Roc Rocks and Sux Sucks! Why Rocuronium is the Agent of Choice for RSI
- Dec 1st, 2014
- Anand Swaminathan
- categories:
Anand Swaminathan, MD, MPH (@EMSwami) is an assistant professor and assistant program director at the NYU/Bellevue Department of Emergency Medicine in New York City. Article edited by Reuben Strayer, MD and Alex Koyfman, MD.
I recently had the pleasure of engaging in a point-counterpoint discussion on the optimal agent for Rapid Sequence Intubation with Billy Mallon at Essentials of Emergency Medicine 2014. I took the pro-rocuronium side.
For decades, succinylcholine (suxamethonium) was the paralytic agent of choice (and the only available option) for RSI. The National Emergency Airway Registry (NEAR) found that it was used in 90% of airways. Succinylcholine has a number of perceived advantages that led to this situation:
- Rapid onset (45-60 seconds)
- Short half-life (6-8 minutes of paralysis)
Rapidly achieving an optimal intubating environment is critical as prolonged time to paralysis can delay successful intubation, potentially leading to oxygen desaturation. Early data demonstrated that succinylcholine reached optimal intubating parameters more rapidly than rocuronium (Sluga 2005, McCourt 1998, Laurin 2000). However, this difference was shown to be caused by inappropriate dosing of rocuronium (0.6 mg/kg in most studies). When a 1.2 mg/kg dose of rocuronium is given, the time to achieving optimal intubating parameters is virtually equivalent (Herbstritt 2012).
Rapid offset has been touted as an advantage because if the airway provider was unable to intubate the patient, the drug would wear off quickly and the patient would resume spontaneous breathing before desaturation occurs. We will see later why this logic is flawed.
Over the last 4-5 years, the RSI agent preference has swung away from succinylcholine.

There are likely numerous reasons for this swing including drug shortages but a better understanding of the limitations of succinylcholine are also likely at play.
Point #1 – Short paralysis time is not an advantage
I can imagine an argument for a short paralysis time in the operating room. Someone comes in for an elective procedure and you proceed with paralysis and induction. If you can’t intubate that patient, you wake him up, send him out of the OR and bring him back after you’ve constructed a new plan/approach to controlling the airway.
The ED is not the OR. Once you decide the patient needs to have their airway secured, you MUST secure the airway. Allowing the patient to wake up and breathe spontaneously isn’t an option for the vast majority of intubations.
Thus, we can see why rocuronium is the preferred agent. With rocuronium, the patient will be paralyzed for 30-45 minutes. If your first airway attempt fails, you will proceed down your airway algorithm ultimately ending with the surgical airway. Patients commonly require multiple intubation attempts with bag mask or LMA ventilation in between attempts. The return of muscle tone during the airway procedure is a precarious event making regurgitation and aspiration more likely. Additionally, the last thing you need is for the paralysis to wear off while you try alternate methods or worst of all, wear off when scalpel hits skin. A longer-acting paralytic affords us time to secure the airway even in the more difficult cases without sending a nurse scrambling for a second dose of succinylcholine. Finally, repeat doses of succinylcholine increase the risk of its adverse effects (masseter spasm, hyperkalemia).
Point #2 – Succinylcholine leads to more rapid oxygen desaturation than rocuronium
After giving a dose of succinylcholine, we watch for fasciculations. This signifies that the drug has taken effect. It also eats oxygen. A study by Taha et al demonstrated that succinylcholine led to oxygen desaturation 20 seconds faster than rocuronium (Taha 2010). A subsequent study of overweight patients revealed a 46 second difference in oxygen desaturation in favor of rocuronium (Tang 2011). That’s a lot of extra safe apneic time. The more time we are given, the more likely we are to succeed.
Point #3 – Succinylcholine has the potential to cause life-threatening hyperkalemia
Succinylcholine’s side effect of raising serum potassium is well-known and accepted. This small rise is typically trivial in most patients. However, in patients with certain underlying conditions, succinylcholine can cause life-threatening hyperkalemia leading to dysrhythmias and potentially, cardiac arrest.
