TXA Use in Trauma: An Update
- Dec 10th, 2014
- Brandon Busuito
- categories:
Author: Brandon C. Busuito, MD (EM Resident Physician, Henry Ford Hospital) // Editors: Justin Bright, MD and Alex Koyfman, MD (@EMHighAK)
As Emergency Physicians, we are always looking for ways to improve the care we provide to our patients. Based on clinical data which have come to light over the past several years, tranexamic acid (TXA) displays considerable promise toward reducing mortality in hemorrhagic trauma. It’s widely available, cost-effective, and an easy way to save lives. Let’s take a look at the evidence and discuss the potential benefit of TXA use in trauma.
BACKGROUND
Memorizing and understanding the coagulation cascade is a staple of medical school. However, as Dr. Tim Coats remarked during an EMCrit Podcast in 2012 while discussing his groundbreaking CRASH-2 Trial TXA work, our understanding may need some tweaking. “We were taught the coagulation system was a chain of events that happened to form a clot… that is entirely wrong.” He describes the process as much more dynamic, “Perhaps the way to think about it is like a modern fighter plane. There’s a sort of network, a web of controls that’s enabling that aircraft to fly. The coagulation system is exactly the same… a beautiful balance of the interaction between different molecules.”
Tranexamic acid was first described in 1966 and has been used over the past few decades in a wide variety of arenas to control hemorrhage resulting from dental procedures, reduce menstrual bleeding and alter intraoperative hemodynamics.1 Biochemically, TXA is a weak inhibitor of fibrinolysis, displacing plasminogen from fibrin and reducing plasmin activity. It acts to tip the balance of all those complex molecular interactions Dr. Coats described away from clot breakdown, but not so far as to create a theoretically hypercoagulable state.2
EVIDENCE
In 2010 the CRASH-2 trial was published in Lancet, showing a statistically significant mortality benefit using TXA early in the resuscitative effort. The study was groundbreaking not only for its impressive claim of reducing mortality in bleeding trauma by 1.5%, but also for its breadth as it encompassed over 20,000 patients in 274 hospitals spanning 40 countries.3
The double-blinded, randomized controlled trial included patients identified by treating physicians as a significant bleeding risk or already presenting with significant bleed. Significance was defined as a bleed causing a drop in systolic blood pressure below 90 mmHg, heart rate greater than 110 bpm or a bleed risk great enough that the clinician thought blood transfusion would likely be required. In practice, this latter part of the inclusion criteria was treated as synonymous with the question of whether to type and cross-screen a patient’s blood. The treatment arm included two stages, the first incorporating a 1g TXA bolus over ten minutes, typically in 100 mL of normal saline. This was followed by stage two, a 1g TXA drip over the following eight hours in 500 mL of normal saline.3
The authors concluded that their TXA treatment protocol resulted in a significant reduction in both all-cause mortality and risk of death due to bleeding by 1.5% and 0.8% respectively (p value 0.0035 and 0.0077) if administered within the first three hours of injury. Importantly, there was no evidence of increased thrombotic events (Table 1).3
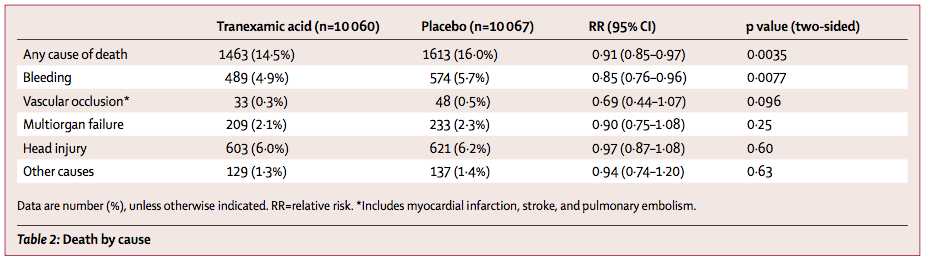
Table 1: CRASH-2 Trial, 2010. Death by cause.3
(click on table to enlarge)
This landmark trial showed great promise for the use of TXA in hemorrhagic trauma, but reproducibility was yet to be shown. The MATTERs trial, a retrospective observational study published in 2011 in Archives of Surgery by the US Army, sought to validate and expand the work done by the CRASH-2 collaborators, although slightly changing the dosage protocol. Nearly 900 consecutive combat trauma patients were examined, selected by those patients who received at least one unit of blood during the first 24 hours of presentation. Of these, 293 received a 1g dose of TXA in an IV fluid bolus. The study found a reduction in 48-hour mortality from 18.9% in the control group to 11.3% in the TXA group, a 7.6% reduction in mortality (p value 0.004) (Table 2).

