Author: Nima Rejali, DO (EM Resident Physician, Hackensack University Medical Center) // Reviewed by: Anthony DeVivo, DO (@anthony_devivo); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); Manpreet Singh, MD (@MprizzleER)
Today’s Unlocking Common ED Procedures post looks at penile zipper injuries and entrapment.

Check out our new downloadable procedure card with QR code link to the article. Print them out and be ready to go over it with your learners!
Case 1:
A 12-year-old male presents to the ED with mom and dad in severe distress. You bring the patient into a room immediately and collect history from the parents. The patient was zipping up his jeans after urinating and got his foreskin caught in the zipper. You examine the patient more closely and see that his zipper is completely zipped up and about halfway up the zipper there is redundant penile tissue caught between the teeth of the zipper.
Discussion:
Penile zipper entrapment is a rare but distressing presentation to the ED for patient and family. Of note, this post will not discuss management of paraphimosis or phimosis.
No large-scale studies have been done examining the best method of penile liberation and most of our information on the topic is from case reports and case series. The largest such study was a case series from 1994.1 This study looked at characteristics of 30 children who presented to the ED for penile entrapment. In the study population, the boys ranged from age 2-12, injury occurred more commonly in uncircumcised versus circumcised boys and most injuries were accidentally self-inflicted. Also, 60% of boys were wearing underwear at the time of injury and most injuries were noted to occur while zipping up as opposed to unzipping.¹
Once a penile entrapment is confirmed, we suggest a stepwise approach to the management of such injuries. The steps include:
1) Identifying the nature of the injury
2) Pain management and analgesia
3) Approach to penile liberation
1. Identifying the nature of the injury
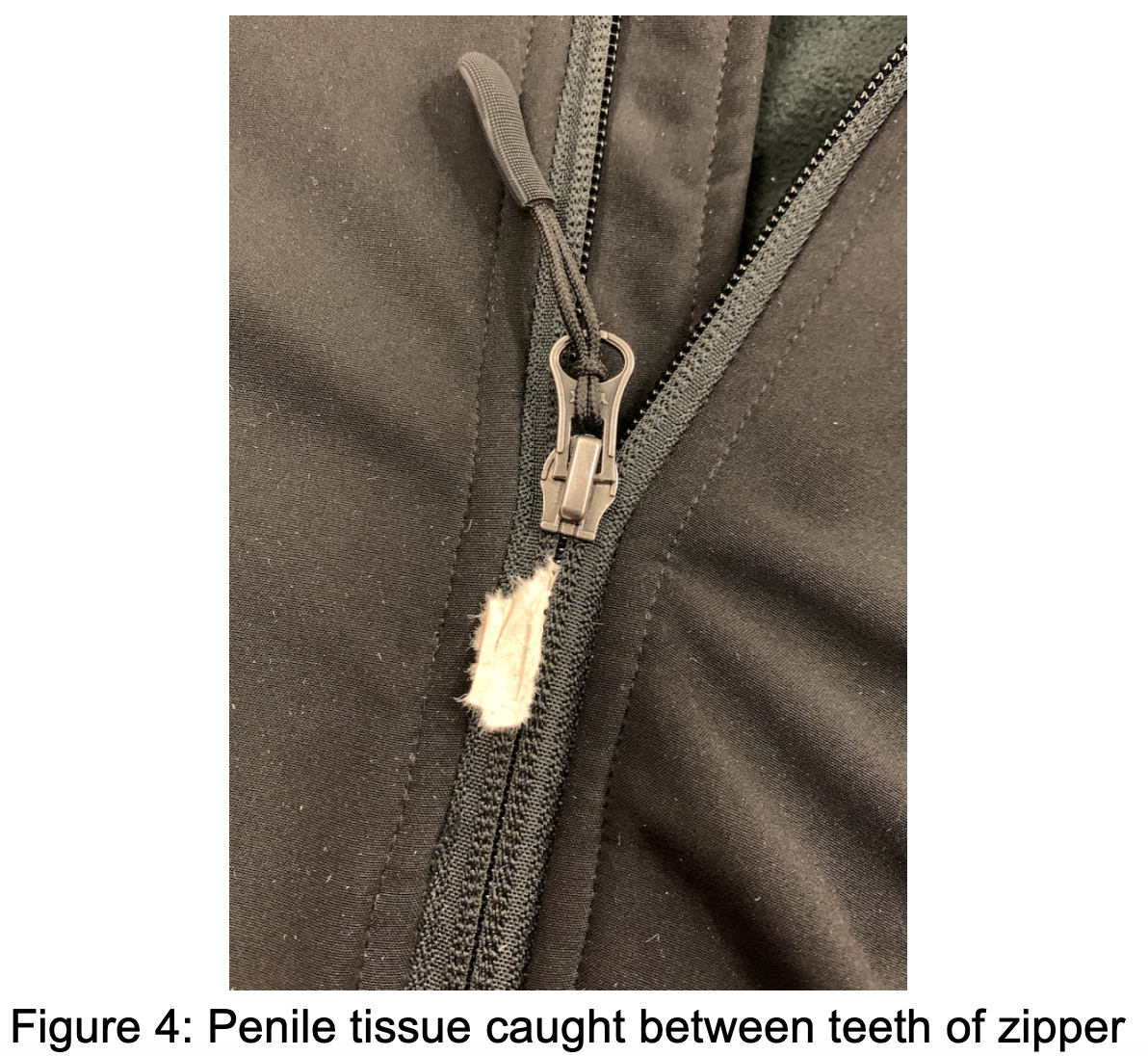
In regard to penile zipper entrapment, two main types of injury have been identified. These include penile tissue getting caught in the sliding mechanism itself (figure 3) as well as penile tissue getting caught between the zipper teeth (figure 4). It is important to identify the exact mechanism as they have different approaches to liberating the patient from the entrapment. If the mechanism is not easily identifiable, better exposure should be obtained. In this case, it would mean cutting the clothing off around the zipper, leaving only the zipper and immediately surrounding fabric still attached to the patient. This will allow for different lines of sight to better identify the type and extent of injury.



2. Pain management
