The Crashing Patient with Long Bone Fractures: A Case of Fat Embolism Syndrome
- Jan 21st, 2016
- Molly L. Tolins
- categories:
Authors: Molly L. Tolins, MD and Nick Johnson, MD (University of Washington Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD (@SAlerhand)
Overview:
- When to suspect fat embolism syndrome (FES)
- Diagnosis of FES and further workup
- Pathophysiology of the syndrome
- Management of the critical patient with suspected FES
- Prognosis
Case Scenario
A 20-year-old man is brought in by medics after jumping from an overpass in a suicide attempt. Paramedics report obvious deformities of his bilateral lower extremities. He arrives with intact ABC’s and normal hemodynamics. Plain films demonstrate bilateral mid-shaft femur fractures and a left tibial shaft fracture; pan-scan demonstrates no other injuries. He is placed in bilateral distal femoral traction with a left long-leg splint and admitted to Orthopedics. While awaiting an inpatient bed after fracture manipulation, he suddenly develops tachycardia to 140 beats per minute, hypoxemia to 80% on ambient air, fever to 38.2, and decreased level of consciousness. He is intubated with improvement of hypoxemia, but he remains obtunded with extensor posturing to noxious stimuli and a fixed rightward gaze. CT head reveals no pathology. What are the next steps in this patient’s workup and management? What should be your primary diagnostic concerns in this trauma patient?
What’s going on?
The differential in the polytrauma patient with a sudden alteration in level of consciousness is broad. Intracranial hemorrhage, hemorrhagic shock, air embolism, cerebrovascular accident, hypoxemia or hypercarbia, carotid or vertebral dissection, profound electrolyte or acid-base disturbance, drug or alcohol intoxication, and a myriad of other potential catastrophic complications must be considered. In our patient, however, the constellation of long bone fractures, sudden hypoxemic respiratory failure, and focal neurologic findings suggested a specific etiology: fat embolism syndrome (FES).
FES Overview
- FES is a rare phenomenon associated with long bone fractures of the lower extremities, typically occurring between 30 minutes and 48 hours post injury.1
- Fat emboli can be detected in the lungs in up to 90% of individuals with long-bone fractures, but FES occurs in only 0.5-2.2% of these patients.1
- Gurd’s criteria most common for diagnosis, requiring 1 of 3 major criteria and 4 minor criteria.2 (Table 1)
- Continuous pulse oximetry may aid in recognition and diagnosis.
Table 1. Gurd’s Diagnostic Criteria for Fat Embolism Syndrome*
| Major Criteria | Minor Criteria |
| ● Petechial Rash● Respiratory symptoms with radiographic changes● Central nervous system signs unrelated to trauma or other condition | ● Tachycardia● Pyrexia● Retinal Changes (fat, petechiae)● Renal Abnormalities (oliguria, anuria, lipiduria)● Acute thrombocytopenia
● Acute decrease in hemoglobin ● High erythrocyte sedimentation rate ● Fat globules in sputum |
*Diagnosis requires 1 major and 4 minor criteria.
Further Testing
- There is no gold standard test; FES is a clinical diagnosis.
- Chest radiograph and CT often show nonspecific bilateral patchy opacities.
- MRI brain often shows “star-field” pattern of diffuse, punctate, hyperintense lesions on diffusion-weighted imaging.2 (Fig 1)
- Fundoscopy may show Purtscher-like retinopathy, with cotton wool spots, hemorrhages, and retinal edema.2
- Transcranial dopplers (TCD’s) can be used for microemboli monitoring; the finding of numerous bilateral microemboli is supportive of the diagnosis of FES.3
In our patient, no rash was seen, but both respiratory symptoms and neurologic signs were present. Additionally, he became tachycardic, febrile, and repeat labs demonstrated acute anemia and thrombocytopenia, meeting 2 major and 4 minor of Gurd’s criteria. MRI brain stroke protocol revealed a “star-field” pattern of innumerable, diffuse, punctate lesions consistent with cerebral FES (Fig 1).
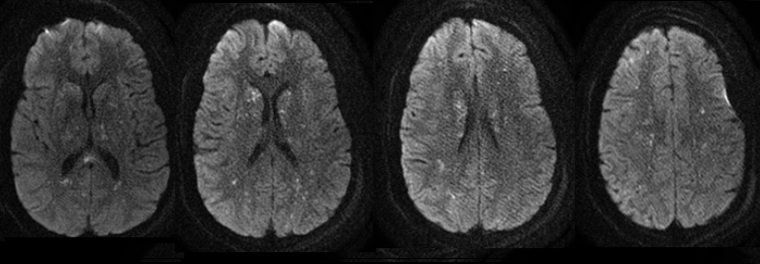
Figure 1. Brain MRI with Axial DWI cuts demonstrating scattered diffusion-restricted lesions predominantly involving the supratentorial cerebrum.

Figure 2: Just to get an idea…An example of a brain pathology sample suggesting FES
(http://library.med.utah.edu/WebPath/CNSHTML/CNS113.html)
Pathophysiology
- Intramedullary pressure and mobilization of fat globules by mechanical forces into adjacent damaged venous sinuses leads to venous emboli; due to their small size, fluidity, and deformability, a percentage of fat globules are able to pass through the pulmonary capillaries and enter the systemic arterial circulation.3,4
- While intrapulmonary or intracardiac shunts are not necessary for the syndrome to occur, their presence increases burden of disease.3,4
- Fat emboli cause both pulmonary and cerebral vasculature occlusion and local inflammation. Generalized intravascular lipolysis and a systemic inflammatory reaction may contribute to cerebral vascular injury.3,4
- In the lungs, mechanical obstruction leads to increased dead space, and inflammation may cause shunt and hypoxemia. Severe cases may cause pulmonary hypertension and acute cor pulmonale.5
Management
- Treatment is generally supportive.
