
A 43-year-old male with past medical history of hypertension, hyperlipidemia, and GERD presents to the ED with swelling to the right armpit. He also endorses a small wound to his right forearm, fatigue, mild muscle aches, and low-grade fever.
Initial vital signs include BP 125/78, HR 67, RR 16, SpO2 99% on RA, T 37.1. On exam, he is well-appearing, has right axillary lymphadenopathy, and a small, non-tender, slightly raised erythematous lesion to the right forearm with no overt evidence of extensive cellulitis.
On further questioning, the patient states that he was playing with the neighborhood cat a little over a week ago. He believes the cat bit him on the arm before running off. He is unsure if the cat is up to date on vaccines and has not seen the cat since. He only sees the cat sparingly and believes it may be difficult to locate. The patient does not remember his last tetanus vaccination.
Question: What is the diagnosis?
Answer: Cat-Scratch Disease
Background
- Also known as cat-scratch fever
- Initially described in the 1930s
- Association with cats identified in the 1950s
- Douglas Wear, a pathologist, described a new bacterium in the lymph nodes of cat-scratch patients (1)
Etiology
- Caused by the bacteria Bartonella Henselae, a fastidious intracellular gram-negative bacillus, needing Warthin-Starry silver stain to visualize, carried by cats
- Cats acquire the bacteria from a bite from the cat flea (Ctenocephalides Felis)
- The infected cat is not symptomatic
