Journal Feed Weekly Wrap-Up
- Oct 30th, 2021
- Clay Smith
- categories:
#1: Non-Operative Management for Acute Appendicitis
Spoon Feed
In shared decision making between patient and provider, it is reasonable to consider nonoperative treatment of acute uncomplicated appendicitis (lack of appendicolith, abscess, tumor, perforation, sepsis, hemodynamic instability, age <45) as a safe first-line alternative to appendectomy.
Why does this matter?
Acute appendicitis is the most common cause of emergency abdominal surgery, with an average lifetime risk of 7-8% peaking between ages 10-19 years old. In the case of untreated appendicitis, rupture, sepsis and death may occur. Traditionally, up to 80% of acute uncomplicated appendicitis has been treated with urgent appendectomy. Advantages and disadvantages of appendectomy versus antibiotic therapy alone should be considered, including work/family responsibility, schedule flexibility, travel plans, expenses, and patient comfort with intervention.
Can we avoid operative intervention?
Three large multicenter trials have evaluated operative versus non-op management of acute uncomplicated appendicitis: absence of appendicolith, abscess, tumor, phlegmon or perforation, or hemodynamic instability; and symptom onset <48 hours, appendiceal diameter <11mm, and WBC count <18,000.
-
APPAC trial: 530 adults evaluated at 5-year outcomes. 95% of adults who got antibiotics alone improved during hospitalization; 27% eventually underwent appendectomy within 1 year. There was a similar 5-year incidence of complications in patients who had urgent vs delayed appendectomy, with no increased risk of perforation. Patients who were treated non-operatively with antibiotics had lower median days of being unable to work or participate in normal activity when compared to patients who received appendectomy (7 vs 19 days).
-
CODA: 1552 adults with 90-day outcomes. Patients with appendicolith had higher rate of appendectomy within 90 days than patients without (41% vs 25%) as well as higher complications when treated with antibiotics only vs urgent appendectomy (14% vs 3%). Patients with acute uncomplicated appendicitis treated with antibiotics versus urgent appendectomy had fewer mean days of disability at 90 days (5 vs 8).
-
MWPSC: 1068 children at 1 year outcome. Initial response rate to antibiotics was 86%; 33% of these had appendectomy within 1 year. There were fewer median days that patients were unable to participate in normal work/activity in the antibiotic group vs appendectomy group (4 vs 7 days).
Antibiotics to cover aerobic gram negative and anaerobic bacteria (such as ertapenem or ceftriaxone with metronidazole) should be given to patients for both operative and non-operative intervention. Patients treated nonoperatively should continue antibiotics with metronidazole + third or fourth generation cephalosporin or fluoroquinolone for 7-10 days. Patient should be instructed on strict return precautions and should have further clinical evaluation within 24-48 hours. Indications for emergent appendectomy include, but are not limited to, diffuse peritonitis or sepsis and lack of improvement at 48 hours. Risk factors for delayed response to antibiotic treatment include presence of appendicolith on CT, extraluminal fluid or air, age >45 years old, fever, symptoms > 48 hours, and initial elevated inflammatory markers. In the absence of any complicating factors, a trial of non-operative management with antibiotics could be considered.
Source
Treatment of Acute Uncomplicated Appendicitis. N Engl J Med. 2021 Sep 16;385(12):1116-1123. doi: 10.1056/NEJMcp2107675.
#2: TOMAHAWK RCT – Immediate vs Delayed Angiography for Out-of-Hospital Cardiac Arrest
Spoon Feed
There was no significant difference in 30-day mortality between immediate vs delayed cardiac catheterization strategies for hemodynamically stable patients who were post-arrest without STEMI on post-ROSC ECG.
Why does this matter?
The prognosis for patients who have out-of-hospital cardiac arrest (OHCA) is poor, even for those who are successfully resuscitated. Acute myocardial infarction is a common cause of OHCA, but there has not been a demonstrated benefit for immediate cardiac catheterization in patients without STEMI. The TOMAHAWK trial was the second and largest randomized trial addressing the timing of coronary angiography in hemodynamically stable patients without ST-segment elevation following OHCA.
