Author: Anna Pickens, MD (@AnnaEMin5, Creator of EM in 5) // Edited by: Alex Koyfman, MD (@EMHighAK), Brit Long, MD (@long_brit), and Manpreet Singh, MD (@MprizzleER)
Welcome to this week’s edition of EMin5 by Dr. Anna Pickens. Today we are focusing on the 4 types of shock.
Video:
To better understand and manage patients in shock, we can think about splitting them into 4 categories: Hypovolemic, Cardiogenic, Distributive, Obstructive.

Let’s go through each type…
Hypovolemic:

This is an issue with low circulating volume and includes patients who have been bleeding, vomiting, having diarrhea, or are generally volume down.
Cardiogenic:
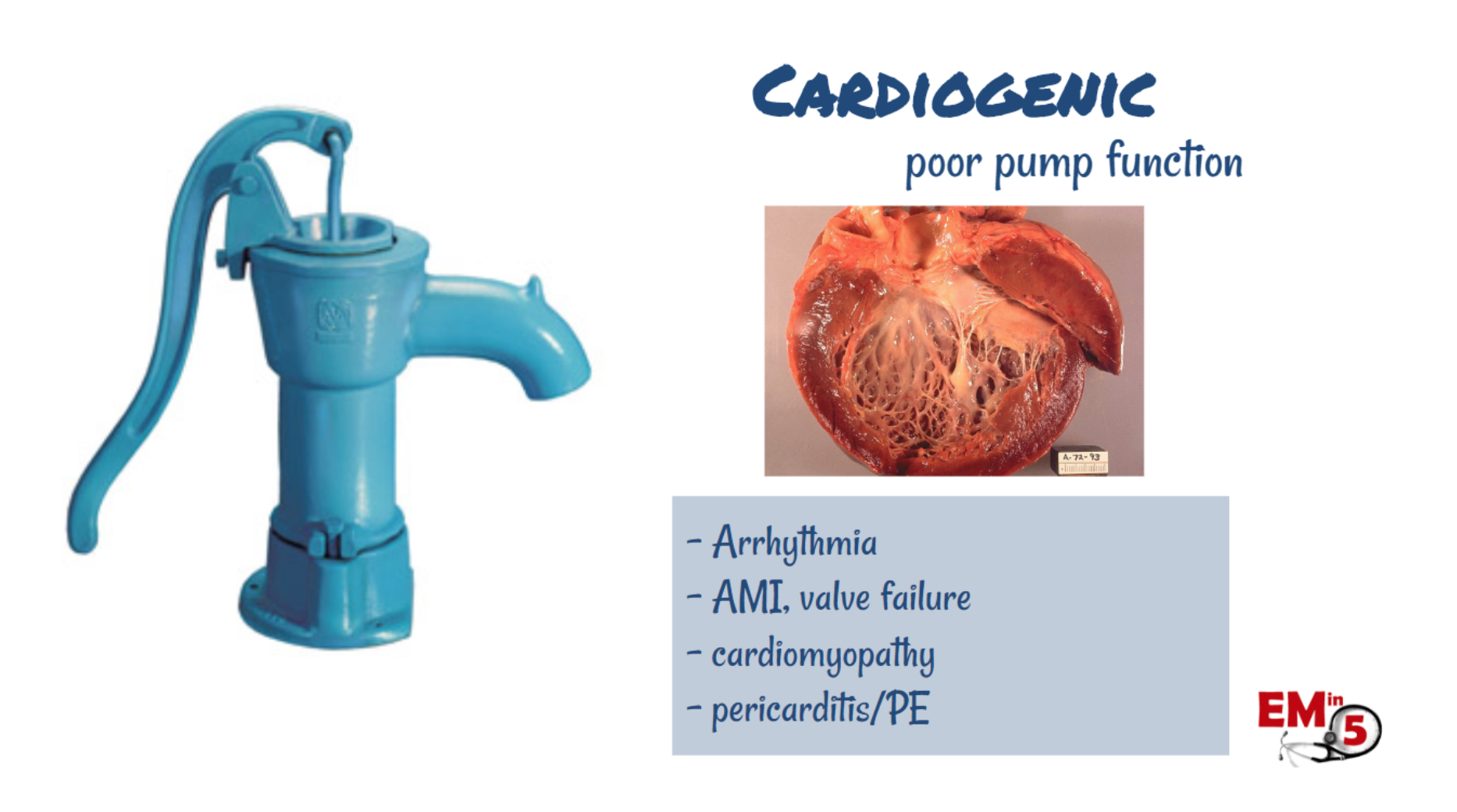
This is a problem with poor cardiac pump function, and can be caused by a number of different things including acute MI, valve failure, arrhythmias, cardiomyopathy, and pericarditis/myocarditis.
