Ultrasound G.E.L. – Transcranial Doppler in Traumatic Brain Injury
- Feb 18th, 2022
- Michael Prats
- categories:
Originally published on Ultrasound G.E.L. on 3/1/21 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!
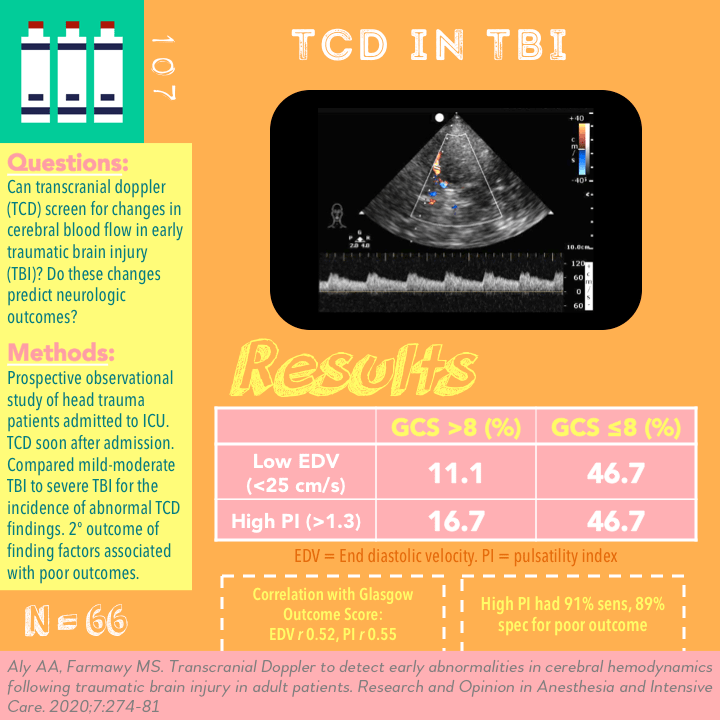
Transcranial Doppler to detect early abnormalities in cerebral hemodynamics following traumatic brain injury in adult patients
Research and Opinion in Anesthesia & Intensive Care Sept 2020 – Journal site Link
Take Home Points
1. TCD is a feasible noninvasive method to obtain information about cerebral blood flow in the setting of traumatic brain injury.
2. A low EDV or a high PI are more common in patients with severe TBI compared to mild to moderate TBI. This likely indicates pathologic cerebral blood flow and these findings correlate with worse neurologic outcomes.
3. More research is needed to determine if this is merely prognostic or if there are treatment implications for these findings.
Background
Transcranial doppler (TCD) has been a mainstay of care in the neuro ICU for decades. One of the primary uses of TCD has been evaluating for vasospasm in stroke and head injured patients. Previously this has been done via continuous doppler and typically executed by neurosonographers. In pediatric patients this was and still is used to assess normal anatomy, ventricle size, midline shift, and for intracranial hemorrhage. In recent years TCD has become used by a wider array of providers. In addition, the applications have grown significantly. TCD is being applied to estimating intracranial pressure, cerebral perfusion, brain death, brain injury, venous thromboembolic disease and concussion.
Questions
Can TCD screen for abnormalities in CBF in the early period following TBI?
Can early changes in CBF velocity be used to predict neurologic outcome ?
Population
Single center in Egypt
Inclusion
- Adults admitted to ICU
- less than 8 hours since diagnosis of TBI
Exclusion:
- Poor windows
- Arrhythmia or valvular stenosis
- Cardiac arrest
- Organ failure
- Polytrauma
For all patients they used arterial lines to keep MAP >90 CPP> 60
Design
Prospective Observational
Patient came in with head trauma, admitted to ICU
Got TCD by ICU provider “after resuscitation” (turned out this was about 50 minutes after admission which was close to 5 hours from their injury)
Measured TCD and carotid indices (see protocol below)
Grouped patients by severity using Glasgow Coma Score (GCS) into >8 (mild-moderate TBI) and ≤8 (severe TBI).
They followed these patients for outcome as measured by Glasgow Outcome Scale (GOS).
Primary outcome (not explicitly stated) appeared to be comparing the incidence of abnormal TCD findings between these two groups.
Secondary outcome was performing logistic regression analysis to see what factors (including TCD) correlated with poor outcomes (as measured by GOS)
They report a power analysis was performed but did not specify the number or if it was met by study enrollment.
Who did the ultrasounds?
“Experienced ICU staff members”
Each individual patient always had the same provider doing their TCD (to avoid variability)
The Scan
2MHz Phased array