Once the injury is identified and a plan for intervention has been made, attention should be turned to pain relief as well as anxiolysis if needed. Particularly in the patient population which this occurs in primarily, this may need to be addressed before you can better expose the injury to identify the mechanism. There are a variety of different methods we can use in the ED for pain control. Ultimately, more than 1 method may need to be used.
Pain control should be initiated utilizing minimally invasive measures before proceeding to sedative hypnotics or opioids. If your ED has a child life specialist, involve them in the case early as they are experts at keeping children calm and cooperative in the ED-particularly if they are about to undergo a procedure. The patient may not even let you examine them due to distress or pain. If this is the case, 1.5mcg/kg of intranasal fentanyl can achieve good pain control without the fear of needles.2 An adjunct/alternative as well would be to use intravenous ketamine for pain control and anxiolysis. Doses will vary based on your goals. Typically for acute pain providers may elect to use 0.1-0.3mg/kg given over slow infusion of 15-20 minutes mixed in a small saline bag 100-250cc.3 If you seek to use ketamine for procedural sedation, typically a dose of 0.5-1mg/kg will be required. The advantages of ketamine for procedural sedation include the fact that it will both sedate as well as give analgesic effects and it will preserve respiratory drive. Topical anesthetic is also a great option and should be considered first line. The use of EMLA cream has been described in the literature as being used for topical anesthesia.4,5,6 EMLA is a mixture of 2.5%Lidocaine-2.5%Prilocaine in a cream which is applied to the skin using an occlusive dressing.4 EMLA cream can be used on intact skin without any skin breaks or lacerations as it is made of small compound molecules that can diffuse through the skin. Unfortunately, it takes a long time to achieve therapeutic effect, approximately 60-90 minutes which may not be adequate if the patient is in significant distress or if there is serious injury and/or edema.5 Liposomal Lidocaine can also be used, which is similar in mechanism to EMLA cream but does not require occlusive dressing over the application site and onset is usually quicker, approximately 30 minutes vs 60 minutes, thus is the preferred topic agent for urologic procedures in pediatrics.7,8 LET (Lidocaine-Epinephrine-Tetracaine) gel should be avoided in penile injuries as there exists a small risk of necrosis due to end organ effects of epinephrine induced vasoconstriction.9Using EMLA or liposomal lidocaine may also provide enough lubrication to liberate the trapped tissue from the zipper, although this should not be expected.
