Today on the emDOCs cast with Brit Long (@long_brit), we cover angioedema.
Episode 133: Angioedema
What is it?
- Non-pitting, non-dependent, transient edema affecting the skin and mucous membranes; due to accumulation of vasoactive substances (e.g., bradykinin, histamine).1-8
- Results in increased vascular permeability with swelling of the deep dermal, submucosal, and subcutaneous tissues of the face, neck, lips, oropharynx, extremities, urogenital tract, and gastrointestinal tract.
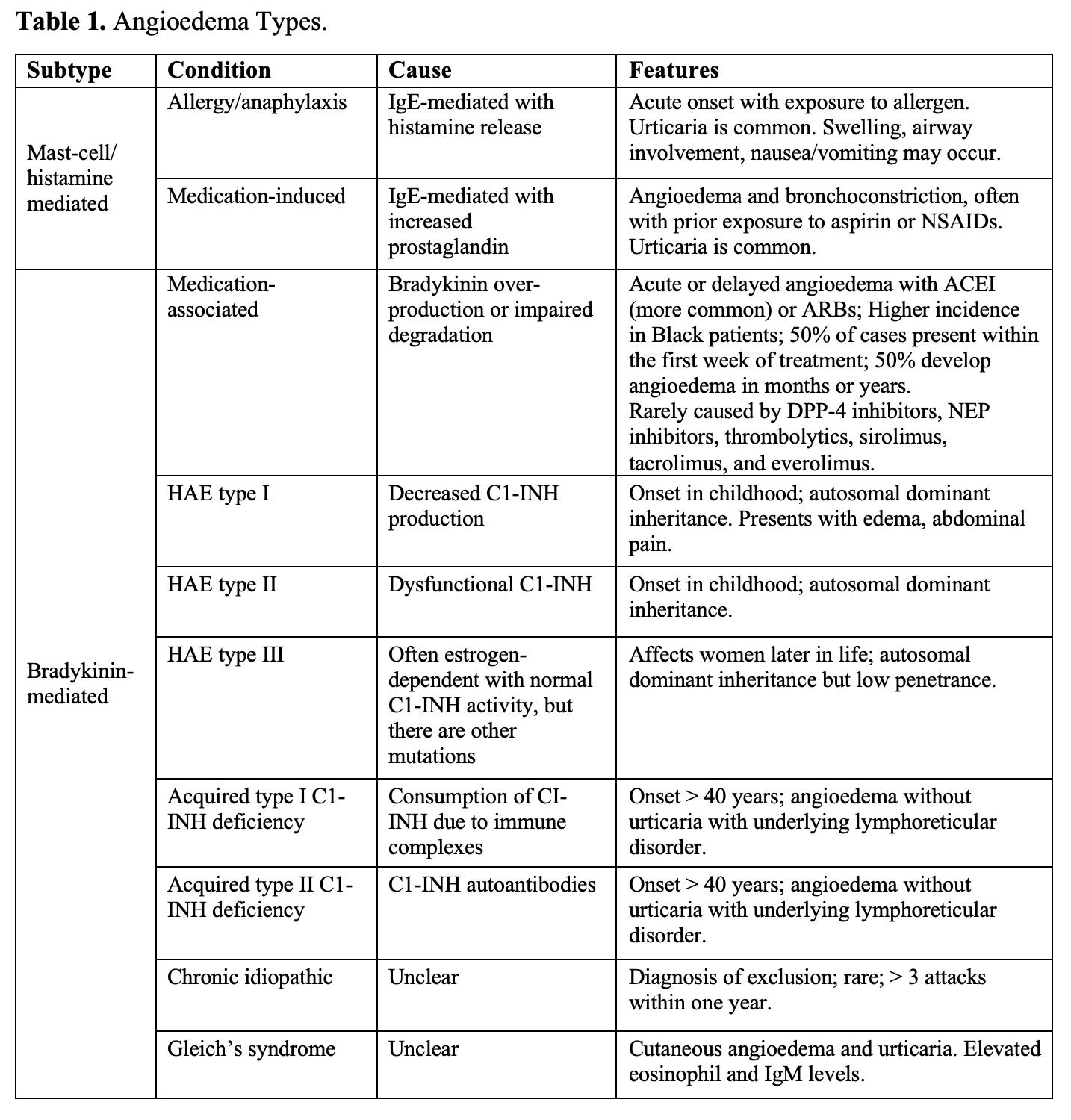
- Angioedema may be categorized several ways: bradykinin mediated versus histamine mediated and hereditary (bradykinin-mediated) versus acquired (bradykinin- or histamine-mediated).
