Author: Tim Montrief (@EMinMiami, PGY-1, Emergency Medicine Residency Program, Jackson Memorial Health System), Cynthia Santos, MD (Assistant Professor, Emergency Medicine, Medical Toxicology, Rutgers NJMS) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital), and Brit Long, MD (@long_brit)
Case:
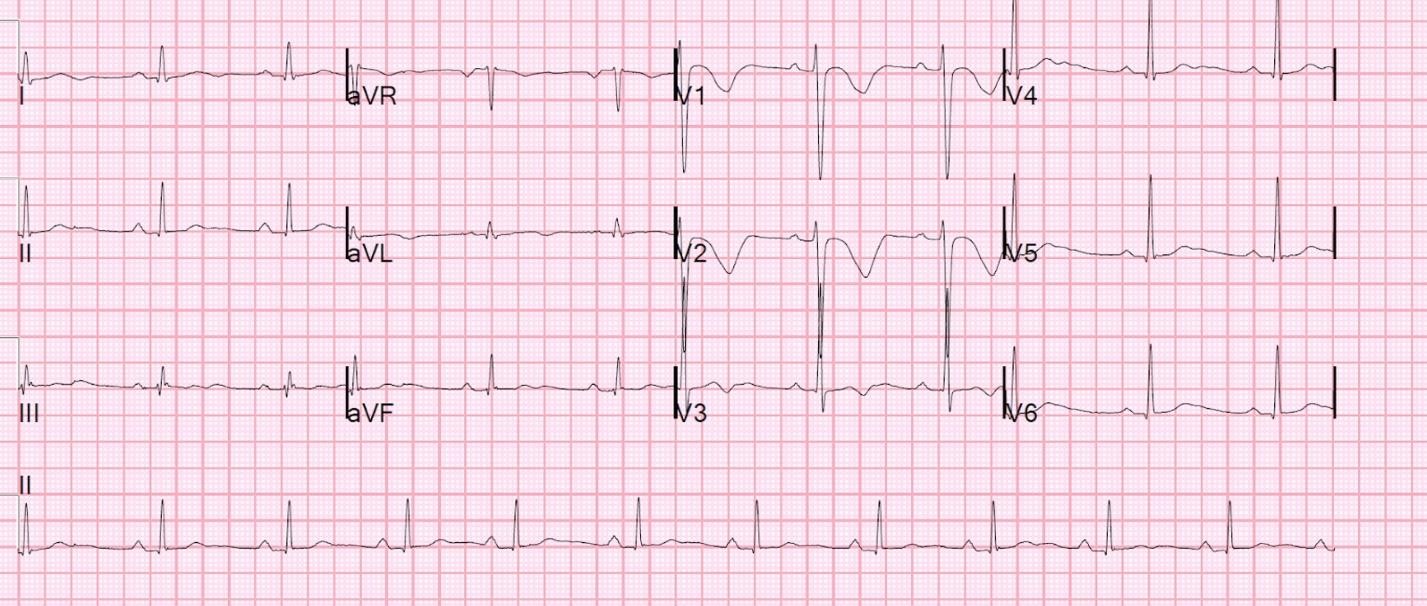
A 20-year-old man with a past medical history of heroin abuse is brought in to the Emergency Department by EMS complaining of palpitations and syncope. The patient admits to taking up to 100 mg of loperamide per day “for weeks” to attenuate his current withdrawal from heroin. His electrolyte levels are within normal limits, and you get an ECG that shows a QTc interval of 530 ms…
Questions:
- Why is loperamide becoming an emerging drug of abuse? What are the historical, social, and pharmacological factors influencing this?
- What is the clinical presentation of a patient with loperamide toxicity? What are the relevant labs and studies to order?
- What is the cardiac toxicity of loperamide?
- What treatments are available for loperamide toxicity?
Background:
- Loperamide is an inexpensive, widely used nonprescription antidiarrheal that inhibits intestinal peristalsis through its peripheral µ-opioid receptor agonism, as well as calcium channel blockade.1
- Loperamide abuse is increasing, as patients use it either to experience euphoric effects or to attenuate the effects of opioid withdrawal.2,3
- The daily maximum recommended dose is 16 mg for the indication of diarrhea treatment. Abuse of loperamide in order to get high or for self-management of withdrawal commonly occurs at very high doses. Average daily dosing of patients presenting with loperamide toxicity has been reported to range from 200-400 mg, with some reports of ingestions exceeding 1000 mg.2,3
- CYP and P-glycoprotein inhibitors are commonly coingested to increase loperamide plasma concentrations. CYP3A4 and CYP2C8 inhibitors increase the plasma concentration of loperamide by about 2- and 4-fold, respectively, and by over 12-fold when both enzymes are inhibited simultaneously. P-glycoprotein inhibitors also increase the plasma concentration of loperamide by about 2 to 3-fold and can also increase the loperamide CNS concentration by its negative effects on the blood-brain barrier.4
- For example, some users co-ingest cimetidine and grapefruit juice to inhibit CYP enzymes, or black pepper and quinidine to inhibit P-glycoproteins.2,3
- At high doses, loperamide blocks cardiac sodium and potassium channels, resulting in prolonged QRS and QT intervals.1
Clinical Presentation and Workup:
- Clinical presentation: Loperamide toxicity is not characterized by its opioid effects alone. Multiple cases of cardiac toxicity have been published in recent literature, and some have been fatal.5 Signs and symptoms of loperamide toxicity include:
- Palpitations
- Nausea and vomiting
- Anxiety
- Generalized weakness
- Presyncope
- Dyspnea
- New-onset or recurrent syncope
- Decreased level of consciousness
- Seizure-like activity
- Cardiac arrest
- Workup: Pay close attention to cardiac effects related to loperamide toxicity.