Temporal window
2 measurements daily in first 72 hours
Daily until 7 days after TBI or discharge from ICU
Additional TCD if deterioration in neuro status
Key Terms:
MCA- middle cerebral artery
ICA – internal carotid artery
EDV – end diastolic velocity
dVF – diastolic flow velocity, seems interchangeable with EDV
PSV – peak systolic velocity
mFV – mean flow velocity. mFV = (PSV+ 2 x EDV)/3
PI – pulsatility index. PI = PSV-EDV/mFV
LR – Lindegaard ratio. LR = (mFV in MCA)/(mFV in ICA)
CPP – cerebral perfusion pressure. Calculated as CPP = MAP x EDV/mFV + 14
ICP – intracranial pressure. ICP = MAP – CPP
Link to article image of some of these measurements]
Great video from Western Sono on Point-of-care TCD
Study Protocol
Bilateral MCAs, ICA
Measurements:
- 10 cardiac cycles
- EDSV, PSV, mGV
- Used worst value
Calculated PI ( PSV-EDV/ mFV)
Lindegaard Ratio (MCA/ICA)
PI >1.3 considered abnormal
EDV< 25 cm/s considered abnormal
mFV in MCA >120 cm/s + LR > 3 = vasospasm
Learn how to do Transcranial Doppler 5 Minute Sono!


Results
n = 66 patients ( 42M, 22F)
Mean age 32 ( important that all are below 60 because normal range changes with age)
- 54.5% GCS > 8
- 45.5% GCS ≤ 8
- TCD performed within an hour ( 48 +/-18)
Primary Outcome
EDV higher in GCS > 8 group (37.8 vs 22.5 cm/s)
PI lower in GCS > 8 (1.02 vs 1.76)
More patients in GCS ≤8 group had low EDV (<25 cm/s) – 46.7% vs 11.1%
More patients in GCS ≤8 group had high PI (>1.3) – 46.7% vs 16.7%
LR and vasospasm also more in GCS ≤8 group but not statistically significant.
LR lower but not significant
Overall initial mVF higher in both groups on admission
Secondary Outcomes
Correlations with GOS (correlation coefficient r)
- Admission GCS 0.48
- EDV 0.52
- mFV 0.23
- PI 0.55
- Lindegaard ratio 0.18
Logistic Regression Analysis – Predictors of Poor Outcome (GOS 1-3)
Admission GCS ≤8
- Sensitivity 80%
- Specificity 72%
Initial EDV < 25 cm/s
- Sensitivity 88%
- Specificity 85%
Initial PI >1.3
- Sensitivity 91%
- Specificity 89%
Vasospasm
- Sensitivity 84%
- Specificity 75%
Strengths
Prospective
Good weighting of groups
Novel application
Achieved TCD early in course which was in line with objectives
Limitations
Fairly small study
Unclear exactly who was acquiring images and what training they had
Angle dependent measurements
As an prediction of early neurologic outcome, this TCD measurement may be too soon and patient could improve after this initial determination
Discussion
Good idea, consistent with prior data
Not useful in acute setting necessarily however often we are having this discussion with families so perhaps one more piece of data that can help with prognostication.
Check out a related application. An interesting study using TCD ins prehospital setting to guide treatment for increased intracranial pressure from traumatic injury! There is sure to more coming for TCD!
Summary
This is a prospective observational study out of Egypt in an ICU setting. 66 patients with TBI were enrolled. End diastolic velocity (EDV) and pulsatility index (PI) were more commonly abnormal in the group with severe TBI. On regression analysis, these measurements correlate with worse neurologic outcomes.
Take Home Points
1. TCD is a feasible noninvasive method to obtain information about cerebral blood flow in the setting of traumatic brain injury.
2. A low EDV or a high PI are more common in patients with severe TBI compared to mild to moderate TBI. This likely indicates pathologic cerebral blood flow and these findings correlate with worse neurologic outcomes.
3. More research is needed to determine if this is merely prognostic or if there are treatment implications for these findings.
More Great FOAMed on This Topic
Thinking Critical Care – TCD in the ED?
Our score

Expert Reviewer for this Post

Rachel Liu, MD @RubbleEM
Assistant Professor, Emergency Ultrasound Fellowship Director, and Director of Clinical Ultrasound Education for Yale School of Medicine
Reviewer’s Comments
Good study. Would be nice to know usefulness to an ED population, doesn’t seem like it has much application as there are no absolutely urgent interventions in their 4 hours pending transfer to ICU. It would have been interesting if they correlated PI, LR in both groups with ultimate GOS numbers. They hint at it in table 4. Also would have been interesting to know how long it took the operator to perform each exam.
Cite this post as
Creagh Boulger. Transcranial Doppler in Traumatic Brain Injury. Ultrasound G.E.L. Podcast Blog. Published on March 1, 2021. Accessed on February 18, 2022. Available at https://www.ultrasoundgel.org/107.
