Author: Erica Simon, DO, MHA (@E_M_Simon, EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC)
It’s three o’clock in the morning on your fourth night shift in a row. While mustering the courage to rescue your energy drink from the dank, dark depths of the staff mini-fridge, you hear a familiar page: “trauma team to the trauma room.” As you walk towards the ambulance bay, the trauma surgeon approaches with information regarding the incoming transfer:
- 17 year-old male – MVC versus pedestrian
- Seen at OSH where CTs demonstrated: epidural hematoma, grade III liver laceration, grade II splenic laceration, open book pelvic fracture, and extraperitoneal bladder rupture
- Patient underwent external pelvic fixation and transfusion of blood products (8U PRBCs, 8U FFP and 4U Plts)
- Most recent VS: BP 136/89, HR 92, RR (intubated/ventilated):14, SpO2 99% (FiO2 70%)
Drawing your attention to a piece of paper in his hand, detailing what appear to be labs from the outside facility, the surgeon points to a colorful figure: “I’m very concerned about this”:
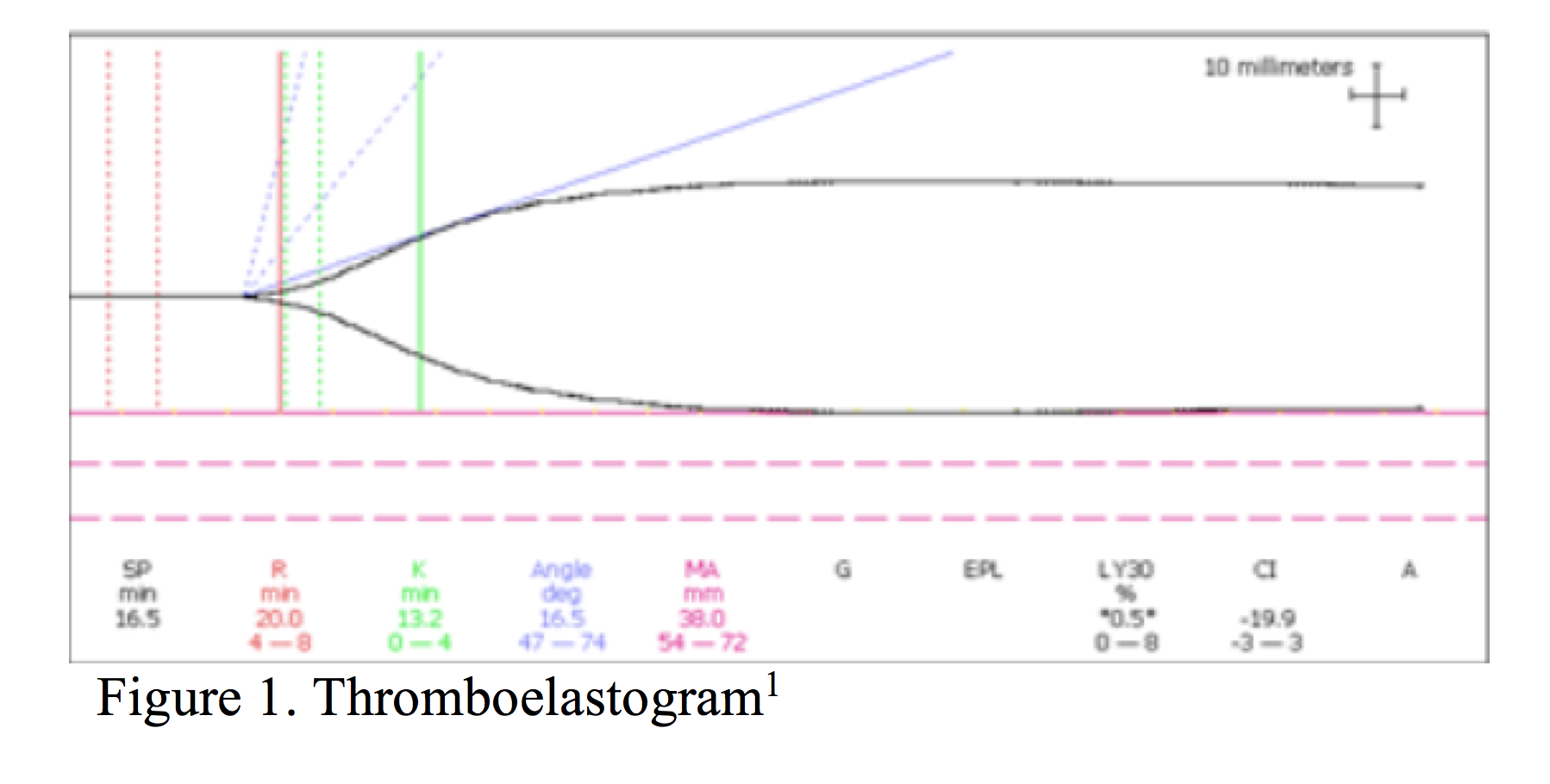
Scanning your mind for intelligent thought, you realize that it’s been some time since you’ve ordered a thromboelastogram (TEG), let alone interpreted one.