Distributive:
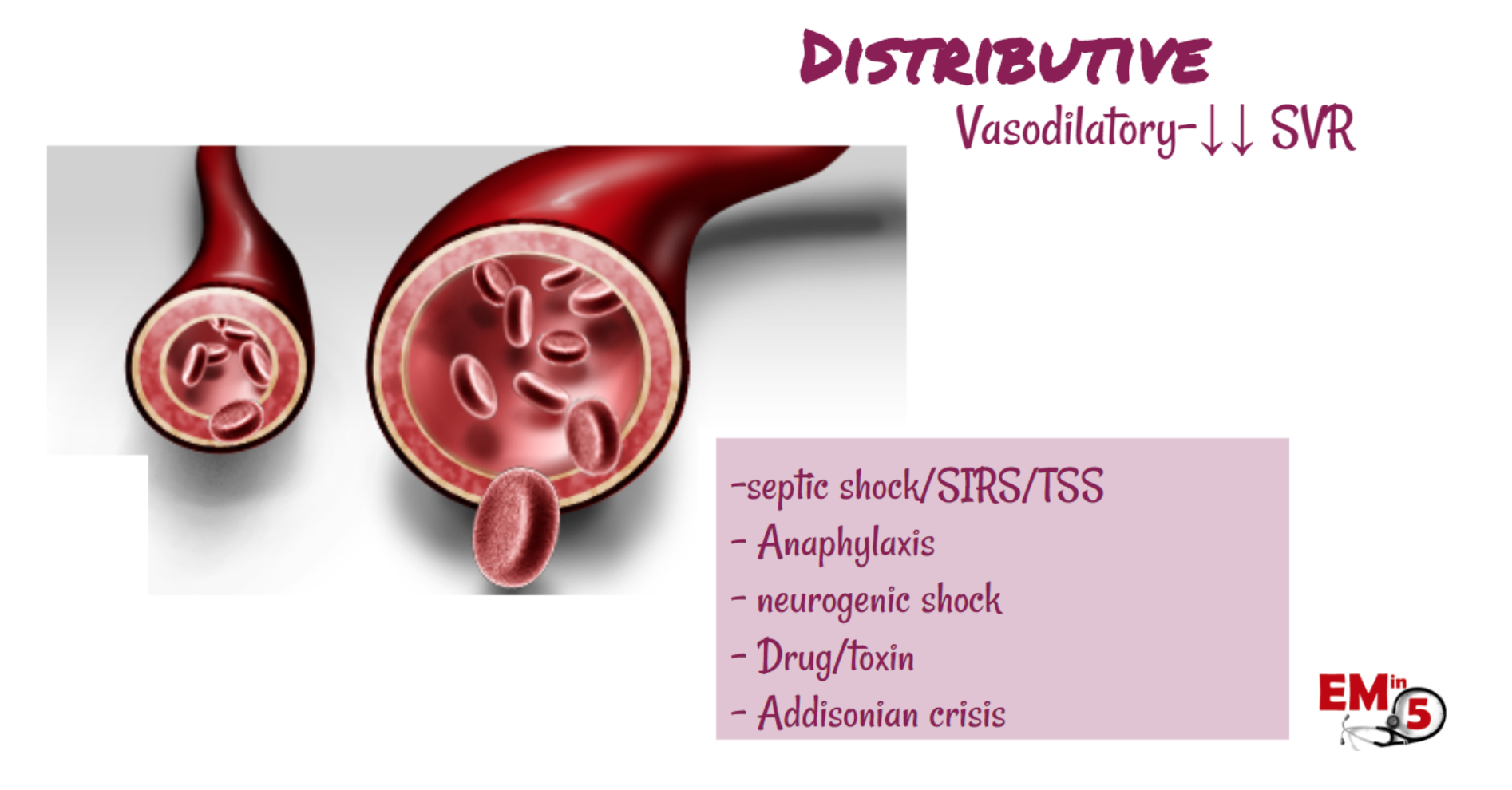
This is the one that we probably think about most commonly, and includes a wide range of categories. But they all share something in common, and therefore are managed in a similar fashion – they all have a problem with severe peripheral vascular vasodilation. Examples include sepsis, anaphylaxis, neurogenic shock, and various drugs and toxins.
Obstructive:

In this type of shock, there is no problem with the peripheral vasculature or the heart – it’s a problem with something obstructing the flow of blood. For example, a PE, tamponade, or a pneumothorax.