- Type affects the clinical presentation and the treatment.
How common is this?
- Up to 117,000 ED visits for angioedema annually; up to 30% of patients with angioedema use the ED at least once during their lifetime.17-21
- Histamine-mediated angioedema most common form (40-70% of cases). Second is drug-induced angioedema (most commonly angiotensin-converting enzyme inhibitors; develops in less than 0.7% of patients), and third hereditary angioedema (estimated prevalence of 1-in-50,000 persons).1,2,4,5,8,12,20,31
- Most patients with hereditary angioedema have first episode between 4-26 years.32-35
- If not treated, angioedema can result in significant morbidity and mortality, especially with laryngeal involvement which may cause airway obstruction (mortality rates 15-56%).9,36,37
How should we assess these patients?
- First step: assess airway, cardiovascular system, mental status.
- Asphyxiation most common cause of mortality with acute angioedema1,14,38-40 Up to 15% experience airway obstruction; may progress rapidly.1,4,6,16,39,40
- Over half of patients with hereditary angioedema experience at least one episode of laryngeal edema during their lifetime; accounts for over 30% of deaths.39,40
- Look for lip and tongue swelling, pharyngeal swelling, change in voice (hoarseness, stridor), drooling, difficulty swallowing, shortness of breath, and inability to lie flat. Ask about lightheadedness, pruritus, rash, and GI symptoms (pain, vomiting, diarrhea).3,4,14,33-35
- Obtain history of prior angioedema attacks and treatments, medications, and family history.
- Assess for exposure to a trigger.
- Stress, medical procedures, trauma, infection, and medications (hormone therapies, oral contraceptives, opioids).3,4,14,16,35,41
- Exam: assess for swelling of the lips or face and evidence of airway obstruction (swelling of the tongue, floor of the mouth, and palate).3,4,14,35,43
- Several studies evaluate common findings in angioedema.
- 2025 retrospective study of ACEI-induced angioedema found lip swelling occurred in 87.5% and tongue swelling in 43.6%42
- Study of 311 patients found several factors were associated with need for airway intervention: presentation within 4 hours of symptom onset; signs/symptoms including dysphagia, dysphonia, drooling, respiratory distress, and globus sensation; and involvement of the tongue, soft palate, vallecula, aryepiglottic folds, and true vocal cords.43
- 2020 study found rapid progression of symptoms within 6 hours of angioedema onset, anterior tongue swelling, voice changes, drooling, and dyspnea were associated with intubation in ACEI-induced angioedema; isolated lip swelling was not.44
- Non-pitting edema may affect the head, neck, extremities, genitals, or abdomen; edema is typically non-contiguous.1-7,10,11,45,46
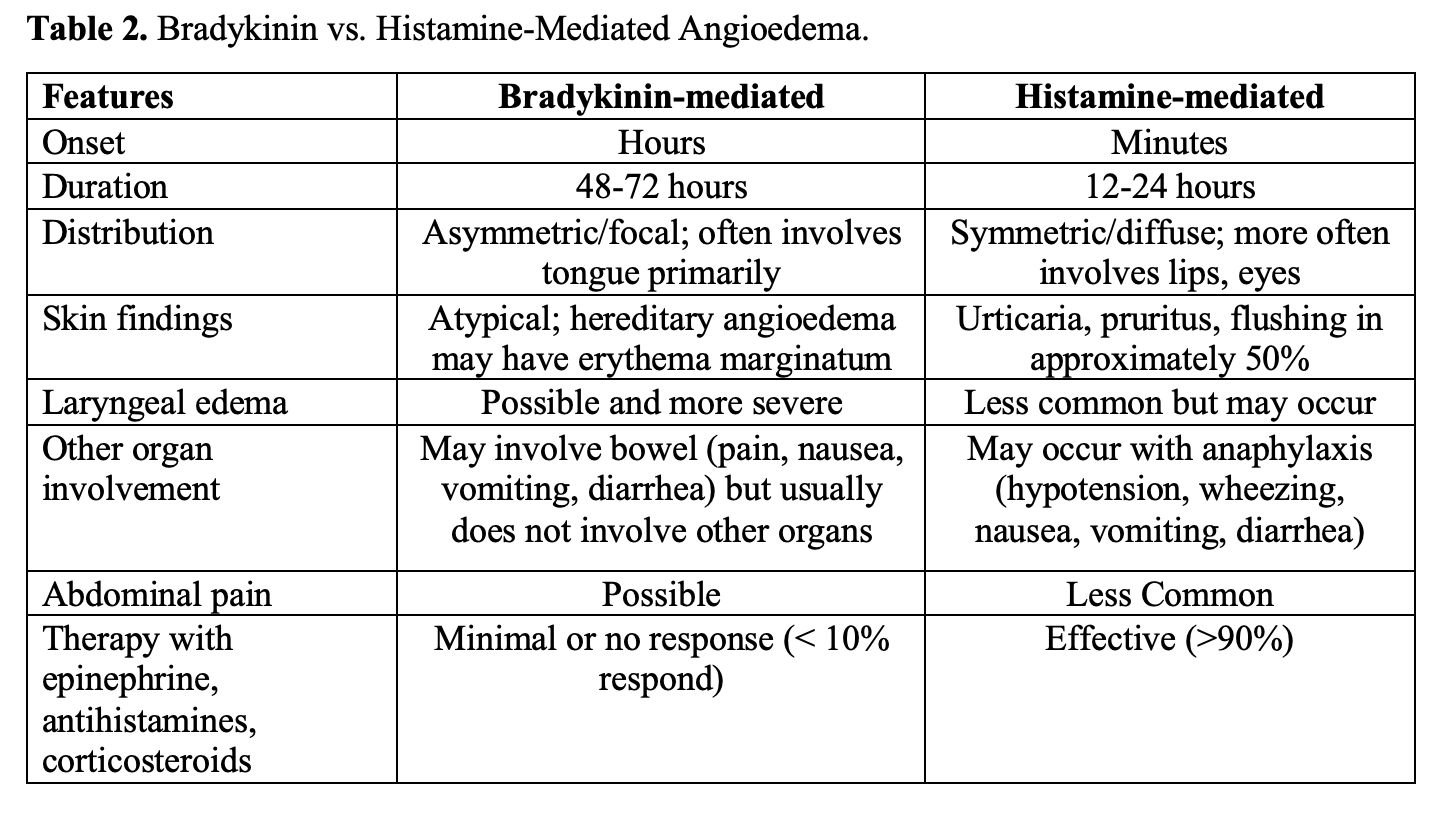