If you’re like this physician, take a few minutes to scan the following review – the quick and dirty on TEGs is coming your way.
Thromboelastography – What is it?
Developed in 1948 by Dr. Hellmut Harter, thromboelastography is a mechanism of assessing coagulation based upon the viscoelastic properties of whole blood.2-8 In contrast to traditional, static measurements of hemostasis (PT, aPTT, INR, fibrinogen level, and fibrin degradation products), thromboelastography allows for an assessment of near real-time, in-vivo clotting capacity, providing the interpreter information regarding the dynamics of clot development, stabilization, and dissolution.7 When utilized as a point-of-care assay, graphic interpretation of thromboelastography (the TEG), offers the opportunity for an expedited assessment of coagulopathies (thrombocytopenia, factor deficiency, heparin effect, hypofibrinogenemia, and hyperfibrinolysis).7,9,12,13
How is a TEG performed?
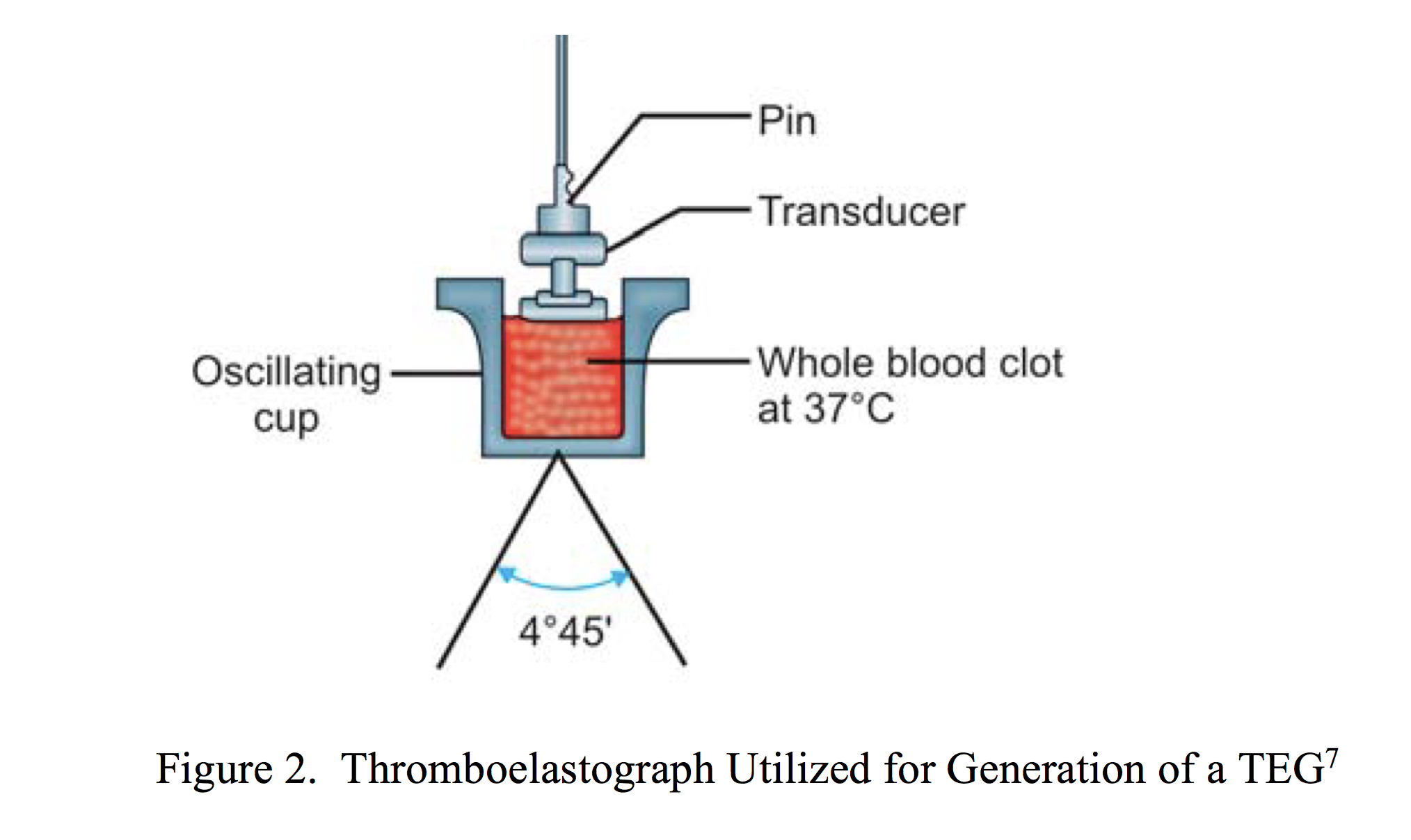
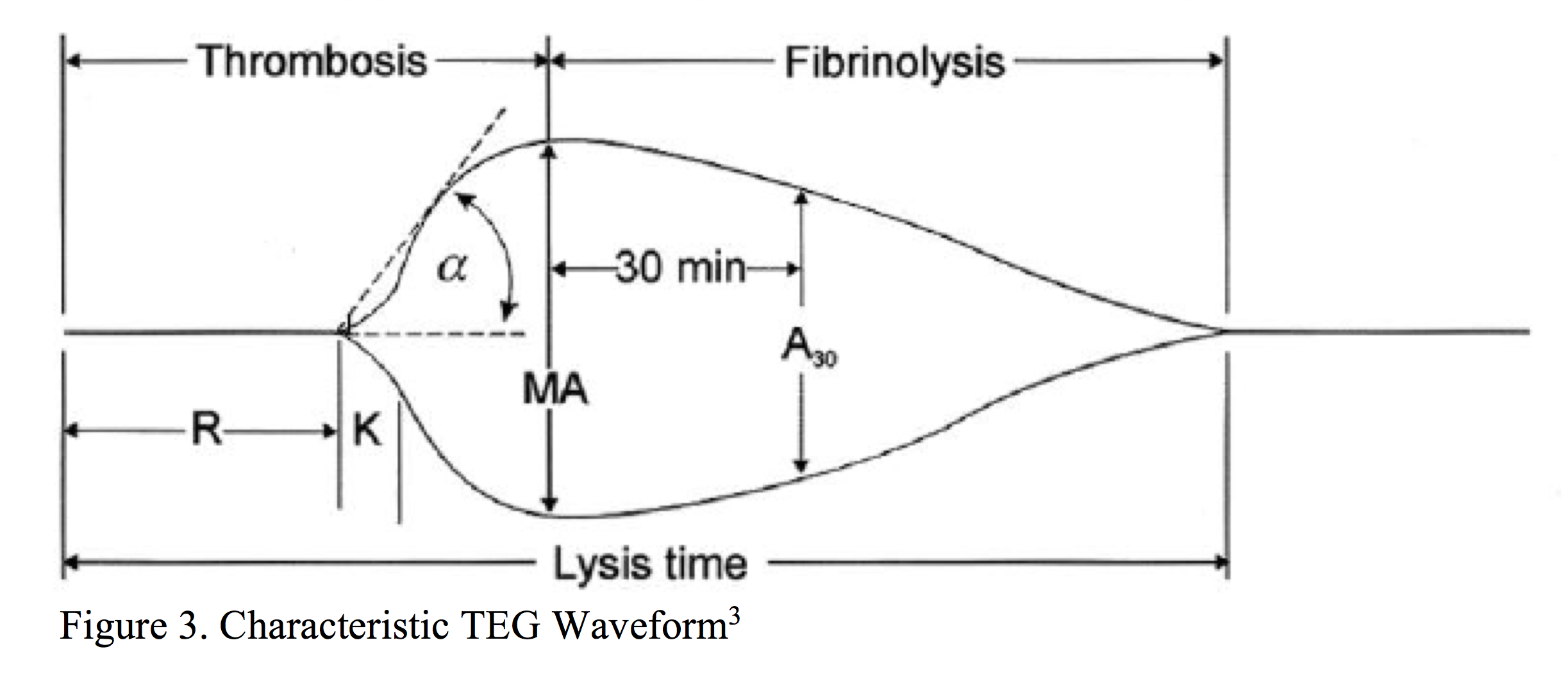
In order to perform a TEG, a citrated-sample of whole blood is placed into a heated sample cup with calcium chloride (to overcome the effects of the citrate), kaolin (a negatively charged molecule known to initiate the intrinsic pathway10), and phospholipids (required for optimal functioning of the extrinsic pathway11) (Figure 2). As the sample cup oscillates in a limited arc, formation of clot results in the generation of rotational forces on a pin suspended from a torsion wire. Forces translated to the torsion wire are then, in turn, transmitted to an electrical transducer, creating a characteristic waveform (Figure 3).