Pain control can also be achieved through a dorsal penile nerve block (figure 5). This option is better reserved for when a large amount of tissue is entrapped or if prolonged/aggressive manipulation will be required to liberate the skin.10 Below is a quick procedure guide:
1: Clean the base of the penis with antiseptic solution.
2: Fill a syringe with approximately 5cc of 1% Lidocaine WITHOUT epinephrine.
3: Using a 20- or 22-gauge needle pierce the skin at the base of the penis at the 11 and 1 o’clock positions. Advance the needle 3-5mm or until you feel a “pop” which indicates you have pierced through buck’s fascia.
4: Drawn back on the syringe to make sure you are not in a vein or artery.
5: Infuse about 1-2cc per side.
6: Adequate analgesia should be experienced in approximately 5-10 minutes.

Your patient may still be in distress, even after a nerve block. This may be from inadequate analgesia or from the trauma of the injury/experience. At this point, the patient may require procedural sedation in the ED and/or consideration to go to the OR with urology for further management.
3. Approach to Penile Liberation
After identifying the type and injury and adequately controlling pain, we turn our attention to definitive treatment.
Penile skin caught between teeth
Of the two types of injury, this is the easier one to treat. In this case, the redundant skin of the penis gets caught in the teeth of the zipper but the sliding mechanism is still advanced above the point of injury. Utilizing trauma shears or heavy-duty scissors, cut across horizontally on the entire zipper apparatus either below or above the area of entrapped skin (figure 6). This should allow for the teeth to easily disengage from each other.11 The zipper can then manually be pulled apart with ease and the penis will be free.

Penile skin caught in the sliding mechanism
If the penis gets caught in the sliding mechanism of the zipper itself, liberation is often a more technically difficult procedure. You may first wish to try mineral oil to lubricate the skin.12 Leave this on for approximately 10 minutes then apply gentle traction to try and pull free the skin out of where it is jammed into the sliding mechanism. If mineral oil is not available, substitute for soap and water. Typically when the skin is trapped within the sliding mechanism, this will usually require more than gentle traction for liberation but it is a reasonable first approach.
Should the mineral oil lubrication fail, the sliding mechanism will need to be cut apart or pried off manually. The sliding mechanism is made up of 2 faceplates that are joined together by a median bar. If the median bar is cut through completely, the 2 faceplates will separate and then the skin should be easily freed as the zipper should come apart easily.13,14 The difficulty in this technique is finding an instrument that is small enough to fit in this small space and also strong enough to cut the median bar. Usual tools that are used include wire cutters or bone cutters-helpful if you find “needle nosed” versions of these tools. If these are not readily available in your ED, you may need to call the OR or central supply to obtain the tools necessary. This will become increasingly more difficult with more and more edema so the sooner you can act, the higher the procedural success rate will be.
If you are unable to access the median bar or are unable to cut through the median bar, you may also try using a screwdriver to liberate the penile tissue.12 In this technique, a thin flat-head screwdriver head is placed in the space between the anterior and posterior faceplates. The screwdriver is then rotated 90 degrees in the hopes of popping the sliding mechanism off the zipper teeth completely or simply widening the space between the 2 faceplates to allow for more space to attempt liberating the tissue with simple traction. Widening the space between the 2 faceplates may also create enough space where the teeth disengage from the sliding mechanism and allow for the ipsilateral zipper teeth to pull apart easily from the sliding mechanism.

One last option would be to thoroughly anesthetize the penis and then simply undo the zipper by pulling it back in the opposite direction that caused the injury or to also apply lateral traction and try to pull the zipper teeth apart. These last two techniques have the potential to cause worsening trauma and are not advisable. Should you attempt to liberate the entrapped tissue and fail, you will need to call a urologist for consultation or transfer the patient to a facility with an accepting urologist. At this point the patient may require OR exploration and/or circumcision which is best done by a urologist in a controlled environment.
