Ultrasound for Confirmation of Endotracheal Tube Placement During CPR
- Feb 18th, 2016
- Stephen Alerhand
- categories:
Stephen Alerhand MD (Emergency Medicine Resident Physician, Icahn School of Medicine at Mount Sinai (@SAlerhand), Edited by Alex Koyfman MD (@EMHighAK)
Background
There are several ways to confirm correct placement of the endotracheal tube after intubation:
- Visualizing the tube passing through the vocal cords
- Fog within the endotracheal tube on expiration
- Auscultating bilateral breath sounds, absence of sounds in the epigastrum, and thoracic movement with respiration
- Endotracheal tube palpation in the neck or suprasternal notch
- Pulse oximetry
- Qualitative and/or quantitative end-tidal CO2 measurement
Quantitative end-tidal CO2 measurement is considered the best method at present to evaluate correct placement of the ET tube. It indirectly reflects real-time changes in CO2 production in the tissues, along with the circulatory system’s delivery of that CO2 to the lungs.
However, this method is less accurate in patients with decreased circulatory perfusion such as those in cardiac arrest, recent return of spontaneous circulation (ROSC), or other low-flow states. Simply put, the delivery of carbon dioxide to the lungs may not be sufficient. This issue may also present in: obese patients, those with air in the esophagus or stomach, and those with copious amounts of gastric or pulmonary secretions.
Let us present the following scenario in which all of the above confirmatory methods are utilized, but where their accuracy may be suboptimal. Then an additional confirmational adjunct for precisely these situations will be introduced as a useful tool in trained hands.
Scenario
The red phone arrives with a notification alert: “68 year-old male in cardiac arrest, ACLS performed for 15 minutes, ETA 5 minutes.”
The team leader assigns you to the airway role, and 5 minutes later the EMS team wheels the patient into the room.
The first things you notice: The patient is obese, chest compressions are in progress, and the patient has been intubated in the field. You next notice that there are some dark gastric secretions pooled up around the endotracheal tube.
Sequence of Actions
You take the following actions (as written above):
- You attach a quantitative end-tidal CO2 connector between the ETT and the BVM (or ventilator)
- However, as described above, the low-flow state of cardiac arrest limits this method’s reliability.
- You attach the pulse oximetry probe to the patient’s finger.
- However, you are not seeing a good waveform on the monitor, thus the number alongside the waveform is unreliable.
- You attach a qualitative colormetric end-tidal CO2 device between the ETT and the BVM (or ventilator).
- However, the device may turn from purple to yellow (end-tidal CO2 >2%) when contaminated by gastric secretions or other acidic substances, and may not function when clogged by secretions.
- You try using the video laryngscope to confirm correct placement of the ETT through the vocal cords.
- However, the patient’s body habitus and gastric secretions may this difficult.
- You look for fog within the ETT.
- However, the gastric secretions make this unreliable.
- You try to auscultate bilateral breath sounds, absence of sounds in the epigastrum, and thoracic movement with respiration.
- However, this is also made unreliable by the patient’s body habitus, as well as by the crowd of noisy providers circled around the patient performing chest compressions, attaching monitor leads, acquiring peripheral or central access, and/or administering medications.
- You try to feel for the ETT in the neck or suprasternal notch.
- However, the patient’s large neck makes this unreliable.
The team leader asks: “ Did you confirm the airway?”
You start to mumble and bumble, when suddenly your Ultrasound Fellowship-trained attending grabs the linear probe, sticks it on the patient’s neck, and within 15 seconds declares that the correct ETT placement is confirmed.
How did he do that? The attending states that the method is by no means perfect and certainly technically difficult, but that with enough practice and repetition he has been able to harness US as a helpful tool for similar situations as the one presented.
Using Ultrasound to Confirm Proper ETT Placement
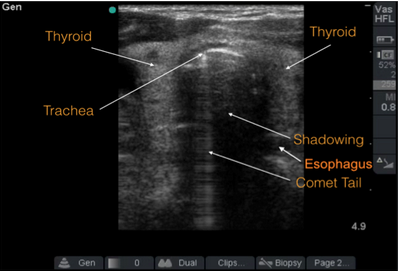
- Gently place the high-frequency linear probe just superior to the suprasternal notch in the transverse plane.
- The trachea will appear as a hyperechoic curvilinear structure with shadowing. A comet tail, or reverberation rings, appear deep to that structure.

- The esophagus will appear distally and to the right. It has a hyperechoic wall and hypoechoic center.
- Tracheal intubation: Visualize the second hyperechoic curvilenar structure within the trachea. You can also gently shake the ETT and visualize tracheal movement on the screen. Using Doppler, a color ray will also appear within the trachea.

- Esophageal intubation: The “double tract sign” (in which there seemingly appears to be two tracheas) indicates esophageal intubation.