I’ve heard of the Rapid TEG (r-TEG), is there a Difference?
When performed by a trained laboratory specialist, an r-TEG may be completed within 15 minutes as compared to the average 30-45 minutes processing time for a standard TEG.4,5,14 In contrast to a TEG, whole blood samples for an r-TEG may be performed with citrated or non-citrated samples.4 Samples utilized for an r-TEG are combined with tissue factor (activating the extrinsic pathway), and kaolin (activating the intrinsic pathway as above) +/- calcium chloride as applicable.4
I’ve also heard of ROTEM, what is it?
Although utilizing the technique developed by Dr. Harter, rotational thromboelastometry (ROTEM) differs from traditional thromboelastography in its mechanical application. Unlike traditional thromboelastography, which utilizes a sample cup rotating in a limited arc, ROTEM employs a static sample cup with an oscillating pin/wire transduction system. By comparison, ROTEM is also a more complex diagnostic test as it requires a number of differing reagents. A complete discussion of ROTEM is outside the scope of this review. If interested in further reading, see:
Tanaka K, Bolliger D. Practical aspects of rotational thromboelastometry (ROTEM). Available from: https://www.scahq.org/sca3/events/2009/annual/syllabus/workshops/subs/wkshp6pdfs/ROTEM%20-%20Tanaka.doc.pdf
Haemoview Diagnostics. ROTEM analysis: thromboelastometry. Available from http://www.haemoview.com.au/rotem-analysis.html