Case 2:
67-year-old male presents to the ED with penis pain. The patient states he had placed a “cock ring” last night prior to sexual activity with his wife. Patient was unable to remove the ring after sex but did not have significant pain and went to sleep. He woke up this morning with extreme pain and discoloration. You take him to an exam room and have the patient disrobe. He has a metallic ring around the base of his penis. The penis is massively engorged and ecchymotic and it is tender to touch. The patient attempts to provide a urine sample but he is unable to void.
Discussion:
Penile strangulation is an uncommon complaint in the emergency department but one that requires rapid intervention due to the risk of ischemic necrosis and potential loss of organ function. There have only been less than 120 case reports ever published on the topic since 1755.15,16 However, a large majority of such cases may be under-reported so the numbers may not be as low as the literature will lead one to believe. Usually the patient’s strangulation will be secondary to a non-metallic or metallic ring that is placed around the base of the penis for sexual enhancement. The ring may encircle only the penile shaft, or the shaft and scrotum-the latter typically causing more complications related to ischemia and vascular congestion. However, there have also been reports of patient placing these objects or other constricting objects (bottles, lugs, etc…) around the penis secondary to psychiatric illness.17 Symptoms are progressive and can range from mild pain and swelling after just a few hours all the way to necrosis, auto-amputation and sepsis if strangulation occurs for longer. By limiting venous drainage, the ring will lead to worsening edema, eventually leading to penile compartment syndrome as the lack of venous drainage causes arterial ischemia. Prolonged ischemia will result in ischemic injury, gangrene, and necrosis if no intervention is had.18 Additionally, patients will typically not present immediately after getting the ring stuck as they will be worried about embarrassment and/or shame so by the time they arrive to your door in the ED they may already be on the way to organ ischemia.
Examination should be done first to better assess the situation. Obtain vital signs and do a detailed GU exam. Look for edema, discoloration, skin changes, or other signs of tissue necrosis. Try to identify what kind of ring or object is strangulating the penis. Penile rings are made in a plethora of shapes, sizes, thickness, and materials but most commonly will be made of some sort of hard rubber/plastic or some metallic alloy. Ask the patient if they know what the ring is made of. If they do not know, ask if they know the name of the product or if they bought it online then where they got it as it may help you identify the materials used. In the ED, typically the rubber/plastic ones are more amenable to intervention in the department while the metallic ones can require industrial power tools or surgical tools for safe removal. A few research groups are currently recommending updating tetanus in the ED as well as early IV antibiotics, recommending initially a 3rd generation cephalosporin such as Ceftriaxone.18,19 Also assess for any signs or symptoms of urethral injury such as blood at the meatus, tissue erosion at the site of contact, or inability to void. It is not uncommon to have to place a suprapubic catheter to drain the bladder if the expected time to ring removal is long or if the patient comes in with an already overly distended bladder.18 Use the information you gathered above to provide valuable information to your urology consultant. Early consultation is recommended as this is a true urologic emergency. This is particularly true if the patient has signs of ischemia on initial exam and we recommend calling urology consultation prior to attempting interventions in the department. Signs and symptoms that should prompt immediate consult include: crepitus, frank necrosis, decreased capillary refill, partial amputation, skin changes suggestive of necrosis/gangrene, pain out of proportion, and hemodynamic instability. While awaiting urology consult, you may try some interventions in the ED which we will discuss below.
Before attempting any interventions, analgesia should be your first step. As mentioned above in the previous case, doing a dorsal penile nerve block should provide excellent pain control to the patient and allow you manipulate the ring and penis without causing too much discomfort. Removal of a penile ring should be thought of in many of the same ways we seek to removal a traditional ring from a finger. It is best to start with simpler and safer methods of removal prior to starting up an electric saw in the ED or OR, although this may ultimately be necessary.
Attempt to use a lubricant such as mineral oil or soap and water to manually remove the ring. If this fails another simple method to try is the “string” method. A quick video on how to do this method can be found here: https://www.youtube.com/watch?v=DrDROoJAF4I. You may need hemostats or pliers to pass the string underneath the ring if there is significant edema. You may elect to also aspirate blood from the corpora cavernosum prior to using the string and/or lubricant methods. This is done by piercing each corpus cavernosa with an 18-gauge needle at the 2 and 10 o’clock positions as if you were draining a priapism. Unlike a priapism, do not attempt to irrigate with saline or infuse with phenylephrine. There is also the option of doing a dorsal T shunt or lateral corpora cavernosa shunt, although this is best discussed with urology as they may elect to perform that procedure in the OR alongside more aggressive ring removal methods.