- In humans, infection affects regional lymph nodes draining the area of inoculation (1)
Epidemiology (1)
- Mild illness in immunocompetent hosts
- 55% of cases are in children < 18
- 60% of cases are in males
- > 50% of cases occur from September-January in the U.S.
- 56% of cats with this infection are less than 1 year old
- Bartonella Henselae is hard to culture but can be detected by PCR
- Infection usually from scratch, bite, or infected saliva through broken skin
Clinical Presentation
- History of cat (normally kitten) exposure
- Usually about 1-2 weeks after exposure
- Lymphadenitis proximal to exposure site
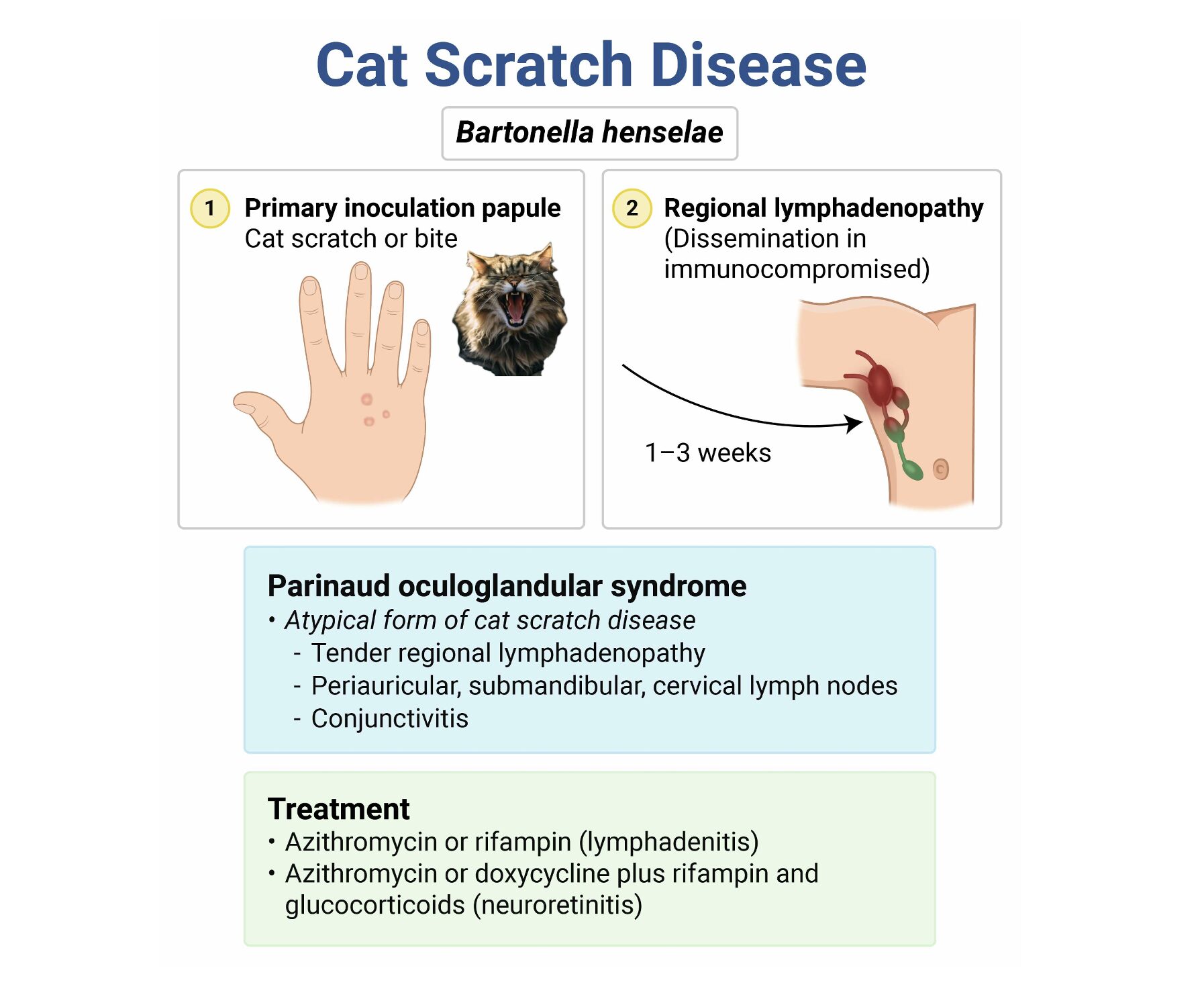
- Parinaud’s oculoglandular syndrome
- Caused by inoculation of the eye
- Conjunctivitis, ocular granuloma, periauricular adenopathy
- Immunocompromised patients or children
- Found in 2-8% of children with cat-scratch disease
- Conjunctivitis usually resolved within weeks, whereas preauricular adenopathy can persist for months (2)
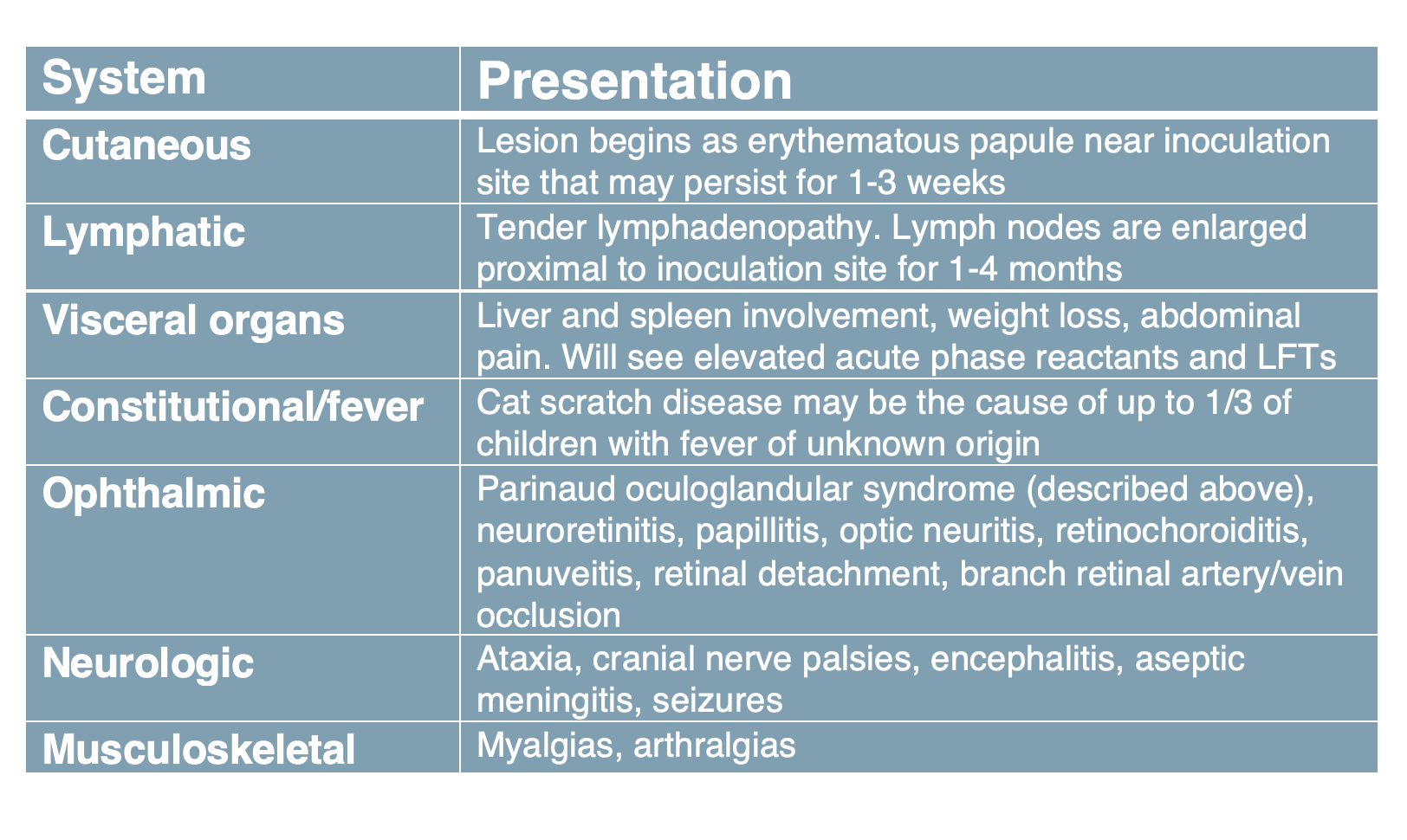
- 85-90% of children have self-limited lymphadenopathy with fever
- Immunocompromised patients, very young, elderly
- More likely to have systemic disseminated disease including cutaneous, lymphatic, ocular, neurologic, MSK, visceral organ involvement
Evaluation/Diagnosis
- Diagnosis is clinical based on symptoms and history
- Bartonella henselae is difficult to culture
- Cat exposure usually required for diagnosis