Below is a slide from the Sydney Helicopter Emergency Medical Service (HEMS) regarding succinylcholine use:
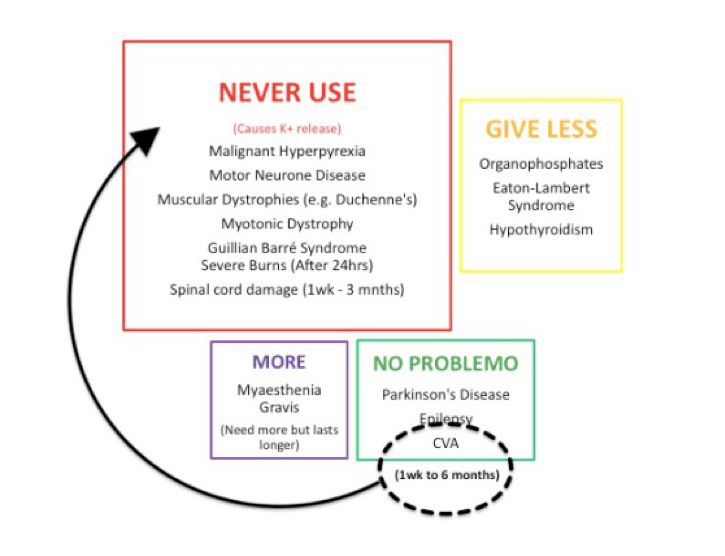
While these diseases are rare, they do exist and patients requiring intubation in the ED will often be unable to give a complete history. Additionally, these can be anxiety-provoking scenarios where simplicity is vital. It is likely that we as providers will not remember all of these contraindications in the heat of the moment.
Unlike succinylcholine, rocuronium does not cause a rise in potassium and has no contraindications to its use.
One of the main arguments to keep succinylcholine as the agent of choice is the neurocritical care intubation. The argument is that if the patient has a bleed, neurosurgery will want to examine the patient to decide whether or not they need to go to the operating room. Giving them rocuronium removes the ability to obtain an examination for 45-60 minutes.
This argument is unsound for a number of reasons. Firstly, you can get all the physical exam you need (pupillary response, motor response, verbal response) prior to intubation in a matter of seconds. Secondly, neurosurgeons are far more likely to take a patient to the operating room based on the CT scan than on the physical examination. Finally, rocuronium is neuroprotective. Hypoxia, while bad in all patients, is horrible in head bleeds. A single hypoxic event can double the risk of bad outcomes. Since succinylcholine leads to more rapid oxygen desaturation (Taha 2010, Tang 2011) the risk of a hypoxic event is increased. Additionally, spikes in intracranial pressure (ICP) can potentially worsen outcomes in these patients. Rocuronium prevents the patient bucking against the endotracheal tube during the early management when the patient is being agitated by procedures (central line, arterial line placement) and diagnostics (moving on/off the CT table). Patients should be covered with sedative agents while paralyzed, dosing may cause amnesia but not prevent all sensation and reflexes.
Summary Points
- In the ED, there is no scenario where a failed attempt at intubation leads to the patient waking up and breathing spontaneously. This isn’t the operating room. We must secure the airway.
- Succinylcholine-induced fasciculations leads to more rapid oxygen desaturation. Rocuronium buys you more safe apnea time.
- Succinylcholine can cause lethal hyperkalemia in patients with specific underlying diagnoses and is contraindicated for use in these circumstances. Patients requiring emergent airway management are unlikely to give you a complete history.
Special Thanks
Thanks to Haney Mallemat, Scott Weingart, Minh Le Cong and Reuben Strayer for helping in the creation of both this post and the debate at Essentials.
Read More
- Strayer RJ. Rocuronium versus succinylcholine: Cochrane synopsis reconsidered. Ann Emerg Med 2011; 58(2): 217-8.
- Strayer RJ. Rocuronium vs. succinylcholine revisited. Ann Emerge Med 2010; 39(3): 345-6.
- Mallon WK et al. Response to Rocuronium vs. succinylcholine revisited. Ann Emerge Med 2010; 39(3): 346-7.