- Pitfall: If the esophagus is anatomically located just posterior to the trachea, then the trachea’s shadowing may obscure an esophageal intubation.
Supporting Literature
Chou EH, Dickman E, Tsou PY, et al. Ultrasonography for confirmation of endotracheal tube placement: a systematic review and meta-analysis. Resuscitation. 2015 May;90:97-103.
Objective: To summarize evidence of diagnostic value of US for assessment of ETT placement in adults.
Design: Meta-analysis
Results: 12 studies. In detecting esophageal intubation, pooled sensitivity 0.93 (95% CI 0.86-0.96) and specificity 0.97 (95% CI 0.95-0.98).
Conclusions: Current evidence shows US has high diagnostic value for identifying esophageal intubation, especially when capnography may be unavailable.
Chou HC, Chong KM, Sim SS, et al. Real-time ultrasonography for confirmation of endotracheal tube placement during cardiopulmonary resuscitation. Resuscitation. 2013 Dec;84(12): 1708-12.
Objective: To evaluate accuracy of tracheal US for assessing ETT position during CPR.
Design: Prospective observational study. Gold standard of correct ETI was combination of clinical auscultation and quantitative waveform capnography.
Results: n=89 patients. 7 had esophageal intubation. Sensitivity of tracheal ultrasonography 100% (95% CI 94.4-100), specificity 85.7% (42.0-99.2), positive predictive value 98.8% (92.5-99.0), negative predictive value 100% (54.7-100).
Conclusions: Real-time tracheal US is accurate for identifying ETT position during CPR without need for interruption of chest compressions. Tracheal US in resuscitation may serve as powerful adjunct in trained hands.
Das SK, Choupoo NS, Haldar R, Lakhar A. Transtracheal ultrasound for verification of endotracheal tube placement: a systematic review and meta-analysis. Can J Anaesth. 2015 Apr;62(4):413-23.
Objective: To evaluate diagnostic accuracy of transtracheal US in detecting ETI.
Design: Meta-analysis
Results: 11 studies, 969 intubations. Pooled sensitivity 0.98 (95% CI 0.97-0.99), specificity 0.98 (95% CI 0.95-0.99). In emergency situations, those values were 0.98 (95% CI 0.97-0.99) and 0.94 (95% CI 0.86-0.98).
Conclusions: Transtracheal US is useful for confirming ETI with acceptable sensitivity/specificity. Can be used in emergency situations as preliminary test before final confirmation by capnography.
Gottlieb M, Bailitz JM, Christian E. et al. Accuracy of novel ultrasound technique for confirmation of endotracheal intubation by expert and novice emergency physicians. West J Emerg Med. 2014 Nov;15(7):834-9.
Objective: To evaluate the accuracy of a novel, simplified, 4-step (4S) technique (see article for steps)
Design: Blind, randomized trial of 4S technique sing adult cadaver, randomized to tracheal or esophageal intubation. Three experts and 45 residents performed 150 scans.
Results: Experts had sensitivity 100% (95% CI 72-100) and specificity 100% (77-100) on thin cadavers, 93% (66-100) and 100% (75-100) on obese cadavers. Residents had sensitivity 91% (69-98) and specificity 96% (76-100) on thin cadavers, 100% (82-100) and 48% (27-69) on obese cadavers. Overall mean time to detection of 17 seconds (13-20) for experts and 29 seconds (25-33) for residents. Statistically significant decrease in specificity on obese cadavers between residents and experts, as well as increased time to detection for residents.
Conclusions: The simplified 4S technique was accurate and rapid for US experts. Among residents, the 4S technique was accurate in thin cadavers, less so in obese cadavers.
Abbasi S, Farsi D, Zare MA, et al. Direct ultrasound methods: a confirmatory technique for proper endotracheal intubation in the emergency department. Eur J Emerg Med. 2015 Feb;22(1):10-6.
Objective: To assess diagnostic accuracy of US for detection of proper ETT placement.
Design: Prospective study. Two phases: 1) dynamic: as intubation being performed 2) static: after intubation.
Results: n=60 patients. For dynamic phase, sensitivity for determining correct ETI 98.1% (95% CI 88.8-99.9), specificity 99% (51.6-100), positive predictive value 100% (91.5-100), negative predictive value 85.7% (42-99.2%). For static phase, all testing characteristics were 100%.
Conclusions: Acceptable sensitivity, specificity, positive predictive value, and negative predictive value for prediction of tracheal ETT placement with use of dynamic and static US.
Chenkin J, McCartney CJ, Jelic T, et al.. Defining the learning curve of point-of-care ultrasound for confirming endotracheal tube placement by emergency physicians. Crit Ultrasound J. 2015 Dec 7(1):14.
Objective: To determine amount of practice required by ED docs to develop proficiency at interpreting clips of tracheal and esophageal intubations.
Methods: Physicians and residents completed a baseline interpretation test, then a 10-minute tutorial. They then took 10-question tests.
Results: n=66. Means core on baseline test: 42.9% (SD 32.7%). After tutorial, 90.9% answered all ten questions correctly after one attempt, 100% after two attempts. Sensitivity of 98.3% and specificity of 100% for detecting correct ETT location.
Conclusions: After brief online tutorial and only two practice attempts, physicians quickly and accurately interpreted US intubation clips of esophageal and endotracheal intubations.
Additional References
Chao A, Gharahbaghian L. http://www.acep.org/Content.aspx?ID=102309
Galvagno , SM. Kodali, BS. Capnography educational website. Use of Capnography in Emergency Medicine and Prehospital Critical Care. http://www.capnography.com/Emrmedicine/capnographyinemergencymedicine.htm
O’Conner RE, Swor RA. Verification of Endotracheal Tube Placement Following Intubation. National Association of EMS Physicians, 1999.
https://www.acep.org/Clinical—Practice-Management/Verification-of-Endotracheal-Tube-Placement/

{kind=link}
Have any studies looked at filling the cuff with a bit of saline in order to assess for placement with ultrasound? I recalled this being mentioned at a recent ultrasound course. Is there more potential for harm with damage to the trachea or larynx with overfilling?