- Serologic testing may confirm diagnosis with EIA or IFA, but negative tests do not rule out diagnosis
- Lymph node biopsy is usually not indicated but may be considered if diagnosis is unclear
- Tissue can be obtained by needle aspiration with US to obtain tissue
- Excision of affected lymph nodes not recommended due to risk of fistula formation
- Labs may show elevated acute phase reactants and elevated liver enzymes
- Differentials include CMV, HIV, EBV (these viral agents usually cause diffuse rather than localized lymphadenopathy. Similar skin findings can be found in fungal infections, leishmaniasis, and nocardiosis (1)

Treatment
- Adult (> 45 kg): azithromycin 500 mg PO x1, 250 mg/day x4 days
- Child (<45 kg): azithromycin 10 mg/kg x1, 5mg/kg/day x4 days
- Can also use doxycycline (4), can be considered in persistent cases, or when complications develop such as encephalitis, eye involvement, or in other disseminated cases. Can use 100 mg PO BID for at least 14 days in severe cases (5)
- Tdap if patient is not up to date, recommended if it has been more than 5 years since last vaccination (6)
- Rabies vaccine and immunoglobulin if rabies status of the cat is unknown (7)
- 1 mL IM of rabies vaccine on days 0, 3, 7, 14. Give in deltoid, not buttock since Ab is not created in fat cells
- Rabies immunoglobulin 20 IU/kg subcutaneous, infiltrating wound, placing remainder in opposite arm of vaccine (7)
Prognosis
- 90-95% of children with cat-scratch disease will resolve with supportive care only (analgesia, antipyretics, warm compresses)