- ECG- look for cardiac dysrhythmias, prolonged QRS/QT intervals
- Electrolytes- look for reverse factors for QT-interval prolongation (such as hypokalemia, hypomagnesemia)
- Co-ingestions
Cardiac Toxicity:
- At high doses, loperamide blocks cardiac sodium and potassium channels, resulting in prolonged QRS and QT intervals.6-9
- Presenting rhythms vary, but include:
- Ventricular tachycardia/fibrillation
- Asystole
- Junctional escape
- Torsade de pointes
Management:
- The management of loperamide toxicity is largely supportive, centering around the treatment of any drug toxicity, in conjunction with consultation with the local poison control center.4,10
- Decontamination
- Enhancing elimination
- Antidote therapy
- Supportive care
- Decontamination
- Loperamide is likely absorbed by activated charcoal
- Loperamide levels are reduced nine-fold when activated charcoal is given.
- In therapeutic doses, loperamide’s peak level is about 5 hours after ingestion. This, in addition to loperamide’s effects on reducing bowel motility means you should consider extending the window of when activated charcoal would be appropriate past the typical ~1 hour.11
- Enhancing elimination
- There is no data on whether activated charcoal or whole bowel irrigation would enhance the elimination of loperamide.
- There is no data on whether loperamide is removed by dialysis, ion trapping, or other methods to enhance elimination of toxins.
- Antidote therapy
- Naloxone should be given in the presence of respiratory depression and may require repeated dosing. To prevent the possibility of precipitated opioid withdrawal, the lowest effective dose of naloxone should be used in order to avoid life-threatening complications such as seizures and arrhythmias.5
- Sodium bicarbonate IV may treat the cardiotoxic effects of loperamide, especially the sodium blockade. If sodium bicarbonate is used, be sure to frequently monitor serum electrolytes.
- Supportive Care
- Reverse any electrolyte abnormalities (hypocalcemia, hypokalemia, hypomagnesemia)
- Cardiac dysrhythmias have all be successfully treated with:
- Defibrillation
- Repeated shocks may be required, as one case report required cardioversion more than 15 times.12
- Magnesium
- Amiodarone
- Lidocaine
- Overdrive pacing
- VA ECMO is an option for the select patients in cardiovascular shock refractory to all medical therapies.
- Consideration should be given to managing any underlying opioid use disorder.
Pearls:
- Loperamide is increasingly used as an inexpensive and legal method for opioid abuse and for self-management of opioid withdrawal.
- However, multiple cases of fatal cardiac toxicity have been reported.
- At high doses, loperamide blocks cardiac sodium and potassium channels, resulting in prolonged QRS and QT intervals.
- Management of loperamide toxicity is largely supportive and should be managed with decontamination, elimination, antidotes, and supportive care in conjunction with consultation with the local poison control center.
References:
- Baker DE. Loperamide: a pharmacological review. Rev Gastroenterol Disord. 2007;7(suppl 3):S11-S18
- Daniulaityte R , Carlson R , Falck R , et al. “I just wanted to tell you that loperamide WILL WORK”:a web-based study of extra-medical use of loperamide. Drug Alcohol Depend 2013;130:241-44.
- Lasoff DR, Koh CH, Corbett B, et al. Loperamide Trends in Abuse and Misuse Over 13 Years: 2002-2015. Pharmacotherapy. 2017;37(2):249-253.
- Horn J, Hansten P. Loperamide: Danger of Elevated Plasma Concentrations. Pharmacy Times, published on August 18 2016. Available at: http://www.pharmacytimes.com/publications/issue/2016/august2016/loperamide-danger-of-elevated-plasma-concentrations
- Wu PE, Juurlink DN. Clinical Review: Loperamide Toxicity. Ann Emerg Med. 2017;70(2):245-252.
- Kang J, Compton DR, Vaz RJ, et al. Proarrhythmic mechanisms of the common anti-diarrheal medication loperamide: revelations from the opioid abuse epidemic. Naunyn Schmiedebergs Arch Pharmacol. 2016;389:1133-1137.
- Lasoff DR, Schneir A. Ventricular dysrhythmias from loperamide misuse. J Emerg Med. 2016;50:508-509
- Bhatti Z, Norsworthy J, Szombathy T. Loperamide metabolite-induced cardiomyopathy and QTc prolongation. Clin Toxicol. 2017.
- Mirza M, Attakamvelly S, Dillon A, et al. Potential life threatening cardiac toxicity from an easily accessible over the counter drug. Journal of the American College of Cardiology. 2017;69:2375.
- Pharmacy Joe. 88:Treatment of loperamide cardiac toxicity. 2016. Available at: https://www.pharmacyjoe.com/treatment-of-loperamide-cardiac-toxicity/
- Juurlink DN. Activated charcoal for acute overdose: a reappraisal. Br J Clin Pharmacol. 2016;81:482-487.
- Marraffa JM, Holland MG, Sullivan RW, et al. Cardiac conduction disturbance after loperamide abuse. Clin Toxicol (Phila). 2014;52(9):952-7.








1 thought on “TOXCard: Loperamide Toxicity”
I am typically a minimalist when it comes to activated charcoal. For these cases, there are a couple of reasons not to give activated charcoal. 1) Loperamide as mentioned above slows GI motility since that’s what it is meant to do. Therefore, these patients have little bowel sounds and are typically constipated. Adding charcoal into the mix may cause a dreaded charcoal brickette. 2) Furthermore, these patients are more likely to be chronic abusers of loperamide rather than an acute ingestion. Most of the loperamide is further down in the GI tract rather than in the stomach.