Table 2: MATTERs Trial, 2011. All-cause mortality of Overall and Massive Transfusion Groups.4
The benefit held in 30-day mortality as well (Figure 1), and in a subgroup of patients treated with a massive transfusion protocol, the 48-hour mortality reduction improved to 13.1% (p value 0.003).4 Moreover, using the severity index defined in the MATTERs trial, the group receiving TXA scored higher on average, further emphasizing the benefit received by the treatment arm, an objectively sicker cohort of patients from the outset.

Figure 1: MATTERs Trial, 2011. Kaplan-Meyer survival curve of overall cohort (p value 0.006).4
DISCUSSION
Now, the conclusions purported by these two trials are not entirely bulletproof. The CRASH-2 trial excluded patients with primary traumatic brain injury, a large subset of emergency department populations, based on data from a 2003 study connecting TXA use with increased cerebral edema in subarachnoid hemorrhage.5 Of note, the CRASH-3 trial is currently ongoing, which will attempt to guide usage in this specific patient subset. In addition, the mortality benefit is entirely lost if TXA is given later than three hours after injury, with some experts arguing potential harm, although this was not significant in the CRASH-2 data.6 It should be noted that there is a paucity of data describing the effect of TXA in the presence of recombinant factor VIIa and therefore it is not recommended for concomitant use at this time.1 Curiously, the overall use of blood products does not diminish along with mortality, a phenomenon the authors explain by citing likely survivor bias.6
The MATTERs trial was equally groundbreaking, but was considerably limited both in patient diversity as well as follow-up data. The study was conducted over a twenty-four month period at one center in Afghanistan, limiting the socioeconomic generalizability of the results. Thrombotic events were also difficult to track outside of the immediate treatment phase simply due to the retrospective nature of the study and lack of baseline follow-up in this dynamic population.4
Despite these minor limitations, the case for use of TXA in acute hemorrhage is overwhelming. Taken together, recent data suggest a safe, inexpensive intervention at roughly 100 USD per gram.1 TXA is widely available and a relatively simple way to reduce mortality in trauma patients, with benefit increasing along the severity curve.7 The implementation conundrum remains, however, with the most convincing data now published over three years ago and anecdotal usage still strikingly low.
MOVING FORWARD
Awareness seems to remain the most troublesome obstacle. In the realm of clinical research, even with the most convincing, easy to implement interventions, adoption rates vary widely. The Institute for Healthcare Improvement published a review in 2000 estimating the average time to 50% implementation of landmark clinical trials to be in excess of 17 years. For instance, the flu vaccine had only reached 55% implementation in the general population in the year 2000 despite academic consensus of efficacy having been reached in the late 1960s.8 Of course, it would be patently unwise to implement new treatment protocols without also planning further study to determine consistent reproducibility, which is indeed ongoing in a variety of areas.