- In patients with disseminated disease, may take months to a year to heal depending on existing comorbidities and depending on which system is involved
- More likely in immunocompromised patients (1)
Pearls
- Cat-scratch disease is a common cause of lymphadenopathy, especially in pediatrics
- A thorough history and physical will aid in the diagnosis
- Age and comorbidities should be considered when discussing prognosis
- Prevention of the disease requires flea control and supervision of kids around kittens
- Don’t forget Tdap
- Don’t forget to consider rabies immunization/immunoglobulin (the patient in this vignette would qualify for both the vaccine and immunoglobulin)

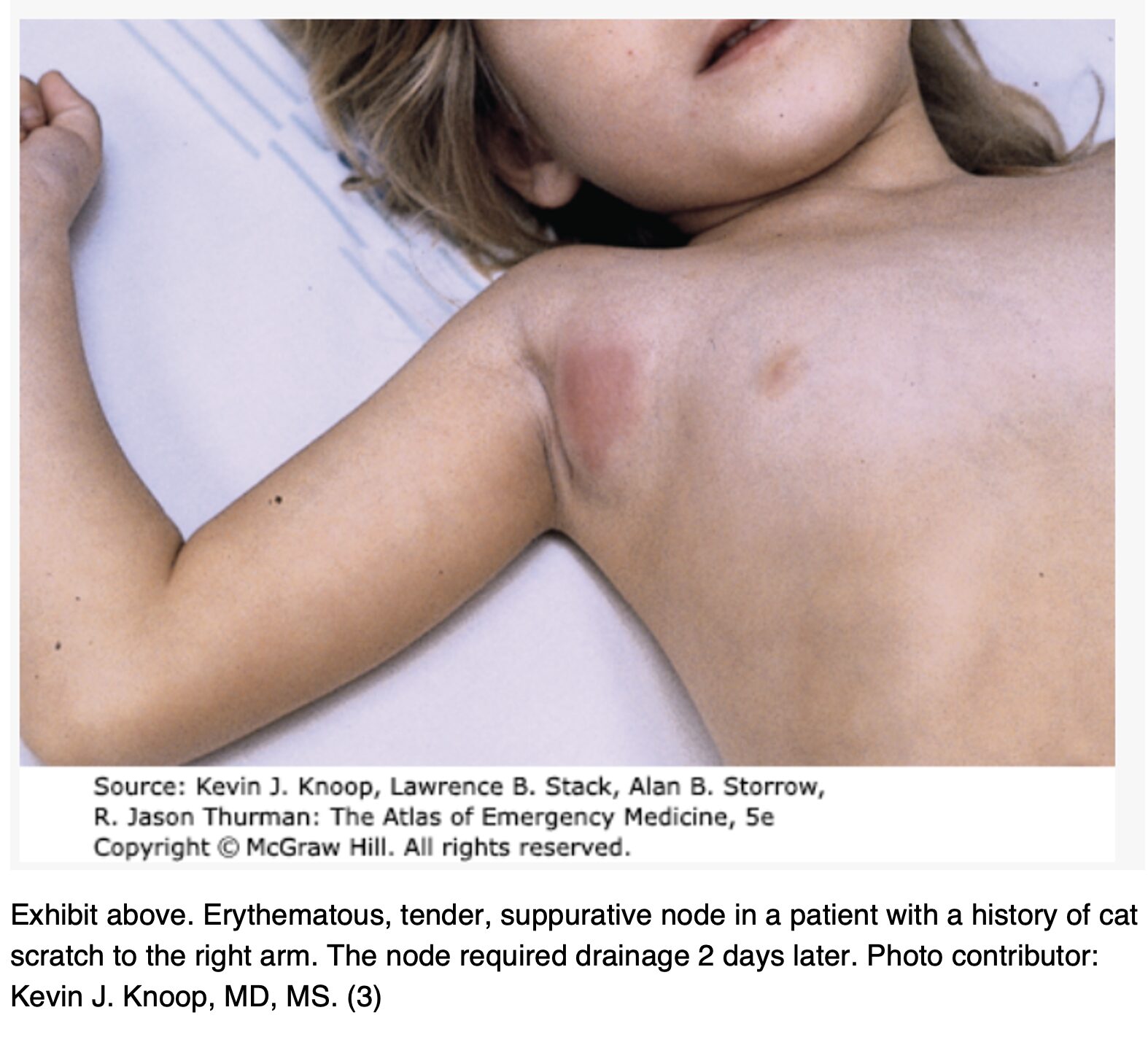
A 12-year-old patient presents to the ED for evaluation of a swollen lump in the axilla, as shown above. The swelling has been present for about 3 weeks, is painful, and seems to be increasing in size. The patient has had intermittent fevers as high as 100.9°F (38.3°C) and increased fatigue. There is no one at home with similar symptoms. The patient lives with their parents, siblings, two dogs, and a kitten. The physical exam is notable for a 4 cm swollen area in the axilla that is tender to touch, erythematous, warm, and indurated. BP is 110/65 mm Hg, HR is 90 bpm, RR is 16/min, and T is 99.9°F (37.7°C). Which of the following organisms is the most likely cause of this patient’s symptoms?