Rest well, interventionalists…
The TOMAHAWK trial expanded on the findings of the COACT trial (prior JF here) to include patients with shockable or non-shockable initial rhythm. Patients with STEMI, obvious extra-cardiac etiology of arrest, hemodynamic or electrical instability, or cardiogenic shock were excluded.
Patients in the immediate group had coronary angiography performed as soon as possible (median 2.9 hours post-arrest), and patients in the delayed group underwent angiography >24 hours post-arrest at the discretion of the treating clinician (62.2% of patients had cardiac catheterization). For the primary outcome of 30-day mortality (all-cause), there was no statistically significant difference between immediate and delayed group (54.0% in vs 46.0%; hazard ratio 1.28; 95% CI, 1.0 to 1.63, p=0.06). The composite secondary endpoint of death or severe neurologic deficit occurred more frequently in the immediate group [64.3% vs 55.6%, RR 1.16; 95% CI 1.00 to 1.34]. This raised an interesting hypothesis, but the results were not adjusted for multiple outcomes, so there wasn’t enough evidence to say that early angiography is harmful. There was not a significant difference in safety outcomes (bleeding, stroke, need for renal replacement therapy). Finally, brain injury was the most common cause of death, so poor neurologic prognosis may attenuate any potential mortality benefit for patients undergoing revascularization.
For post-OHCA patients with hemodynamic or electrical instability, or clinical evidence of evolving ischemia, I will continue to discuss potential benefits of cardiac catheterization with cardiology. However, ICU admission with delayed catheterization for hemodynamically stable patients without STEMI continues to be a reasonable strategy. The authors also report that culprit lesions were identified in only 40% of all patients undergoing angiography, so be sure to consider and treat other causes of cardiac arrest.
Source
Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N Engl J Med. 2021 Aug 29. doi: 10.1056/NEJMoa2101909. [Epub ahead of print].
Spoon Feed
Several ECG features can help differentiate ventricular tachycardia (VT) from supraventricular tachycardia (SVT) with aberrancy. When in doubt, assume wide complex tachycardia (WCT) is VT, especially for patients with history of coronary artery disease or structural heart disease.
Why does this matter?
When patients with wide complex tachycardia present for medical care, initial evaluation should focus on hemodynamic stability. All patients with hemodynamic instability should be managed with urgent electrical cardioversion. For patients who are stable, correct diagnosis of wide complex tachycardia will guide the appropriate management and disposition. However, differentiating ventricular tachycardia (VT) from supraventricular tachycardia (SVT) with aberrancy isn’t easy.
It’s shocking how complex the diagnosis of wide complex tachycardia can be…
This was a case report and review article in JAMA Internal Medicine focusing on the diagnostic approach to wide complex tachycardia. The authors described several ECG features that are strongly associated with ventricular tachycardia. In addition, they highlighted the importance of reviewing the patient’s medical history, as nearly 90% of patients with wide complex tachycardia and a history of myocardial infarction will be in ventricular tachycardia.
ECG factors associated with VT include:
-
AV dissociation (P waves marching through at a slower rate, capture beats, or fusion beats)
-
QRS positivity in lead aVR
-
QRS concordance throughout the precordium
-
QRS duration longer than 160 ms
-
A broad and notched intrinsic deflection (initial portion of the QRS)
An example ECG from the article showing VT and several features associated with VT is shown below.
