Psoas Abscess: Pearls and Pitfalls
- Sep 4th, 2015
- Brit Long
- categories:
Author: Michele Callahan, MD (EM Resident Physician, University of Maryland Dept of Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
A 35 year-old male presents to your ED with a complaint of right flank pain that radiates into the hip region. His pain has been gradually worsening over the course of several days, with minimal response to motrin or tylenol. He can’t recall any trauma to the area. Review of systems is significant only for chills and increasing malaise over the past 1-2 weeks. He reports a past medical history of Crohn’s disease. The remainder of his history is unremarkable. On exam, the patient has pain with flexion of his right hip and ambulates with a limp. Bloodwork shows a WBC count of 11.2 x 109 L and a C-reactive protein of 300 mg/L. A CT scan is ordered and pending.
What is within your differential diagnosis for this patient’s symptoms?
Introduction
A psoas abscess (PA) is a retroperitoneal collection of purulent material involving the psoas muscle. These infections are classified as primary (resulting from hematogenous or lymphatic spread) or secondary (via direct spread or extension of nearby infection). Such nearby infections include diverticulitis, Crohn’s disease, spondylodiscitis, and appendicitis. The most common disease associated with secondary PA is Crohn’s disease.5
Epidemiology
Epidemiologic data is limited, as it is based on a small number of review articles relating to this topic. In a review of 367 cases by Ricci et al, it was found that over 99% of cases in Asia and Africa are primary, compared to 17% in Europe and 61% in North America.1 There is a male:female predominance of approximately 3:1, with involvement of the right psoas more common than the left7. In younger patients, the cause is more likely to be primary; secondary infections are more commonly seen in older patients.
When treated, mortality rates were found to be 2.4% in primary and 19% in secondary. Without treatment, these rates approach 100%.4
Patients who are predisposed to development of a psoas abscess include those with immunosuppression (HIV/AIDS), renal failure, IV drug abuse, diabetes, and instrumentation of the hip, flank, or groin.
Anatomy
The psoas major muscle is often grouped with the iliacus muscle, creating a muscle bundle referred to as the iliopsoas. These reside in the extra peritoneal space, taking off around the T12-L5 vertebrae. This muscle bundle extends downward and inserts in the lesser trochanter of the femur, acting as the primary flexor of the hip joint. Innervation of the psoas muscle is via the lumbar nerve roots of L1-L3, whereas the iliacus innervation comes from L2-L3 and the femoral nerve.4,5 The psoas muscle is prone to infection due to its rich vascular supply. Anatomically, its presence near intra-abdominal organs also makes it susceptible to spread from nearby infections.
Organisms involved
The most common organisms depend upon whether the infection is primary or secondary in nature. The leading cause is Staphylococcus aureus (accounting for up to 88% of primary PAs, and increasingly involving MRSA). Other infections commonly seen include Escherichia coli, Streptococcus spp, Bacteroides spp, Enterococcus faecalis, and Mycobacterium tuberculosis.4 In developing countries, vertebral osteomyelitis from tuberculosis is associated with development of a psoas abscess in 5% of cases.
Clinical Features
The presentation of these patients is often vague and nonspecific. The classic triad described by Mynter in 1881 includes abdominal or flank pain, fever, and limp. This triad is very rarely seen.6 Common complaints include fever, pain in the flank / abdomen / back / hip, pain with ambulation, limping, and malaise.
What else could it be?
The differential diagnosis of this condition is broad, as these patients often present with vague symptoms. A non-exhaustive list of alternate diagnoses to consider includes: appendicitis, renal colic, pyelonephritis, diverticulitis, appendicitis, sciatica, endometriosis, septic arthritis of the hip joint, abdominal aortic aneurysm, or muscle strain.
How to diagnose it
The biggest key to diagnosis of a psoas abscess is clinical suspicion. Although it can be useful to collect particular blood tests (CBC, ESR, CRP, blood cultures), ultimately the diagnosis will hinge upon clinical suspicion and findings on advanced imaging.
Physical exam maneuvers that may increase suspicion include pain with hip flexion, hyperextension, or external rotation. “Psoas sign” involves the examiner placing his/her hand just proximal to the knee and having the patient raise the thigh against this resistance – this maneuver is only 16% sensitive, but 95% specific.4 A tender mass palpable in the inguinal region may be appreciated. Needless to say, differentiation between hip pathology and psoas abscesses is difficult.
CT abdomen/pelvis with IV contrast is the standard test of choice for diagnosis. A CT scan showing a well-defined abscess collection is helpful for planning open or percutaneous drainage. To minimize radiation exposure, ultrasound may be attempted first – however, reported accuracy with use of ultrasonography in diagnosing psoas abscess is only 60%.7 In pregnant patients, US and MRI are preferred imaging modalities. MRI has higher sensitivity for detection when compared with CT scan, but is less readily available in most emergency departments.