If the above methods fail, obtain wire cutters, bone cutters, or bolt cutters and attempt to cut through the ring. It is best to place a malleable retractor between the ring and skin if possible to minimize risk of damage to surrounding tissue.16 If you are attempting to use such devices in the ED, the patient should have penile block anesthesia by this point and procedural sedation should be considered as the procedures are very traumatic and anxiety inducing. One other device to use in the ED that may be readily available is the electric ring cutter. Most EDs will carry one of these devices or should have easy access to one. They vary from model to model but at their core they are made of a motor that spins a small circular saw blade. They may include a metal guard to avoid damage to underlying skin but if not, a malleable retractor should be placed under the ring. Alternatively, a finger splint with foam on one side and a metal guard on the other may slipped between the skin and metal in order to protect the skin. Cooling should also be addressed as many electrically powered cutting devices will generate a lot of heat through friction while attempting to cut through the ring and it is strongly recommended that ice water be continuously, gently, poured over the ring while cutting to avoid iatrogenic burns.18,19 If you are unable to safely remove the ring through any of the above mentioned methods, the patient will need to go to the OR where they can be placed under general anesthesia and more powerful devices such as orthopedic drills or angle grinders will be available and can be used in a safe and controlled fashionby the urology team. Depending on the resources of your ED and OR at your hospital, you may need to call on the services of the fire department and see if they have any ultra-high powered saws or grinders which they can bring in for use in the department. Again, this is a diagnosis that carries with it considerable morbidity and mortality if not addressed in a timely fashion. Call for help early, particularly to your urologist on call, and stress the urgency of the diagnosis.
Rapid procedure review:
1: Penile zipper injury
- Determine if the penis is stuck in the sliding mechanism of the zipper or between the teeth.
- Give appropriate analgesia. Great options if patient is without an IV include topical as well as intranasal agents. Penile dorsal nerve block is also a very effective tool.
- If the penis is caught between the teeth, cut across the entire zipper either above or below (preferred and usually easier) the tissue. The zipper teeth should then come apart easily and free the tissue.
- If the penis is caught within the sliding mechanism, multiple modalities should be attempted. This type of zipper injury is much more difficult to relieve and analgesia should thoroughly be addressed. Depending on the patient agitation, they may even require procedural sedation to allow for effective liberation techniques.
- First start with mineral oil or soap and water and try to pull the tissue from the sliding mechanism gently. If this is not successful, attempt to cut the median bar of the zipper with bone or bolt cutters. If you can cut completely through the median bar, the anterior and posterior faceplates will no longer be connected and the zipper can easily be pulled apart. You can also attempt to wedge a screwdriver between the anterior and posterior faceplates and rotate 90 degrees. This should either open up the space between the faceplates enough to pull out the trapped skin or completely disengage the sliding mechanism from the zipper teeth.
- If unable to have success with any method of penile liberation, patient will require urology consultation for possible surgical intervention and/or circumcision.
2: Penile strangulation
- Examine the patient and assess for signs of ischemia. Realize that they may have waited a long time to come in due to fear of embarrassment and may not be forthcoming with duration of injury. If any signs of ischemia are suspected, consult with urology immediately prior to attempts to remove in the ED.
- Multiple methods may be used to remove the penis ring. Attempt lubrication and gentle traction first.
- If unsuccessful, consider the string method presented in the video above.
- If attempts are still unsuccessful, patient will need intervention with heavier tools, start first by utilizing your department’s ring cutter. Remember to give appropriate analgesia and at this point, procedural sedation should also be considered due to the anxiety of the situation. Pour ice water during any attempts to cut the ring off to prevent iatrogenic burns.
- If strong enough machines are not available in the ED, the patient may need to go to the OR for use of surgical grade saws and grinders. Also consider calling local fire department to source removal tools.