A) Bartonella henselae
B) Sporothrix schenckii
C) Staphylococcus aureus
D) Streptococcus pyogenes
Correct answer: A
This patient is exhibiting typical findings of cat scratch disease (CSD), caused by the bacteria Bartonella henselae following a cat bite or scratch. Most cases occur in people < 20 years of age, and a history of recent contact with a cat (most often kittens or feral cats) is present in almost all cases. The incubation period may be 5–50 days before the appearance of skin findings or regional lymphadenopathy. Skin manifestations include a scratch or bite with surrounding pustules or papules, which can be small and easily overlooked. The most common physical exam finding is regional lymphadenopathy of 1–5 cm, present in almost all cases, and is most often a single node but can involve multiple lymph nodes in some cases. The involved lymph nodes are typically tender, erythematous, warm, and indurated. The axillary, cervical, submandibular, preauricular, epitrochlear, femoral, and inguinal lymph nodes are the most commonly involved sites. Patients may also experience symptoms of low-grade fever, malaise, fatigue, anorexia, and headache. CSD can rarely cause more severe symptoms of persistent fever, maculopapular rashes, aseptic meningitis, encephalitis, hepatitis, pneumonia, microabscesses in the liver and spleen, osteolytic lesions, and thrombocytopenic purpura.
Lymphadenopathy from CSD typically lasts several months but may last up to a year. It tends to resolve spontaneously, but in patients with severe, painful lymphadenopathy, a 5-day course of azithromycin may decrease swelling and speed up resolution. Suppuration of involved lymph nodes can occur and may be drained with needle aspiration. Incision and drainage should be avoided due to the risk of fistula formation. For ill patients with systemic symptoms, antibiotic therapy with oral azithromycin, trimethoprim-sulfamethoxazole, or ciprofloxacin is often recommended. No treatment or quarantine of cats who transmit CSD is recommended, but patients should be counseled regarding hand washing after animal contact.
Sporothrix schenckii (B) is the causative organism in sporotrichosis infections. It is associated with a rash that can last weeks to months and may spread along lymphatic channels and cause lymphadenitis. This patient does not have a rash suggestive of sporotrichosis or the expected history of inoculation through agricultural exposure.
In cases of CSD, abscess formation with an involved lymph node may occur and can be confused for an abscess caused by Staphylococcus aureus (C). The clinical history of a longer duration of symptoms and the lack of fluctuance in a swollen lymph node suggest CSD rather than an acute abscess.
Streptococcus pyogenes (D) can cause cellulitis, streptococcal pharyngitis, and impetigo that may have mildly associated lymphadenopathy but not to the degree seen with CSD.
Further reading:
Cat-Scratch Disease | The Atlas of Emergency Medicine, 5e | AccessMedicine.
Sources:
- Baranowski K, Huang B. Cat Scratch Disease. Nih.gov. Published June 12, 2023. https://www.ncbi.nlm.nih.gov/books/NBK482139/
- Nelson CA, Saha S, Mead PS. Cat-Scratch Disease in the United States, 2005–2013. Emerging Infectious Diseases. 2016;22(10):1741-1746. doi:https://doi.org/10.3201/eid2210.160115
- Shah A, Sobolewski B, Mittiga MR. Cat-Scratch Disease. McGraw Hill Medical. Published 2025. Accessed August 12, 2025. https://accessmedicine.mhmedical.com/content.aspx?bookid=2969§ionid=250460409
- Klotz SA, Ianas V, Elliott SP. Cat-scratch Disease. American Family Physician. 2011;83(2):152-155. https://www.aafp.org/pubs/afp/issues/2011/0115/p152.html
- Rolain JM, Brouqui P, Koehler JE, Maguina C, Dolan MJ, Raoult D. Recommendations for Treatment of Human Infections Caused by Bartonella Species. Antimicrobial Agents and Chemotherapy. 2004;48(6): 1921-1933. doi:https//doi.org/10.1128/aac.48.6.1921-1933. 2004
- Ellis R, Ellis C. Dog and Cat Bites. American Family Physician. 2014;90(4):239-243. Https://www.aafp.org/pubs/afp/issues/2024/0815/p239.html
- Koury R, Warrington SJ. Rabies. PubMed. Published 2022. https://www.ncbi.nlm.nih.gov/books/NBK448076/