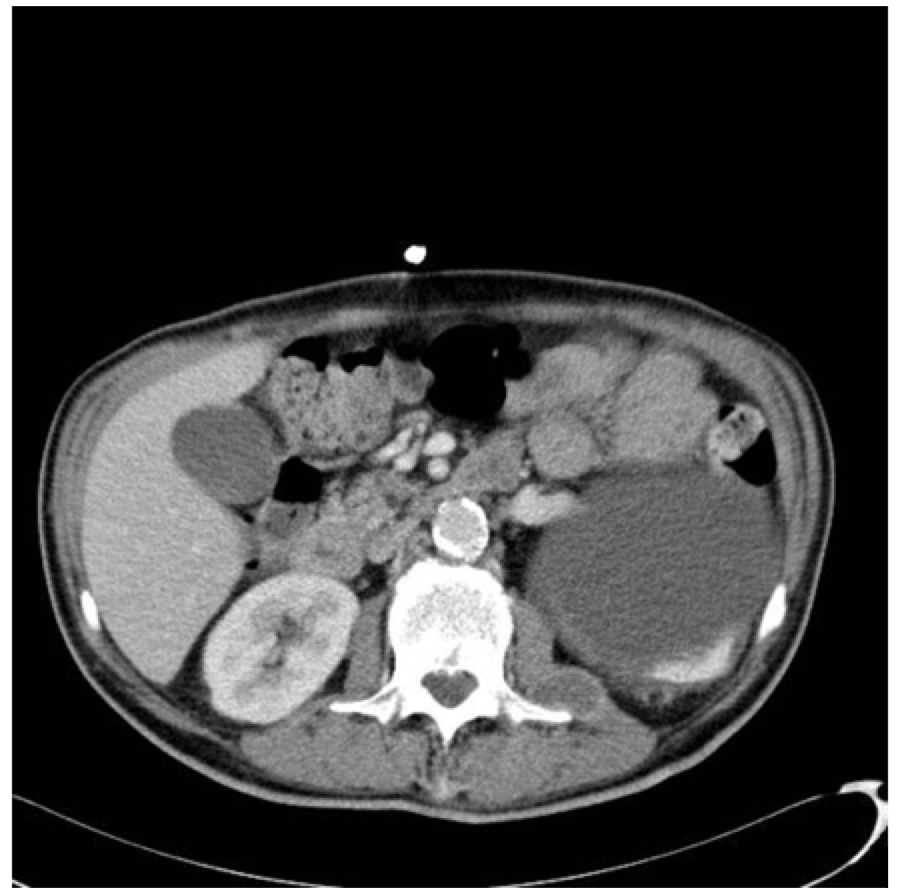
Case courtesy of Dr Jeremy Jones3: http://radiopaedia.org/cases/tuberculosis-with-psoas-abscess
So you’ve made the diagnosis – now what?
Once the diagnosis has been verified with CT scan or other advanced imaging, several steps should be taken. First, early involvement of your surgical / interventional radiology colleagues is paramount, as the ultimate treatment for psoas abscess is CT-guided percutaneous drainage +/- open drainage if unable to contain the infection with percutaneous techniques alone.
Initiation of broad-spectrum antibiotics with staphylococcal (MRSA if suspected) and enteric organism coverage is recommended – however, keep in mind that antibiotic coverage should be tailored to the presumed etiology of the patient’s illness. Obtaining blood cultures prior to the first dose of antibiotics can be useful to adjust antibiotic therapy later in the patient’s course. Culture and analysis of the abscess aspirate is more specific and produces higher yield. Ultimately, surgical intervention is the key.
Pearls
- Keep psoas abscess in your differential for patients with vague complaints, as mortality nears 100% when untreated.
- Patients predisposed to development of a psoas abscess include those who are immunocompromised (HIV, DM, IVDA, inflammatory conditions such as Crohn’s) as well as those with recent instrumentation of the groin or abdomen.
- Diagnosis requires clinical suspicion; CT scan can be useful to confirm the diagnosis and to guide surgical management.
- Cover patients with broad-spectrum antibiotics while they await treatment. Cultures of the blood can be useful, as are cultures from the abscess collection itself.
- The ultimate treatment is surgical drainage, either percutaneous or open.
Sources / Further Reading
1. Agrawal SN, Dwivedi AJ, Khan M. Primary psoas abscess. Dig Dis Sci2002;47:2103–5.
2. Dietrich A, Vaccarezza H, and Vaccaro CA. “Iliopsoas abscess: presentation, management, and outcomes,” Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, vol. 23, no. 1, pp. 45–48, 2013.
3. Hosn S. Psoas muscle abscess. Radiology Reference Article. Radiopaedia.org. Radiopaediaorg. 2015. Available at: http://radiopaedia.org/articles/psoas-muscle-abscess. Accessed May 21, 2015.
4. Mallick IH, Thoufeeq MH, Rajendran TP. Iliopsoas abscesses. Postgrad Med J. 2004;80:459–62.
5. Shields D, Robinson P, Crowley TP. “Iliopsoas abscess—a review and update on the literature,” International Journal of Surgery. 2012; 10(9): 466–469.
6. Tabrizian P, Nguyen SQ, Greenstein A, Rajhbeharrysingh U, Divino CM, “Management and treatment of iliopsoas abscess,” Archives of Surgery, vol. 144, no. 10, pp. 946–949, 2009.
7, Ricci MA, Rose FB, Meyer KK. Pyogenic psoas abscess: worldwide variations in etiology. World J Surg1986;10:834–43.
