees toward the side that one is trying to intubate13.
In patients on anticoagulation, reversal may be needed. Some medications to consider, depending on the specific anticoagulant, include prothrombin complex concentrate (PCC), TXA (tranexamic acid) vitamin K, fresh frozen plasma (FFP), and recombinant Factor VII14. For further information on reversal of anticoagulation please visit: http://www.emdocs.net/reversal-of-anticoagulation/. Blood products may be required.
In patients with massive hemoptysis, hemodynamic instability, or significant comorbidities, the emergency provider should consider admission for further workup. Inpatient workup may involve bronchoscopy, endovascular embolization, and/or surgery (Figure 2).

Figure 2: A management approach to massive hemoptysis (Image reproduced from Larici et al. Diagn Interv Radiol 2014)
Summary
-Hemoptysis is defined as expectoration of blood originating from the tracheobronchial tree or lung parenchyma and must be distinguished from pseudohemoptysis
-Hemoptysis is categorized as Massive or Non-massive
-There are many causes of hemoptysis and broad categories of these causes include: Infection, Autoimmune, Trauma, Drugs, and Neoplastic
-There is no consensus on the volume of expectorant that one must have to meet the diagnosis of massive hemoptysis
-Massive hemoptysis is life threatening, and, after securing the airway with intubation and maximizing hemodynamic stability with transfusion and reversal of anticoagulation, the patient should be admitted.
-Depending on the suspected etiology, definitive care may come in the form of bronchoscopy, bronchial artery embolization, and/or surgery
References / Further Reading
- Ong Z, Chai H, How C, Koh J, Low TB. A simplified approach to haemoptysis. Singapore Med J 2015; 57(8): 415-418.
- Abdulmalak C, Cottenet J, Beltramo G, Georges M, Camus P, Bonniaud P, et al. Haemoptysis in adults: a 5-year study using the French nationwide hospital administrative database. Eur Respir J 2015 Aug;46(2):50311.
- Larici AR, Franchi P, Occhipinti M, Contegiacomo A, Ciello A, Calandriello L, et al. Diagnosis and management of hemoptysis. Diagn Intervn Radiol 2014 Jul-Aug; 20(4):299-309.
- Yoon Woong, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and Nonbronchial Systemic Artery Embolization for Life-threatening Hemoptysis: A Comprehensive Review. Radiographics 2002 Nov-Dec;22(6):1395-409.
- Andersen PE. Imaging and interventional radiological treatment of hemoptysis. Acta Radiol 20016 Oct;47(8):780-92.
- Jean-Baptiste E. Clinical assessment and management of massive hemoptysis. Crit Care Med 2000;28:1642-1647.
- McGuinness G, Beacher JR, Harkin TJ, Garay SM, Rom WN, Naidich DP. Hemoptysis: 30 prospective high-resolution CT/bronchoscopic correlation. Chest 1994:105:1155-1162.
- Cahill BC, Ingabar DH. Massive hemoptysis: assessment and management. Clin Chest Med 1994; 15:147-167.
- Nadich DP, Funt S, Ettenger NA, Arranda C. Hemoptysis: CT—bronchoscopic correlations in 58 cases. Radiology 1990:357-362.
- Abal AT, Nair PC, Cherian J. Haemoptysis: aetiology, evaluation, and outcome—a prospective study in a third-world county. Respir Med 2001;95:548-552.
- Tak S, Ahluwalia G, Sharma SK, Mukhopadhya S, Pande JN. Haemoptysis in patients with a normal chest radiograph: bronchoscopy-CT correlation. Australas Radiol 1999; 43:451-455.
- Earwood JS, Thompson TD. Hemoptysis: Evaluation and Management. Am Fam Physician 2015 Feb 15;91(4):243-249.
- Bair AE, Doherty MJ, Harper R, Albertoson TE. An evaluation of a blond rotational technique for selective mainstem intubation. Acad Emerg Med 2004;11(10):1105-7.
- Sakr L, Dutau H. Massive Hemoptysis: An Update on the Role of Bronchoscopy in Diagnosis and Management. Respiration 2010;80:38-58.

2 thoughts on “Hemoptysis: Key principles and management”