
Author: Lloyd Tannenbaum, MD (EM Attending Physician, APD) // Reviewer: Brit Long, MD (@long_brit)
Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations.
Disclaimer: This is a fictional case and morbidity and mortality conference. This case did not happen.
ER Chairman, Dr. Sullivan: “Good morning. For this month’s Morbidity and Mortality (M and M) Conference, we will be discussing a recent death in the emergency room. Joining us today, in addition to my ER colleagues, we have representatives from the departments of congenital cardiology, cardiac anesthesia, critical care, and pharmacy. Our case today involved patient, JM, who was a 32-year-old male coming into the ER complaining of shortness of breath. Dr. Jackson, he was your patient, please present this case to the room. As with all M and M conferences, please remember that everything discussed is confidential and designed for honest reflection and growth, not blame. For those of us in attendance today who are not part of the ER, please feel free to interrupt Dr. Jackson as he presents to ask any clarifying questions as needed. Go ahead Dr. Jackson.”
Dr. J: “Thank you Dr. Sullivan. And thank you to my colleagues both from the ER and from other departments who have taken time out of their busy day to discuss our care. This was a tough case; one that I think will really benefit all of our departments from reviewing. Patient JM presented to the ER during a busy Friday night shift by car. It was around 8 pm when he checked in. He was initially triaged as a level 1 patient, meaning that he needed to get brought back from the waiting room, ideally as soon as possible. Looking over the nurse’s triage notes, she wrote that the patient was complaining of shortness of breath for the past 3-4 days, but it was getting progressively worse, to the point that he could no longer speak in full sentences. Nursing notes mention that they called for a stat bed, but unfortunately, none were available. One was being cleaned, however, and it was reserved for JM. Triage vitals show an O2 sat of 78% on room air, heart rate of 126, respiratory rate of 27, blood pressure of 140/83, and a temperature of 37 degrees Celsius (98.6F). Once vitals were obtained, nursing again called for a stat bed, placed the patient on oxygen (6L NC), and alerted respiratory therapy to be on standby. The patient remained in the triage room for an additional 5-7 minutes until the room was available, during which time an ECG was performed. After completing the ECG, the patient was wheeled immediately to the room and nursing asked me to come over and look at him right away.”