Haemoview. The 5 ROTEM tests. Available from http://www.haemoview.com.au/uploads/2/5/4/9/25498232/the_5_rotem_tests.pdf
How Do I Interpret TEG and r-TEG Results?
Drs. Semon and Cheatham of the Orlando Regional Medical Center Department of Surgical Education generated an excellent quick reference chart:
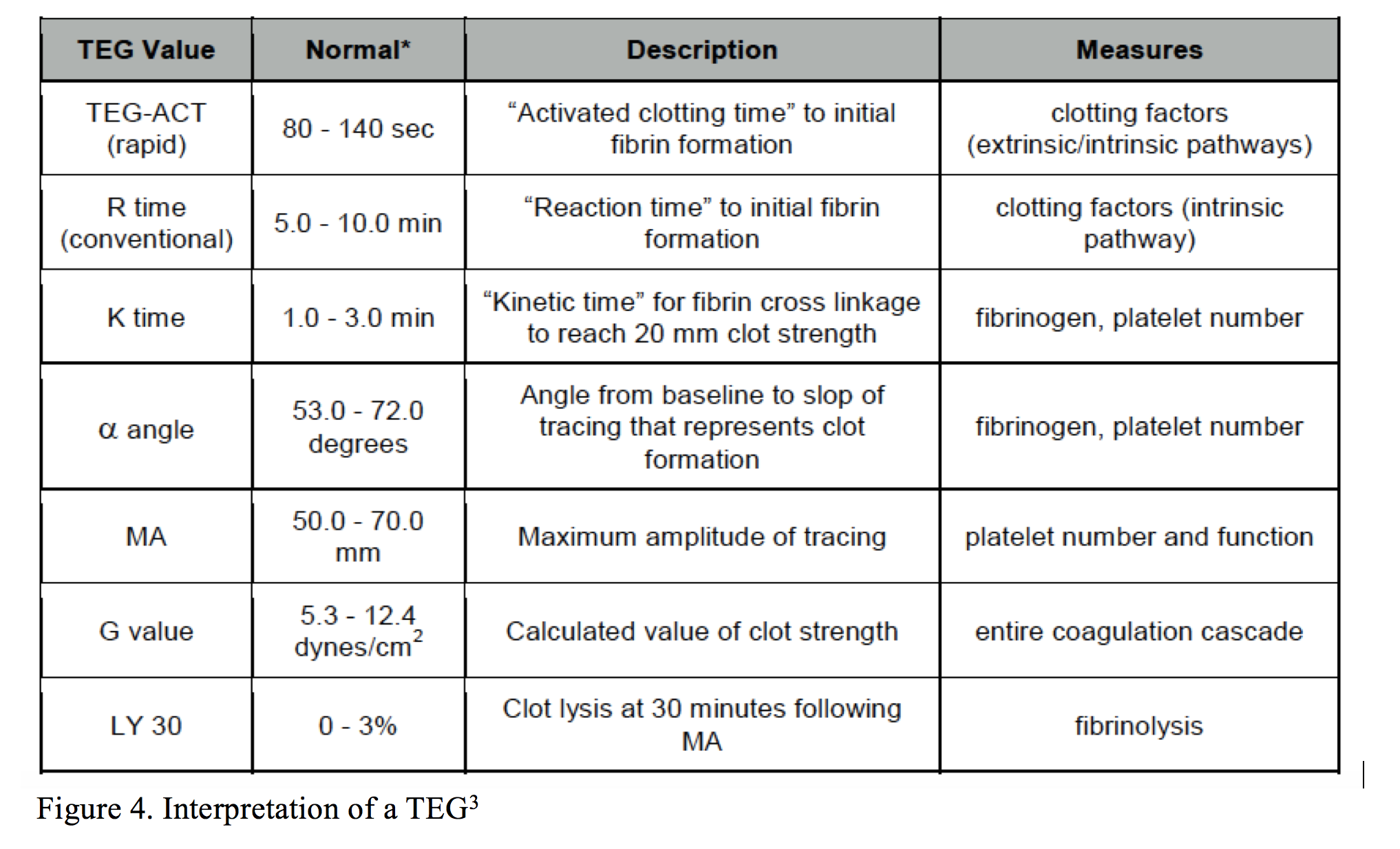
*Note: TEG-ACT (rapid) – reported for r-TEG only.
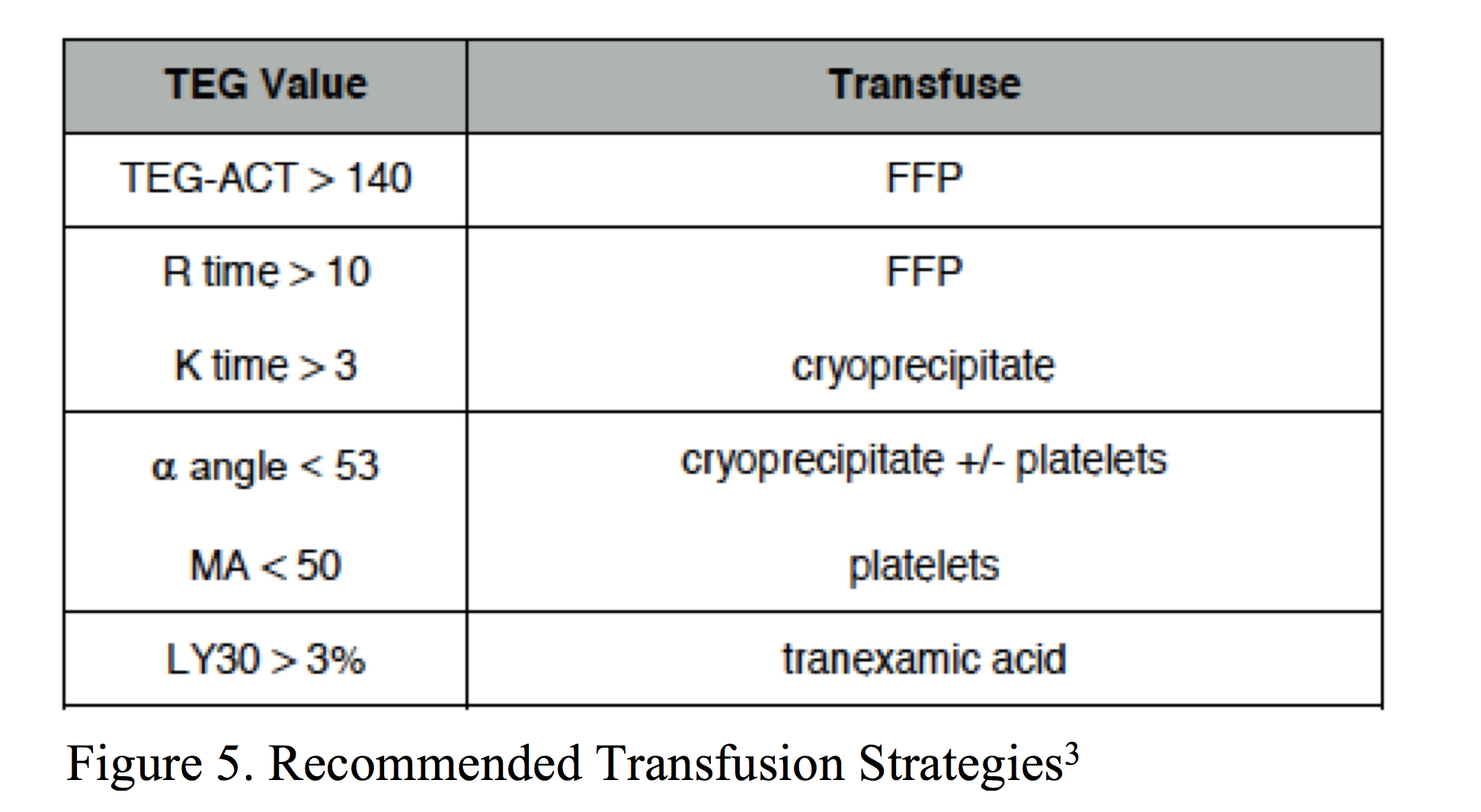
A TEG-Guided Transfusion Strategy
In addressing TEG and r-TEG abnormalities, experts recommend the following3:
The Quick and Dirty: Pattern Recognition
Perhaps most useful for the ED physician is knowledge of qualitative TEG representations:
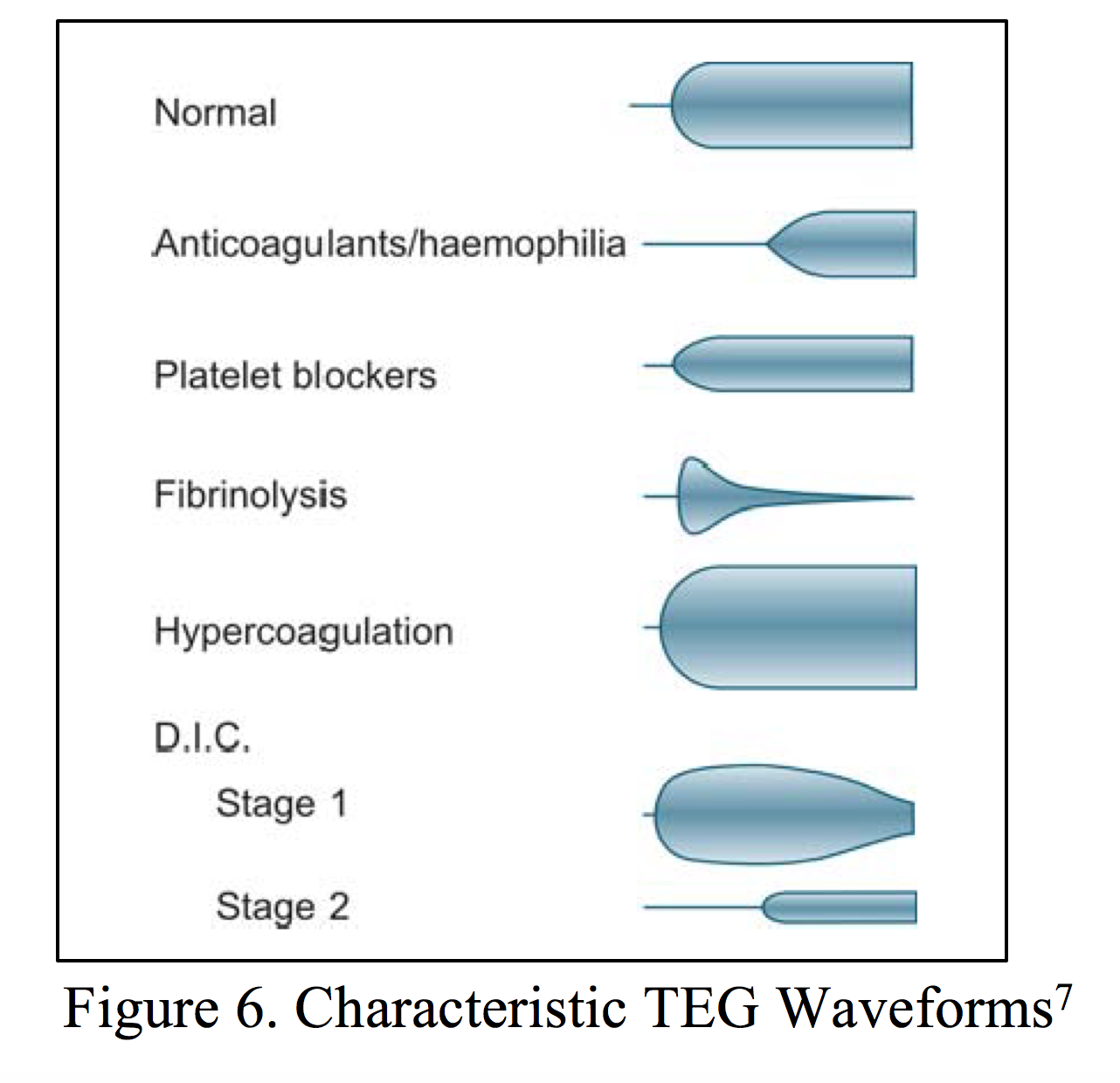
Some clarification on DIC Stage 1 and 2:
- Stage 1: Fibrinolysis results in the degradation of fibrin, increasing fibrin degradation products (FDPs). Excess FDPs result in clot de-stabilization.1
- Stage 2: The cycle of clot formation and breakdown results in platelet and clotting factor consumption.1
Why Might an Emergency Medicine Physician Want to Know about this Test?
Coagulation abnormalities in trauma patients have demonstrated a significant association with infection, multi-organ failure, and death.15-18 Given its ability to quickly detect hematologic pathology, the TEG is becoming a tool for the evaluation of transfusion requirements/coagulopathy post transfusion in this patient population.3,12,13
