Author: Ryan Pedigo, MD (Chief Resident and PGY-3, Harbor-UCLA Medical Center – @DrPedigo) // Editors: Manpreet Singh, MD (@MPrizzleER) and Alex Koyfman, MD (@EMHighAK)
Featured on #FOAMED REVIEW 41ST EDITION – Thank you to Michael Macias from emCurious (@EMedCurious) for the shout out!
Accidental Hypothermia Pearls
- Hypothermia is a core temperature less than 35 degrees Celsius
Hypothermic patients without vital signs
Should resuscitation be initiated?
- Must decide if they arrested and then got cold, or arrested because they were cold
- If arrested because they were cold, CPR duration does not predict outcome
- Case report of 190 minutes of CPR with full neurologic recovery – cold is protective!
- In general, a cardiac arrest from hypothermia requires a temperature under 32°C
- Potassium greater than 12 mEq/L is criteria for terminating resuscitation
- If patient’s chest is frozen solid and chest is not compressible, do not resuscitate
Did they have a drowning incident? Was it submersion or immersion?
- Submersion: Patient goes under water immediately, becomes hypoxemic, arrests and cools
- Extremely poor prognosis except perhaps in pediatric patients who can cool faster
- Immersion: Patient is in the water but able to breathe, arrests due to hypothermia only
- Prognosis is good
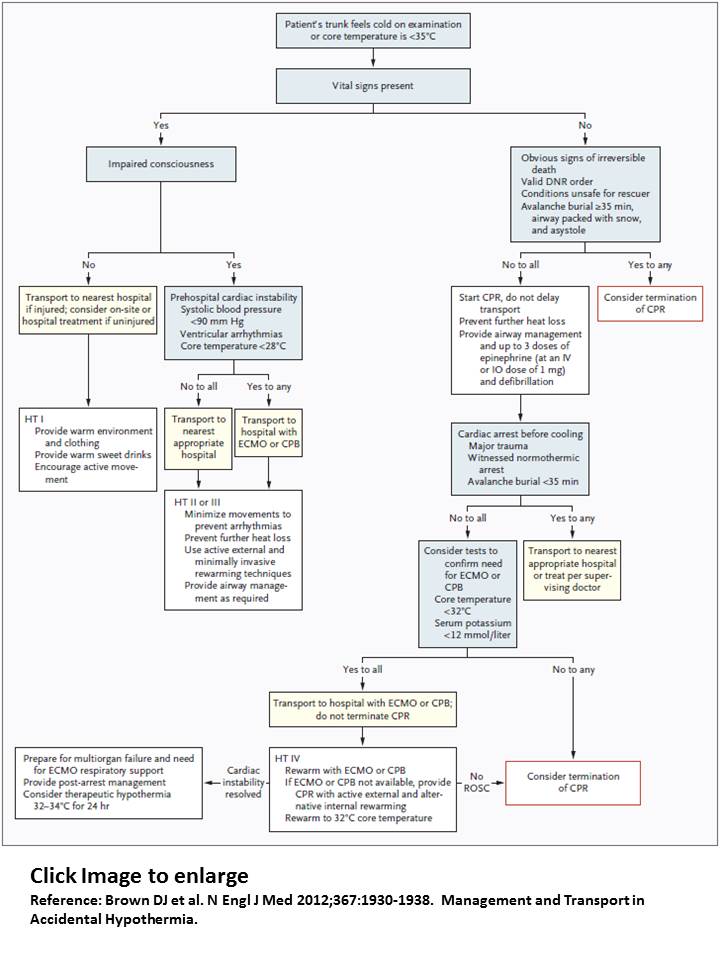
Resuscitation pearls (NEJM Accidental Hypothermia 11/2012)
- Follow management flowchart (see below)
- Warm fluids to prevent further heat loss; cold diuresis may mean high fluid requirements
- Rescue collapse: Cardiac arrest related to extrication / transport of a cold patient
- Minimize patient movement if still has a pulse
- Afterdrop: Continued core cooling during rewarming – physiologically-real but clinically insignificant
- Always consider ECMO and transfer, knowing that CPR duration / transport time is not predictive of outcome
- ECMO center survival rate: 50% (note: selection bias likely contributes to this)
- Non-ECMO center survival rate: 10%
- European Resuscitation Council recommendations
- Up to 3 defibrillations until T > 30°C (then as normal)