- Consider antibiotics, particularly if patient is febrile, has signs of ischemia, or appears septic. Also update tetanus if necessary.
Key Points:
- Penile zipper injuries usually occur in pediatric populations. Identify the type of injury to better help guide which techniques to use to free the penile tissue.
- If the skin is caught between the teeth then cut the zipper above or below and pull apart.
- If it is stuck in the sliding mechanism, you must either release the median bar or use a screwdriver to break the sliding mechanism.
- Be certain to address anxiolysis and pain control adequately.
- Penile strangulation occurs more commonly in adult males and usually linked to rings applied around the penis for pleasure which are now difficult to remove.
- Address removal in a stepwise manner and escalate up through more invasive techniques as mentioned above.
- If unable to remove in the ED, consult with urology and/or fire department for stronger tools to cut through the denser metal rings.
- If there are any signs of organ ischemia, urology should be consulted upon identifying these findings.
References/Further Reading:
- Wyatt JP, Scobie WG. The management of penile zip entrapment in children. Injury. 1994;25:59.
- Reynolds SL, Studnek JR, Bryant K, et al. Study protocol of a randomised controlled trial of intranasal ketamine compared with intranasal fentanyl for analgesia in children with suspected, isolated extremity fractures in the paediatric emergency department. BMJ Open.2016;6:
- Motov S, Drapkin J, Likourenzos A, et al. Sub-dissociative dose ketamine administration for managing pain in the emergency department. World J Emerg Med. 2018;9(4):249-255.
- Steward DJ. Eutectic mixture of local anesthetics (EMLA): what is it? What does it do? J Pediatr. 1993;122:S21.
- Cordoni A, Cordoni LE. Eutectic mixture of local anesthetics reduces pain during intravenous catheter insertion in the pediatric patient. Clin J Pain. 2001;17:115.
- Bjerring P, Arendt-Nielsen L. Depth and duration of skin analgesia to needle insertion after topical application of EMLA cream. Br J Anaesth. 1990;64:173.
- Taddio A, Stevens B, Craig K, et al. Efficacy and safety of lidocaine-prilocaine cream for pain during circumcision. N Engl J Med. 1997;336:1197.
- Lander J, Brady-Fryer B, Metcalfe JB, et al. Comparison of ring block, dorsal penile nerve block, and topical anesthesia for neonatal circumcision: a randomized controlled trial. JAMA. 1997;278:2157.
- Resch K, Schilling C, Borchert BD, et al. Topical anesthesia for pediatric lacerations: a randomized trial of lidocaine-epinephrine-tetracaine solution versus gel. Ann Emerg Med. 1998;32:693.
- Lewis LS, Stephan M. Local and Regional Anesthesia. In: Textbook of Pediatric Emergency Procedures, Henretig FM, King C (Eds), Williams & Wilkins, Baltimore 1997.
- Oosterlinck W. Unbloody management of penile zipper injury. Eur Urol. 1981;7:365.
- Kanegaye JT, Schonfeld N. Penile zipper entrapment: a simple and less threatening approach using mineral oil. Pediatr Emerg Care. 1993;9:90.
- Strait RT. A novel method for removal of penile zipper entrapment. Pediatr Emerg Care 1999;15:412.
- Raveenthiran V. Releasing of zipper-entrapped foreskin: a novel nonsurgical technique. Pediatr Emerg Care 2007;23:463.
- Maruschke M, Seiter H. [Total infarction of the penis caused by entrapment in a plastic bottle]. Urologe A. 2004;43:843–844.
- Noh J, Kang TW, Heo T, et al. Penile strangulation treated with the modified string method. Urology. 2004;64:591.
- Perabo FG, Steiner G, Albers P, et al. Treatment of penile strangulation caused by constricting devices. Urology. 2002;59:137.
- Puvvada S, Kasaraneni P, Gowda RD, et al. Stepwise approach in the management of penile strangulation and penile preservation: 15-year experience in a tertiary care hospital. Arab Journal of Urology. 2019;17(4):305-313.
- Xu T, Gu M, Wang H. Emergency management of penile strangulation: a case report and review of Chinese literature. Emerg Med J. 2009;26(1):73-74.