- Other treatable causes of neurological decline such as diffuse edema, contusions, or herniation should be ruled out.
- Most are hypovolemic and require volume resuscitation.
- Supplemental oxygen or ventilatory support are often needed.
- Early operative fixation has been shown to reduce the incidence and severity of FES.6
- Patients usually require ICU management for close neurologic monitoring and respiratory support.
- Cerebral edema can ensue. In the case of asymmetric cerebral involvement, midline shift requiring neurosurgical decompression has been described. Signs of impending herniation should prompt a head CT and neurosurgical consultation, and intracranial pressure monitoring should be considered.4
- Case reports describe the use of extracorporeal membrane oxygenation in the management of catastrophic FES.7
Pharmacologic interventions remain controversial. Some randomized controlled trials have suggested the use of steroids to both prevent and treat FES, but there have been no large conclusive studies.8,9 High dose statin use as adjunctive treatment in FES has been described in a case report, mainly for its anti-inflammatory effects.3 However, further studies are necessary to repeat these findings. Heparin has been found helpful in animal models, but as most FES patients are poly-traumatized and minimal benefit with significant risks have been shown with anticoagulation, it is no longer recommended in clinical practice.3
Prognosis
- In a review of literature from 1980 to 2012, Kellogg et al. found 54 cases of FES with cerebral involvement.4
- Of these patients, a good outcome (intact or mild disability) was seen in 57.6% of patients with coma and/or abnormal posturing on presentation, and in 90.5% of patients with mild mental status changes, focal deficits, or seizure.3
- Overall, as many as 3-8% of FES patients will die.8
- Recovery is often delayed by weeks to months, but because the pathophysiology is thought to include inflammation rather than solely neuronal death, a much higher chance of recovery has been seen than in comparable ischemic lesions.4
Case outcome
Our patient was admitted to the ICU. Fundoscopy demonstrated Purtscher-like retinopathy, and echocardiogram demonstrated a patent foramen ovale. A high dose statin was initiated as adjunctive therapy for ongoing microemboli seen by transcranial Doppler. Over the next 2 days, the number of microemboli observed decreased to zero. Percutaneous tracheostomy was performed for ongoing depressed mental status and airway protection. Over time his neurologic exam improved, with resolution of posturing and increasing spontaneous movement, but at the time of this report, he remained mechanically ventilated for airway protection.
Key points
- FES is a clinical diagnosis; it should be suspected in the long bone fracture patient with respiratory symptoms, altered level of consciousness, or petechial rash.
- It can occur within hours of trauma, and while manipulation or operative management increase risk, FES can occur in the absence of any intervention.
- Gurd’s criteria are the most frequently used clinical criteria for diagnosis; major criteria include petechial rash, respiratory signs/symptoms, and CNS signs/symptoms.
- Adjunct diagnostics include fundoscopy with Purtscher-like retinopathy, chest radiograph or CT chest with ground-glass or diffuse opacities, MRI with diffusion-weighted imaging with “starfield” pattern, and transcranial Doppler with numerous microemboli.
- Treatment is largely supportive, and might include respiratory support, volume resuscitation, and fracture management, with close monitoring for increased ICP.
- Unlike other stroke patients, those with FES may make dramatic improvements despite poor initial neurologic status.
References/Further Reading
- Bulger EM, Smith DG, Maier RV, Jurkovich GJ. Fat embolism syndrome. A 10-year review. Arch Surg. 1997;132:435-439.
- Kosova E, Bergmark B, Piazza G. Fat embolism syndrome. Circulation 2015;131(3):317-20. PMID: 25601951
- Whalen LD1, Khot SP2, Standage SW. High-dose rosuvastatin treatment for multifocal stroke in trauma-induced cerebral fat embolism syndrome: a case report. Pediatr Neurol. 2014 Sep;51(3):410-3. doi: 10.1016/j.pediatrneurol.2014.04.025.
- Kellogg RG, Fontes RBV, Lopes DK. Massive cerebral involvement in fat embolism syndrome and intracranial pressure management. August 16, 2013; DOI: 10.3171/2013.7.JNS13363.
- Shaikh N. Emergency management of fat embolism syndrome. J Emerg Trauma Shock. 2009 Jan;2(1):29-33. doi: 10.4103/0974-2700.44680.
- Kwiatt ME, Seamon MJ. Fat embolism syndrome. Int J Crit Illn Inj Sci. 2013 Jan;3(1):64-8. doi: 10.4103/2229-5151.109426.
- Webb DP, McKamie WA, Pietsch JB. Resuscitation of fat embolism syndrome with extracorporeal membrane oxygenation. J Extra Corpor Technol. 2004;36:368–370.
- Sen RK, Tripathy SK, Krishnan V. Role of corticosteroid as a prophylactic measure in fat embolism syndrome: a literature review. Musculoskelet Surg. 2012;96:1-8. http://dx.doi.org/10.1007/s12306- 011-0156-1.
- Silva DF, Carmona CV, Calderan TR, Fraga GP, Nascimento B, Rizoli S. The use of corticosteroid for the prophylaxis of fat embolism syndrome in patients with long bone fracture. Rev Col Bras Cir. 2013 Sep-Oct;40(5):423-6.
- http://www.ncbi.nlm.nih.gov/pubmed/23759683
- http://www.ncbi.nlm.nih.gov/pubmed/23466024