- No epinephrine until T > 30°C, only half as frequent epinephrine until T > 35°C
- ACLS on epinephrine in hypothermia: “may be reasonable to consider”
Hypothermic patients with vital signs
- Hypothermia with cardiac instability: ECMO transfer
- Consider bladder lavage but need to do esophageal temperature measurements
- Consider thoracic or peritoneal lavage if cannot transfer to ECMO center
- Hypothermia with stable vital signs
- Warm with warm fluids, Bair Hugger, warm room
- If patient becomes unstable, #1 intervention is high-quality CPR
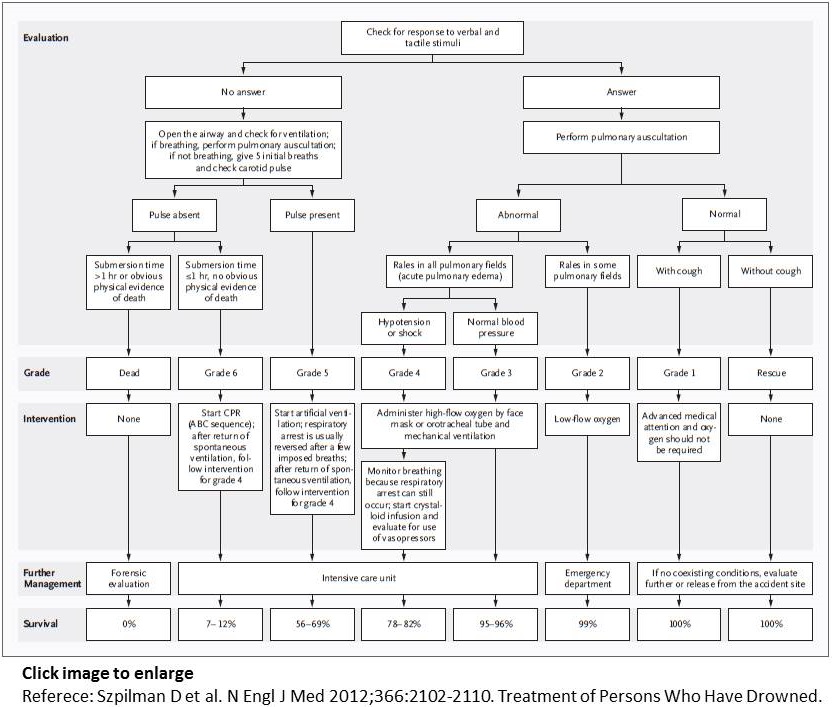
Drowning Pearls
- Definition: Drowning is a process resulting in primary respiratory impairment from submersion/immersion in a liquid medium. Implicit in this definition is that a liquid/air interface is present at the entrance of the victim’s airway, preventing the victim from breathing air. The victim may live or die after this process, but whatever the outcome, he or she has been involved in a drowning incident.
- Nomenclature: Reading the above definition indicates that all patients involved in a drowning incident have drowned, regardless of patient outcome. The terms “dry”, “wet”, “active”, “silent”, “secondary”, and “near-drowning” should not be used (consensus statement, 2003 Circulation).
Pathophysiology
- Breath holding underwater > involuntary gasp > aspiration/laryngospasm > LOC > active aspiration > death
- 90% “wet drowning” and 10% “dry drowning”
- Aspiration leads to loss of surfactant, atelectasis, V/Q mismatch, and ARDS
- Hypoxemia leads to a significant metabolic acidosis
Management
- No prophylactic antibiotics (consider if drowned in obviously infected source such as sewage tank)
- C-spine immobilization only if high concern for injury (injuries only occur in 0.5% of drowning)
References:
Brown DJ et al. N Engl J Med 2012;367:1930-1938. Management and Transport in Accidental Hypothermia.
Szpilman D et al. N Engl J Med 2012;366:2102-2110. Treatment of Persons Who Have Drowned.






4 thoughts on “Hypothermia and Drowning Pearls”
Pingback: Hypothermia and Drowning Pearls | FOAM links
Pingback: Pediatric Drowning and Hypothermia | CritCases | EM Cases