CRASH-2, and to a large extent MATTERs, present statistically sound, large-scale, generalizable studies which stand up to peer scrutiny. Although TXA is not yet FDA-approved for trauma, experts in military and civilian systems alike agree that the available data paint a picture of solid evidence which does not require further validation to begin implementing. In fact, the United States Military as well as Massachusetts General Hospital have already included TXA in their hemorrhagic trauma treatment protocols.1 And last year, Annals of Emergency Medicine published a policy paper recommending the use of TXA per CRASH-2 protocol in trauma patients at risk of significant hemorrhage without isolated traumatic brain injury.9
TXA TRAUMATIC HEMORRHAGE DOSAGE
________________________________________
• 1 g IV bolus in 100 mL NS within first 3 hours of incident
• 1 g IV in 500 mL NS over the following 8 hours
________________________________________
Contraindications: Primary head trauma, factor VIIa administration
Granted a less nimble practice environment, the civilian private sector will certainly take longer to adopt, but the Emergency Medicine fraternity is a small enough community that we can affect change by taking on the implementation responsibility ourselves.
Inquire with a pharmacist at your institution to determine availability. Start a conversation with colleagues. Review the evidence. TXA for traumatic hemorrhage is a simple way to reduce mortality, but implementation remains elusive.
References / Further Reading:
1. Cap AP, Baer DG, Orman JA, Aden J, Ryan K, Blackbourne LH. Tranexamic acid for trauma patients: a critical review of the literature. J Trauma. 2011 Jul;71(1 Suppl):S9-14. doi: 10.1097/TA.0b013e31822114af. Review. PubMed PMID: 21795884.
2. Roberts I, Shakur H, Ker K, Coats T; CRASH-2 Trial collaborators. Antifibrinolytic drugs for acute traumatic injury. Cochrane Database Syst Rev. 2011 Jan 19;(1):CD004896. doi: 10.1002/14651858.CD004896.pub3. Review. Update in: Cochrane Database Syst Rev. 2012;12:CD004896. PubMed PMID: 21249666.
3. CRASH-2 collaborators, Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, Dewan Y, Gando S, Guyatt G, Hunt BJ, Morales C, Perel P, Prieto-Merino D, Woolley T. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet. 2011 Mar 26;377(9771):1096-101, 1101.e1-2. doi: 10.1016/S0140-6736(11)60278-X. PubMed PMID: 21439633.
4. Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Arch Surg. 2012;147(2):113-119. doi:10.1001/archsurg.2011.287.
5. Roos YB, Rinkel GJ, Vermeulen M, Algra A, van Gijn J. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev. 2003:CD001245.
6. CRASH-2 trial collaborators, Shakur H, Roberts I, Bautista R, Caballero J, Coats T, Dewan Y, El-Sayed H, Gogichaishvili T, Gupta S, Herrera J, Hunt B, Iribhogbe P, Izurieta M, Khamis H, Komolafe E, Marrero MA, Mejía-Mantilla J, Miranda J, Morales C, Olaomi O, Olldashi F, Perel P, Peto R, Ramana PV, Ravi RR, Yutthakasemsunt S. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010 Jul 3;376(9734):23-32. doi: 10.1016/S0140-6736(10)60835-5. Epub 2010 Jun 14. PubMed PMID: 20554319.
7. Roberts I, Perel P, Prieto-Merino D, Shakur H, Coats T, Hunt BJ, Lecky F, Brohi K, Willett K; CRASH-2 Collaborators. Effect of tranexamic acid on mortality in patients with traumatic bleeding: prespecified analysis of data from randomised controlled trial. BMJ. 2012 Sep 11;345:e5839. doi: 10.1136/bmj.e5839. PubMed PMID: 22968527; PubMed Central PMCID: PMC3439642.
8. Balas, E. A., and S. A. Boren. “Review Paper: Managing Clinical Knowledge for Health Care Improvement.” Yearbook of Medical Informatics (2000): 65-70. Print.
9. J Harvey V, Perrone J, Kim P. Does the use of tranexamic acid improve trauma mortality? Ann Emerg Med. 2014 Apr;63(4):460-2. doi: 10.1016/j.annemergmed.2013.08.028. Epub 2013 Oct 3. Review. PubMed PMID: 24095056.
10. http://www.ncbi.nlm.nih.gov/pubmed/24155347
11. http://www.ncbi.nlm.nih.gov/pubmed/23967785