What does the literature say?
Cotton, et al., 20114:
- Pilot study to evaluate the timeliness of r-TEG results, their correlation to conventional coagulation testing (CCT – PT, aPTT, INR, platelet count, fibrinogen), and the ability of r-TEG to predict early blood transfusion.
- 272 patients meeting requirements for major trauma activation
- Outcomes:
- All r-TEG values available within 15 minutes vs. 48 minutes for CCTs
- ACT, r-value, k-time correlated with PT, INR, PTT (r >0.70; p<0.001)
- MA and a-angle correlated with platelet count (p<0.001, p<0.001)
- Controlling for demographics and ED vitals: ACT>128 predicted massive transfusion (>10 U) in the first 6 hours of presentation and treatment
Bottom line – r-TEG results were available within minutes, results correlated with conventional coagulation test results, and were predictive of the requirement for early massive transfusion.
Holocomb, et al., 201219:
- Study to evaluate the reliability of r-TEGs versus CCTs in predicting blood product transfusion
- 1974 major trauma patients, median ISS 17 (25% meeting criteria for shock; 28% transfused, 6% died within 24 hours)
- Outcomes
- When controlling for age, injury mechanism, weighted-Revised Trauma Score, base excess and hemoglobin, ACT predicted RBC transfusion and a-angle predicted massive transfusion better than PT/aPTT or INR (p<0.001).