- Strayer RJ. (2010, January 14). Screencast: Rocuronium vs. Succinylcholine in 8 minutes. Retrieved from http://emupdates.com/2010/01/14/rocuronium-vs-succinylcholine/
References
- Sluga M, Ummenhofer W, Studer W, Siegemund M, Marsch SC. Rocuronium versus succinylcholine for rapid sequence induction of anesthesia and endotracheal intubation: a prospective, randomized trial in emergent cases. Anesth Analg 2005; 101:1356 – 61.
- McCourt KC, Salmela L, Mirakhur RK, et al. Comparison of rocuronium and suxamethonium for use during rapid sequence induction of anaesthesia. Anaesthesia 1998;53:867–71.
- Laurin EG, Sakles JC, Panacek EA, Rantapaa AA, Redd J. A comparison of succinylcholine and rocuronium for rapid-sequence intubation of emergency department patients. Acad Emerg Med 2000;7:1362–9.
- Herbstritt A. BET 3: Is rocuronium as effective as succinylcholine at facilitating laryngoscopy during rapid sequence intubation. Emerg Med J 2012; 29(3): 256-9.
- Taha SK et al. Effect of suxamethonium vs rocuronium on onset of oxygen desaturation during apnoea following rapid sequence induction. Anaesthesia 2010; 65: 358-61.
- Tang L et al. Desaturation following rapid sequence induction using succinylcholine vs. rocuronium in overweight patients. Acta Anaesthesiol Scand 2011; 55: 203-8.

Great post! For an OR situation Sugammadex might come in handy if you encounter problems and need to reverse the effect.
Sugammadex is NOT available in the US at this time. It is NOT an option as suggested above. Also, there are several references to defasiculations occurring with succinylcholine. They are fasiculations. The muscles fasiculate. Defasiculation refers to administering a nondepolarizing muscle relaxant several minutes prior to the administration of a depolarizer (Anectine).
Jeff – excellent point on sugammedex and thank you for your correction regarding the fasciculations. We have updated the post regarding your correction.
We have been instructed to never use Roc in a seizure patient so that we will know if they are having seizures. Do you still use Roc in those patients?
Reuben Strayer has posted about this before- if you want to be able to tell if the patient is still seizing simply put a “finger tourniquet” on (the same you would use to sew up a finger lac to stop bleeding) before the roc is pushed. That way the finger will keep twitching if the patient is still seizing. If you don’t have that, in theory you could put a manual BP cuff on the patient’s forearm and pump it up above the patient’s systolic BP as another way of cutting off circulation. They use BP cuff tourniquets all the time in the OR for hours- 30-45 minutes until roc wears off won’t be a big deal.
This is a commonly asked question. Should we use Rocuronium in status epilepticus. I think you can as long as you make sure to give whopping sedative doses (typically propofol for me) to suppress seizure activity. Better still would be to get continuous EEG monitoring on the patient. The problem with using sux here is the same as above – more rapid desaturation, unknown contraindications.
All great reasons to use Roc in the emergency department. Obviously this article is focused on intubation in the ED. What are your thoughts about Succinylcholine vs Rocuronium in the pre-hospital setting?
I don’t practice prehospital so it’s probably not fair for me to really comment. I think if you do an exam (as much as you can) before intubation, there’s no reason not to use Sux prehospital. The flow diagram above is from Sydney HEMS so, clearly, they are behind roc.
I’ve mostly used succ, based on how long ago I trained. My general approach: I don’t care what the resident picks as long as they know the dose and the contraindications. We recently reviewed an article comparing roc vs succ in the ED and the drugs were equivalent in what matters the most: getting the tube in the right spot on first attempt (Patanwala etc al). I think most people get in trouble when they don’t use an adequate dose, regardless of which agent they choose. For me, regardless of history available, I look for AV fistulas, a wide QRS on the monitor, or signs of neuromuscular disease. Having used succ now for 19 years, I have only seen two cases of hyperkalemia that we obviously did not predict (or we would have picked something else). Right now, we are perhaps at 50% use of either agent at our place.