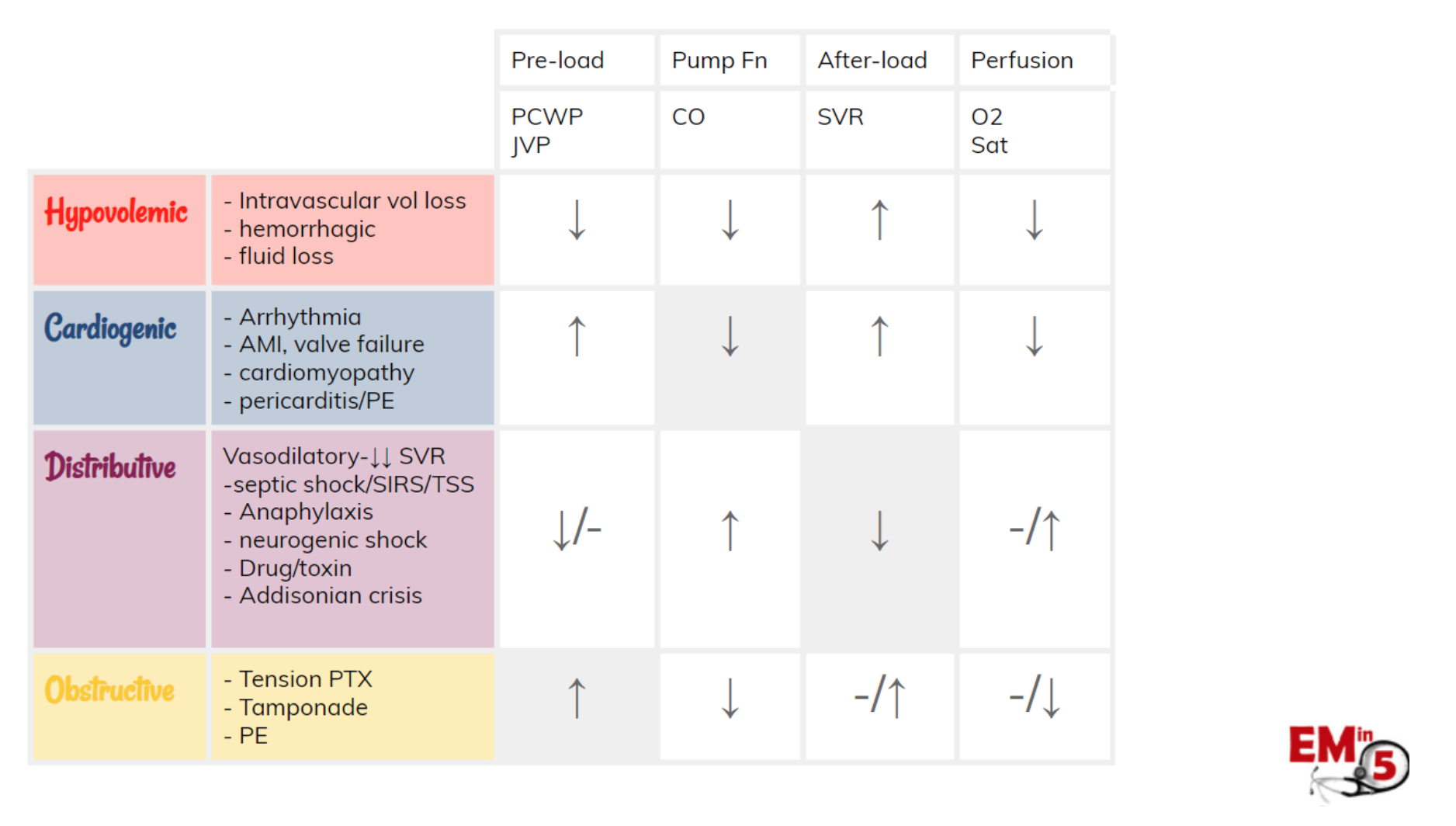
Here’s a summary of how these 4 types of shock affect the circulatory system:
Once we have decided what type of shock we are dealing with in our patient, we can start to think about how to treat it.
- Hypovolemic shock needs fluids or blood transfusions.
- Cardiogenic shock can be very difficult to manage, but to give a general summary, you usually need to treat with a delicate balance of fluids (go slow!), norepinephrine (vasoconstriction) and dobutamine (inotrope).
- Distributive shock treatment needs to target the peripheral vasculature, so pressors it is!
- Obstructive shock needs a specific problem fixed. If your patient has a pneumothorax or tamponade, it needs a needle. If your patient has a PE, consider heparin, thrombolytics or thrombectomy. In each of these cases, you can usually start with some fluids (preload dependent) to stabilize the blood pressure while you take your definitive actions.

Suggested/Further Reading:
Articles/Posts:
- emDOCs – PEM Playbook – Approach to Shock
- emDOCs – The Hypotensive ED Patient: A Sequential Systematic Approach
- First 10 EM – Undifferentiated Hypotension
- CDEM – Approach to Shock
- EMJ-BMJ – Critical care in the emergency department: shock and circulatory support
- EM Practice – Diagnosis And Management Of Shock In The Emergency Department