- a-angle was superior to fibrinogen for predicting plasma transfusion, and MA was superior to platelet count for predicting platelet transfusion (p<0.001)
Bottom line – r-TEG was more accurate in the prediction of requirements for RBC, plasma, and platelet transfusions as compared to traditional CCTs.
Wikkelso A, et al., 201612:
- Cochrane Review including 17 current RCTs (n=1493 participants)
- Per the authors:
- Low quality studies: numerous biases
- Limited generalizability: majority of studies center on cardiac patients undergoing surgical intervention
- Per the authors:
Bottom line – There is growing evidence to suggest that the utilization of TEG and ROTEM reduce transfusion requirements and improve morbidity in patients with bleeding, but additional studies are required.
Back to Our Case
Why was the trauma surgeon concerned? If we interpret our TEG values:
- R time 20.0 => well above the upper limit of normal (10.0 minutes) = significantly prolonged time for clot formation
- K time 13.2 => normal: up to 10.0 = prolonged fibrin cross-linking
- a-angle 16.5 => normal >53.0 = limited clot formation
- MA 38 => normal platelet function >50 = limited platelet function
More importantly, one quick glance at our TEG and through pattern recognition, we known that aside from his significant traumatic injuries, the patient is in trouble. This waveform is characteristic of DIC Stage 2.