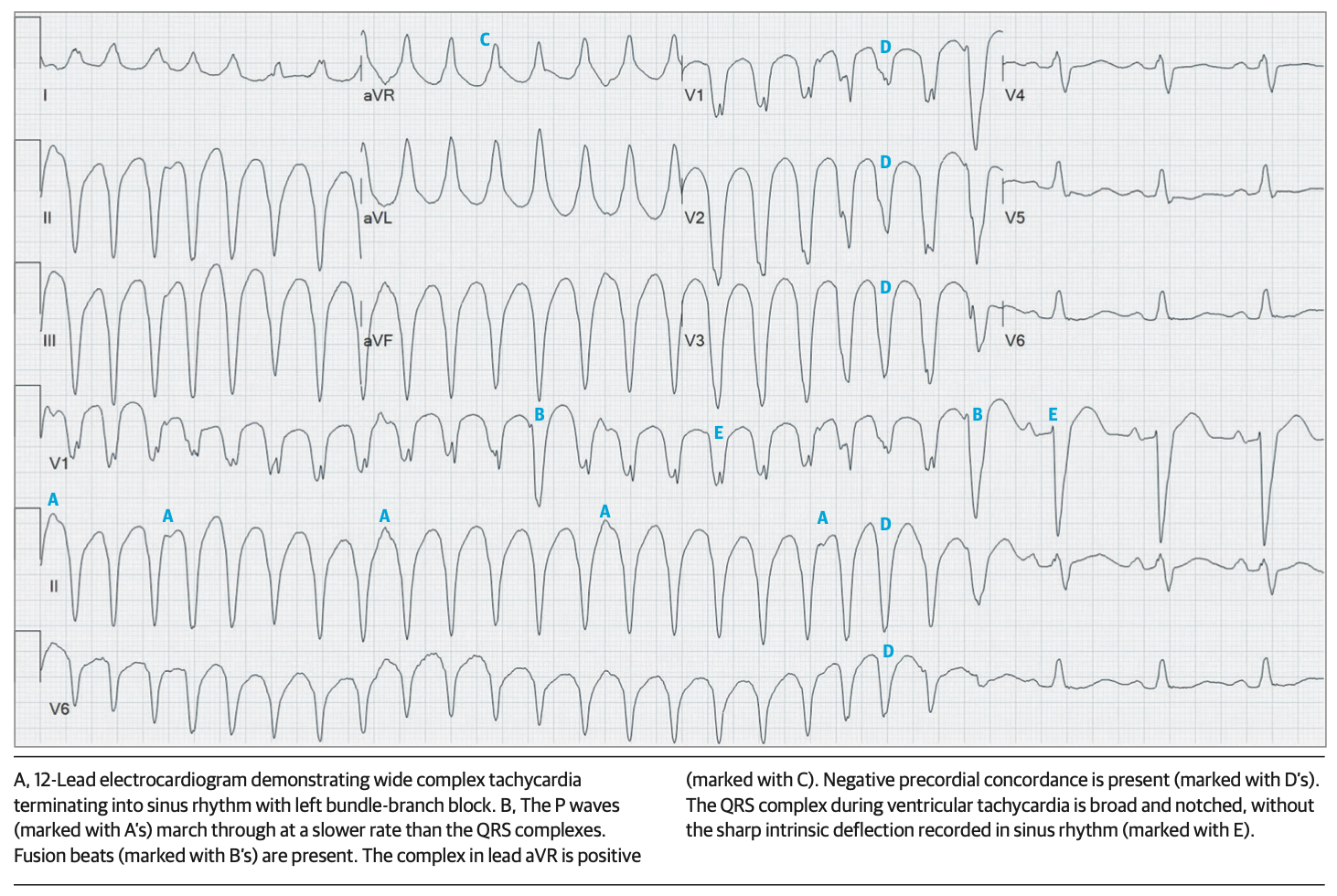
From cited article
These ECG features can help differentiate VT from SVT with aberrancy. However, when in doubt, err on the side of caution by assuming the patient is in VT, especially if the patient has a history of coronary artery disease or structural heart disease.
Source
Diagnostic Approach to Wide Complex Tachycardia. JAMA Intern Med. 2021 Sep 1;181(9):1231-1233. doi: 10.1001/jamainternmed.2021.3189