Dr. J: “I met the patient at the room and saw an early 30s-year-old male in distress. He was short of breath. He had audible rales and rhonchi from across the room and looked unwell. I called RT to the bedside and asked them to get BPAP ready, as the patient appeared to be in some kind of heart failure exacerbation or volume overload state. When I tried to get more history from him, he kept saying, ‘I can’t breathe! I … Can’t … Breathe!’ He was able to tell me that his mother was on her way, and he kept pointing to his chest and said ‘Tan! Tan!’ but we weren’t sure what that meant. At this time, the tech handed me his ECG, which I have enlarged and displayed on the screen. If you’d all please take a second to review his ECG:”
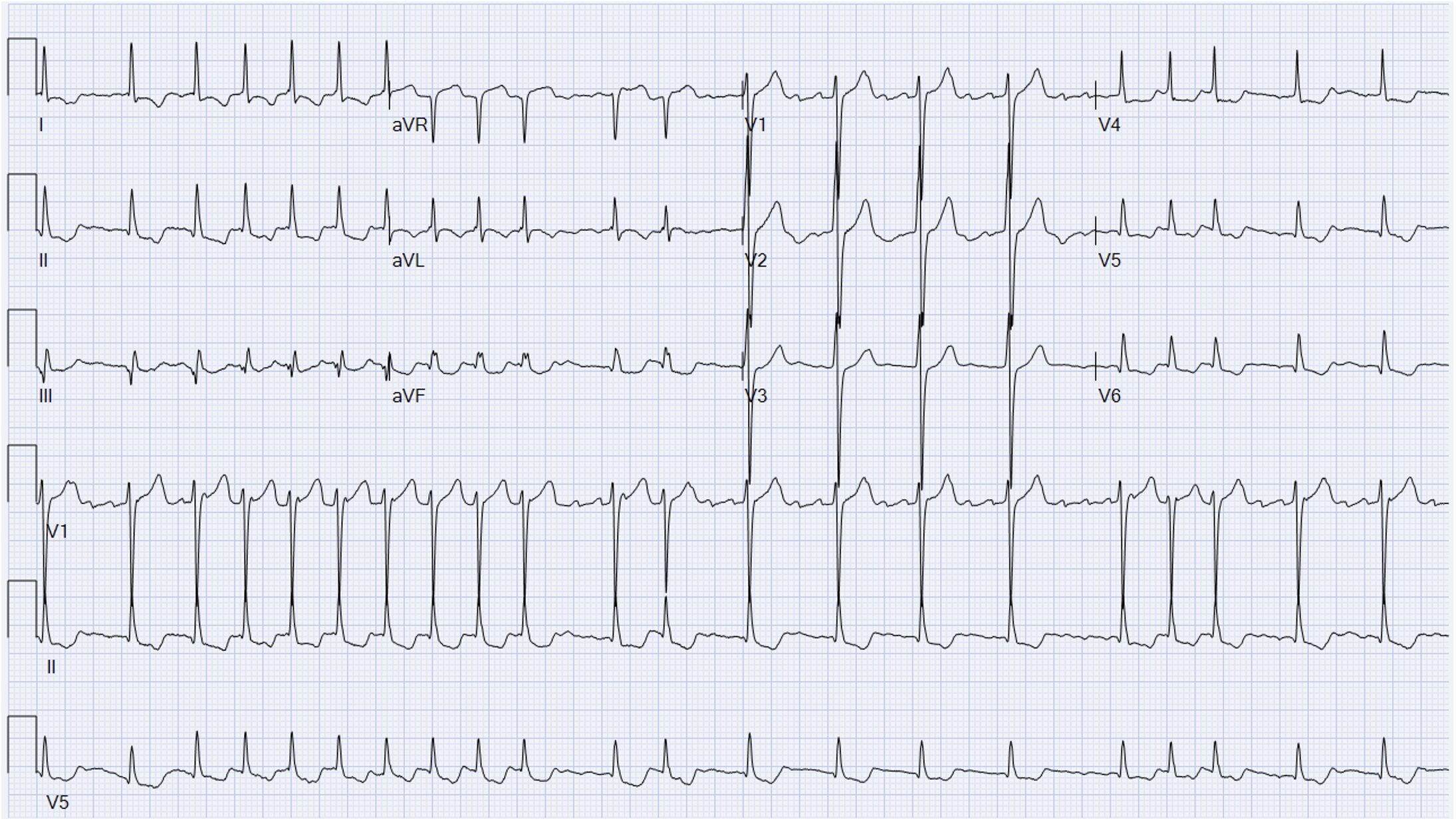
Dr. J: “I interpreted the ECG as:
Rate: 126 bpm
Rhythm: irregularly irregular, but with P waves; very confusing
Axis: Normal
Intervals: Narrow QRS, variable PR, sometimes PR not present
Morphology: Some ST segment depressions, some ST elevation in AVR, likely some strain going on
Final read: I read this ECG to show some kind of atypical atrial rhythm with signs of strain. Given the P wave’s axis, they aren’t coming from the SA node. I was concerned for possible multifocal atrial tachycardia (MAT), but all of the P waves looked the same, making MAT less likely.”
Dr. J: “At this time, the nurse had pulled up JM’s chart, and as I finished looking at the ECG, I heard her say, ‘He has a Fontan and a history of hypoplastic left heart syndrome.’”
Dr. Kimber: “Pardon me, may I interrupt for a second? I’m Dr. Kimber from the department of congenital cardiology. I’d like to just spend a few seconds going over this ECG; I think there are a lot of good learning points to take away from it. You are correct; this is an atypical atrial rhythm, likely atypical flutter. Fontan patients are at high risk for atrial dysrhythmias, stemming from years of stretch being placed on their atria, given their abnormal cardiac mechanics. Typical flutter usually presents as a circuit around the tricuspid valve and tends to have a predictable rate. For atypical flutter, as often seen in these patients, it can be irregular since the circuit isn’t around the tricuspid. Remember, Fontan patients are very sensitive to atrial dysrhythmias, Dr. Jackson, what happened next?”
Dr. J: “Thank you Dr. Kimber. At this point, I think we all knew JM was in trouble. Once we recognized that he was a Fontan patient, we took the BPAP mask off of him immediately and I asked the charge nurse to stat page the congenital team. I think the BPAP was only on him for 30-60 seconds. RT had just finished setting it up when I ripped it off of him. I know how sensitive Fontan patients are to positive pressure ventilation. We placed a non-rebreather (NRB) mask on JM and cranked it up to 15L. Also, we tried to get more history out of JM, but he was so short of breath, he could barely talk. We did finally figure out that “Tan” and pointing to his chest meant that he is a Fontan patient, but unfortunately, Mom still had not arrived. Right around now, stat labs were being run, and I took a look with the ultrasound. I’ve blown up some images on the screen ahead to review:”





