Originally published at R.E.B.E.L. EM on March 3, 2020. Reposted with permission. Follow Salim R. Rezaie at @srrezaie
Background Information:
The care and management of patients with acute respiratory distress syndrome (ARDS) is complex and follows an inciting injury to the lungs. This constellation of symptoms is characterized by hypoxemia, diffuse lung inflammation, decreased lung compliance and noncardiogenic pulmonary edema typically seen as bilateral opacities on radiographical imaging.1 Slow progress has been made in developing effective ARDS treatments, among them are low tidal volumes which have been shown to improve mortality.2 Over time the development of guidelines such as the ARDSnet protocol have also helped provide a stepwise framework to treatment. However, there are a subset of patients who continue to remain hypoxic and refractory hypoxemia accounts for 10-15% of deaths in ARDS patients.3
The therapies typically implemented to correct refractory hypoxia include proning, inhaled pulmonary vasodilators, extracorporeal membranous oxygenation (ECMO), paralysis, recruitment maneuvers, unconventional ventilator modes and more.4–8 The following post and included infographics focus on the following therapies: Proning, Paralytics and (lung) Protection. It is important to note that regardless of the therapy, specializing care on an individual basis with a risk-benefit analysis is required to give patients the best possible chance at survival.
Proning:

Infographic by Mark Ramzy, DO, (@MRamzyDO)
Paralytics:
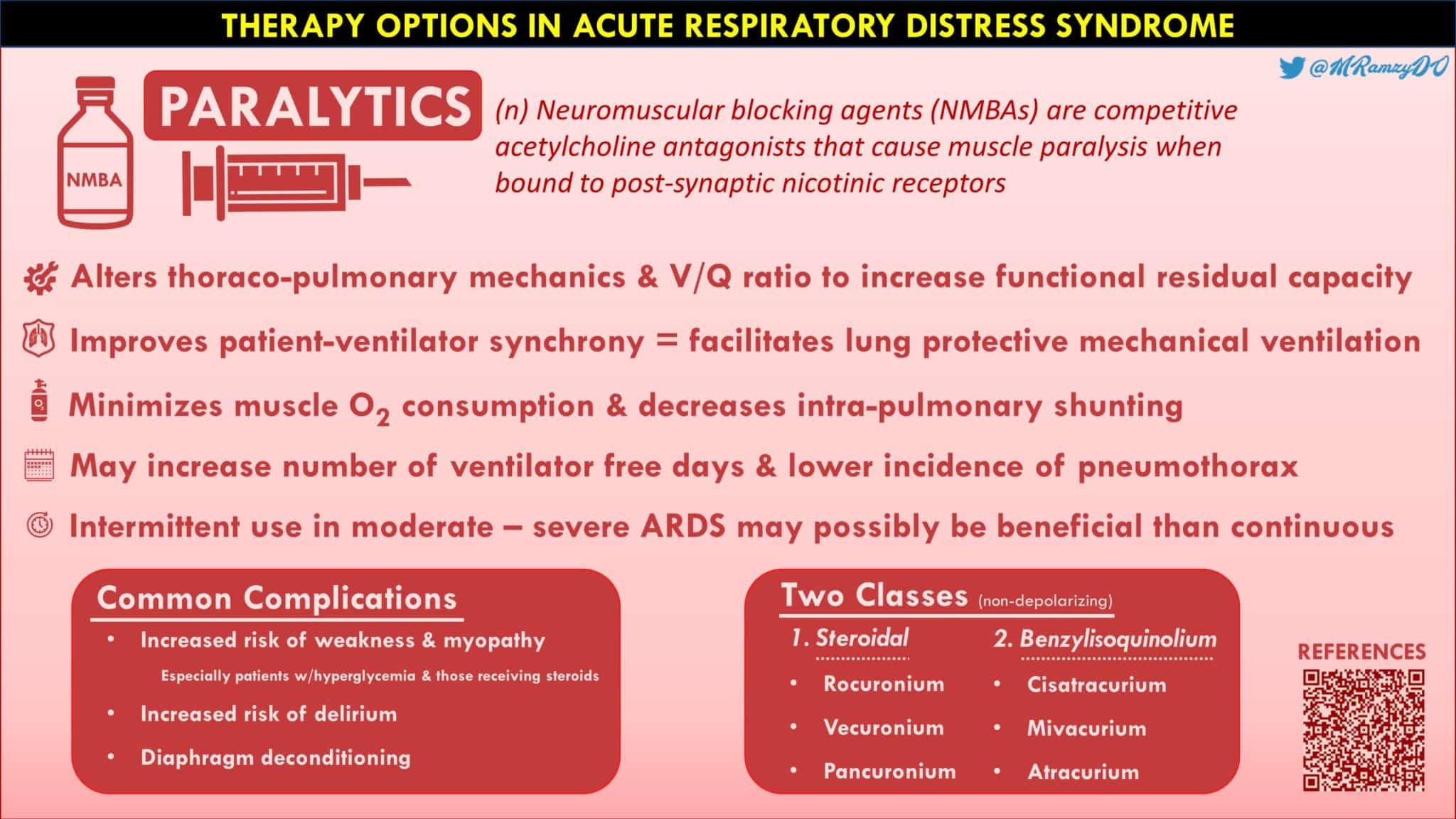
Infographic by Mark Ramzy, DO, (@MRamzyDO)
Protection:
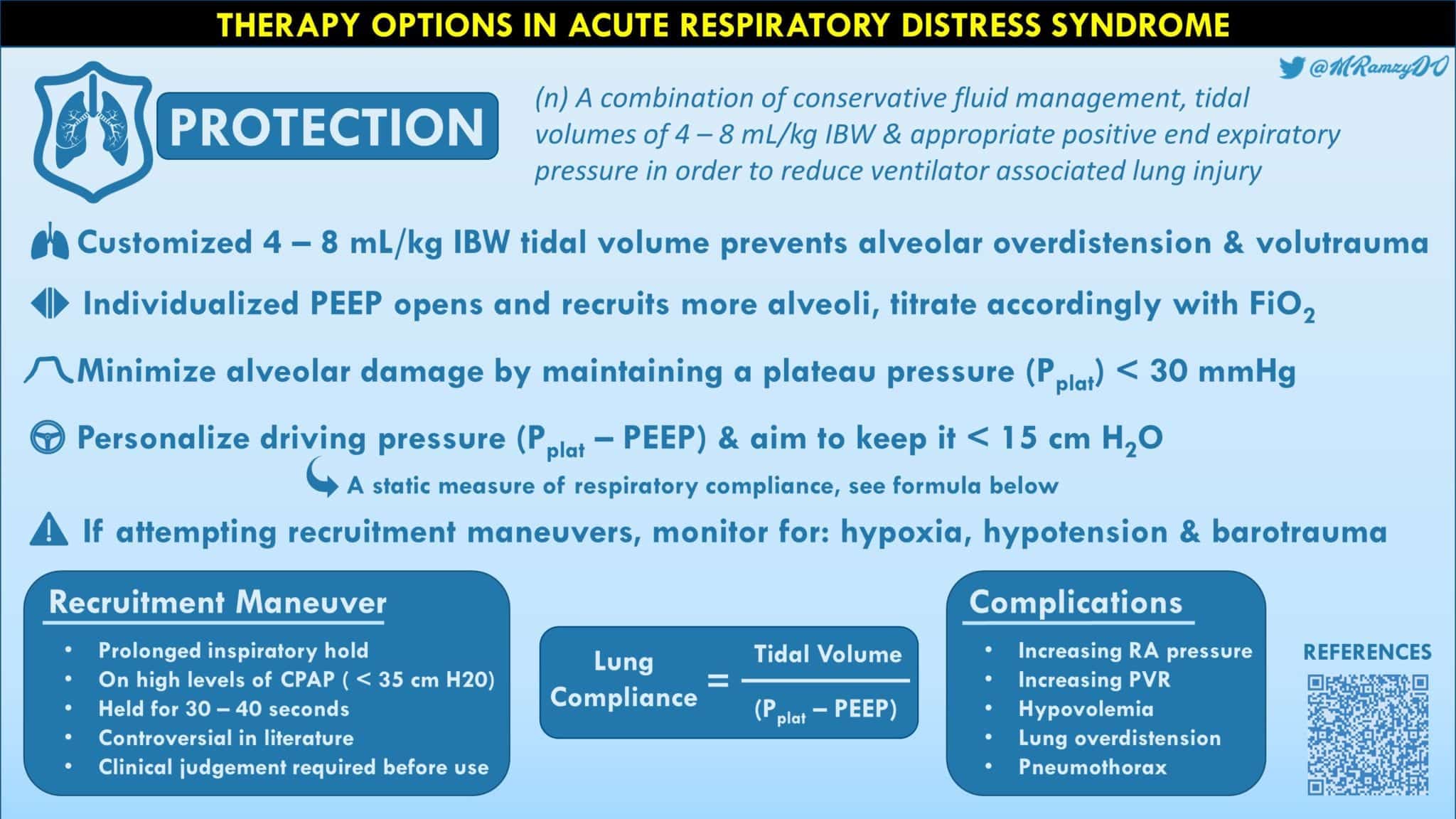
Infographic by Mark Ramzy, DO, (@MRamzyDO)
SUMMARY:
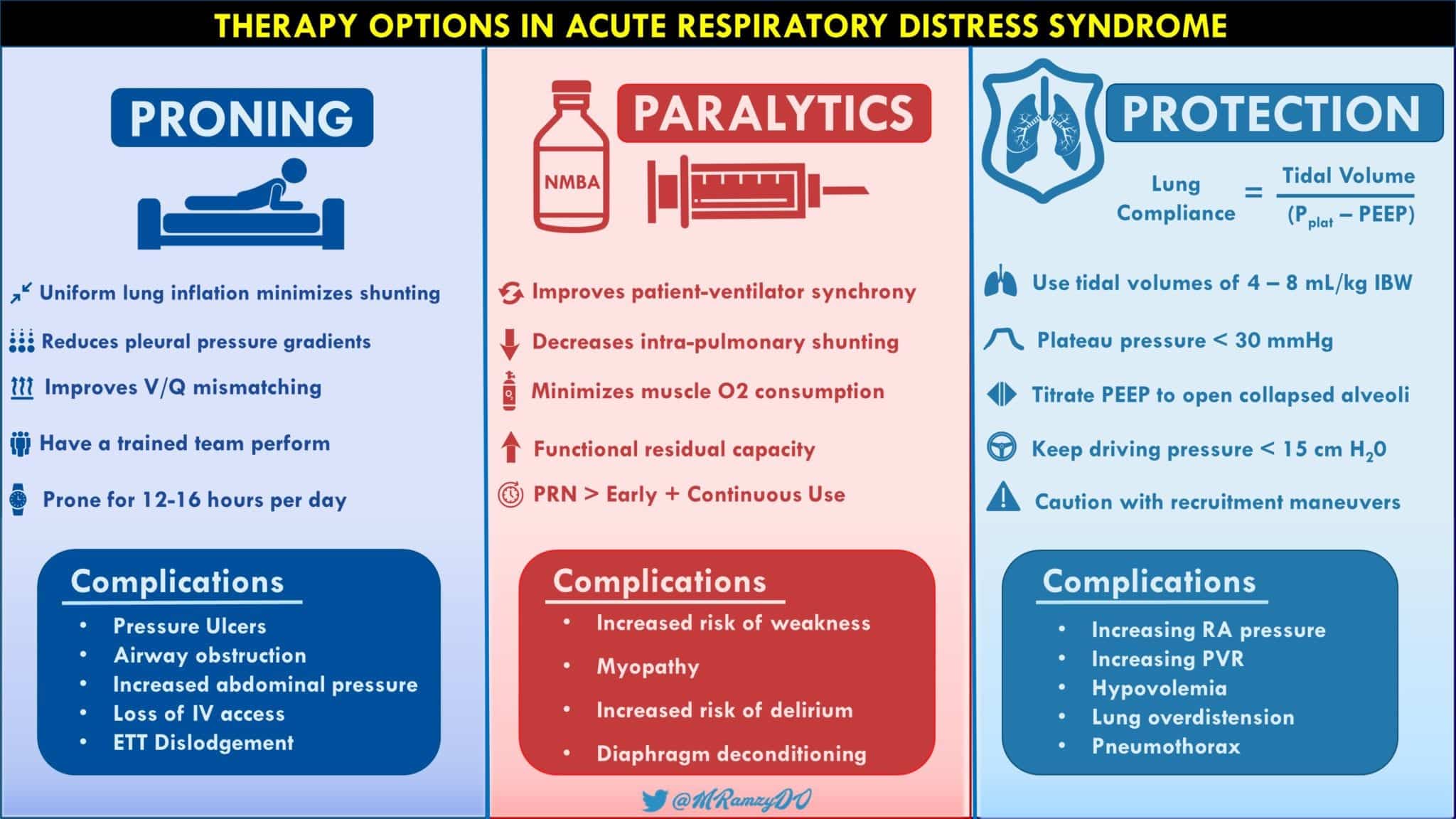
Infographic by Mark Ramzy, DO, (@MRamzyDO)
REFERENCES:
- Cherian SV, et al. Salvage therapies for refractory hypoxemia in ARDS. Respir Med. 2018; PMID: 30053961
- Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N Engl J Med. 2000; PMID: 10793162
- Pipeling MR, Fan E. Therapies for refractory hypoxemia in acute respiratory distress syndrome. JAMA. 2010; PMID: 21139113
- Papazian L, et al. Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. N Engl J Med. 2010; PMID: 20843245
- Gattinoni L, et al. Effect of Prone Positioning on the Survival of Patients with Acute Respiratory Failure. N Engl J Med. 2001; PMID: 11529210
- Noah MA, et al. Referral to an extracorporeal membrane oxygenation center and mortality among patients with severe 2009 influenza A(H1N1). JAMA. 2011; PMID: 21976615
- Fan E, et al. Recruitment maneuvers for acute lung injury: a systematic review. Am J Respir Crit Care Med. 2008; PMID: 18776154
- Facchin F, Fan E. Airway Pressure Release Ventilation and High-Frequency Oscillatory Ventilation: Potential Strategies to Treat Severe Hypoxemia and Prevent Ventilator-Induced Lung Injury. Respir Care. 2015; PMID: 26405188
Post Peer Reviewed by: Salim R. Rezaie, MD (Twitter: @srrezaie)