Key Pearls
- A TEG can be used as a rapid assessment of thrombosis and fibrinolysis.
- Although additional RCTs are needed, TEGs utilized in trauma patients have been demonstrated to reduce transfusion requirements (important when we consider TACO/TRALI, risk of DIC, and blood-borne pathogens).
- If nothing else, take a few minutes to review the characteristic TEG waveforms – depending on your laboratory processing time, knowledge of above tracings could allow early identification of coagulopathy and immediate treatment.
References / Further Reading
- Williams. Haemscope Basic Clinician Training: Fibrinolysis and Hyperfibrinolysis TEG Analysis. Available from: www.medicine.wisc.edu/~williams/TEG5_analysis.ppt
- Walsh M, Thomas S, Howard J, Evans E, Guyer K, et al. Blood component therapy in trauma guided with the utilization of the perfusionist and thromboelastography. J Extra Corpor Technol. 2001; 43(4):162-167.
- Semon G, Cheatham M. Thromboelastography in Trauma. Surgical Critical Care Evidence-Based Guidelines Committee. 2014. Available from: www.surgicalcriticalcare.net/Guidelines/TEG%202014.pdf
- Cotton B, Faz G, Hatch Q, Radwan Z, Podbielski J, et al. Rapid thromboelastography delivers real-time results that predict transfusion within 1 hour of admission. J Trauma. 2011; 71:407-417.
- Teodoro da Luz L, Nascimento B, Rizoli S. Thromboelastography (TEG): practical considerations on its clinical use in trauma resuscitation. Scand J Trauma Resusc Emerg Med. 2013; 21:29.
- Bollinger D, Seeberg M, Tanaka K. Principles and practice of thromboelastography in clinical coagulation management and transfusion practice. Transfus Med Rev. 2012: 26(1): 1-13.
- Thakur M, Ahmed A. A review of thromboelastography. Int J periop Ultrasound Apply Technol. 2012; 1(1):25-29.
- Nickson C. Critical Care Compendium: Thromboelastogram (TEG). 2014. Available from http://lifeinthefastlane.com/ccc/thromboelastogram-teg/
- Kashuk J, Moore E, Sawyer M, Wolhauer M, Pezold M, et al. Primary fibrinolysis is integral in the pathogenesis of acute coagulopathy of trauma. Ann Surg. 2010; 252: 434-444.
- Zhu S, Diamond S. Contact activation of blood coagulation on a defined kaolin/collagen surface in microfluidic assay. Thromb Res. 2014; 134(6): 1335-1343.
- Heemskerk J, Bevers E, Lindhout T. Platelet activation and blood coagulation. Throm Haemost. 2002; 88(2):186-193.
- Wikkelso A, Wetterslev J, Moller A, Afshari A. Thromboelastography (TEG) or thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or children with bleeding (Review). Cochrane Database of Systematic Reviews. 2016; 8:1-149.
- Luddington R. Thromboelastography/thromboelastometry. Clin Lab Haematol. 2005; 27(2):81-90.
- Jeger V, Zimmerman H, Exadaktylos A. Can rapid TEG accelerate the search for coagulopathies in the patient with multiple injuries? J Trauma. 2009; 66:1253-1257.
- Niles S, McLaughlin D, Perkins J et al. Increased mortality associated with the early coagulopathy of trauma in combat casualties. J Trauma. 2008; 64:1459-1463.
- Brohi K, Sing J, Heron M. Coats T. Acute traumatic coagulopathy. J Trauma. 2003; 54:1127-1130.
- Cotton B, Gunter O, Isbell J, et al. Damage control hematology: the impact of a trauma exsanguination protocol on survival and blood product utilization. J Trauma. 2008; 64;1177-1182.
- Cohen J, Call M, Nelson M, et al. Clinical and mechanistic drivers of cute traumatic coagulopathy. J Trauma Acute Care Surg. 2013; 75:S40-47.
- Holocomb J, Minei K, Scerbo M, Radwan Z, Wade C, et al. Admission rapid thromboelastography can replace conventional coagulation tests in the emergency department: experience with 1974 consecutive trauma patients. Ann Surg. 2012








3 thoughts on “The Thromboelastogram (TEG®): A Five-Minute Primer for the Emergency Physician”
Pingback: The Thromboelastogram (TEG®): A Five-Minute Primer for the Emergency Physician – Global Intensive Care
Thanks guys – love ur site! Really useful
Pingback: TEG simplified – Code Team Pearls