- Histamine mediated form may present with urticaria and pruritus (less common in bradykinin-mediated angioedema, though may develop erythematous rings known as erythema marginatum).22,38,47,48
- Abdominal symptoms may occur.
What should we be focusing on for the ED evaluation?
- Focus on the airway; in those with swelling of the tongue, floor of the mouth, or soft palate on initial examination, flexible endoscopy/scope is best means of assessing airway edema.
- May also use hyperangulated or standard geometry video laryngoscopy with appropriate topical analgesia to visualize the glottic structures if flexible endoscopy not available.
- X-ray/CT can reveal tongue, glottic, and airway swelling; do not use these to assess airway integrity if concerned about imminent airway obstruction.52
- POCUS has been evaluated with the high frequency linear transducer in the submandibular region; evaluate for airway edema as move the probe in the transverse orientation until the anterior base of the neck is reached.53-55
- Laboratory testing will no change management in isolated angioedema; outpatient testing can include C4, C1 esterase inhibitor (C1-INH), and tryptase levels.
Where do we start with management?
- If evidence of airway obstruction (stridor, drooling, dyspnea, marked edema in the larynx), need definitive airway. If angioedema involves the external face and lips only; airway intervention is rarely needed.49,50,56-61
- Do not wait for angioedema specific medications if intervention necessary, but while preparing for intubation, may attempt inhaled epinephrine.
- If you have 15-20 minutes, consider awake intubation strategy with flexible intubating endoscopy.
- If not feasible, use video laryngoscopy.
- When intubating, avoid excessive physical manipulation (worsens airway edema).
- Prepare for surgical airway. Cricothyrotomy or tracheostomy is needed in up to 50% of patients with angioedema who need emergent airway intervention. Use double set up.
- Consider using non-invasive positive pressure ventilation to temporize the patient and for preoxygenation, but this is not a long-term solution.
- Supraglottic airway devices may be displaced due to progressive swelling and may worsen airway edema.1,3,6,10,14,56,64
What medications are available?
- If unsure of etiology or concerned for histamine-mediated angioedema: administer epinephrine, antihistamines, steroids.1,3,4,14,65
- These medications are not usually effective in bradykinin-mediated forms.
- Allergy guidelines recommend against their routine use in patients with a definite diagnosis of bradykinin-mediated angioedema (they have not been shown to be effective, but they have not been associated with harm).1,3,4,33,38,66
- For known bradykinin-mediated angioedema (e.g., hereditary angioedema), there are several available medications that reduce the production or activity of bradykinin (peptide that increases vascular permeability and inflammation).3,4,33,66-72
- Administer as soon as possible in bradykinin-mediated angioedema.
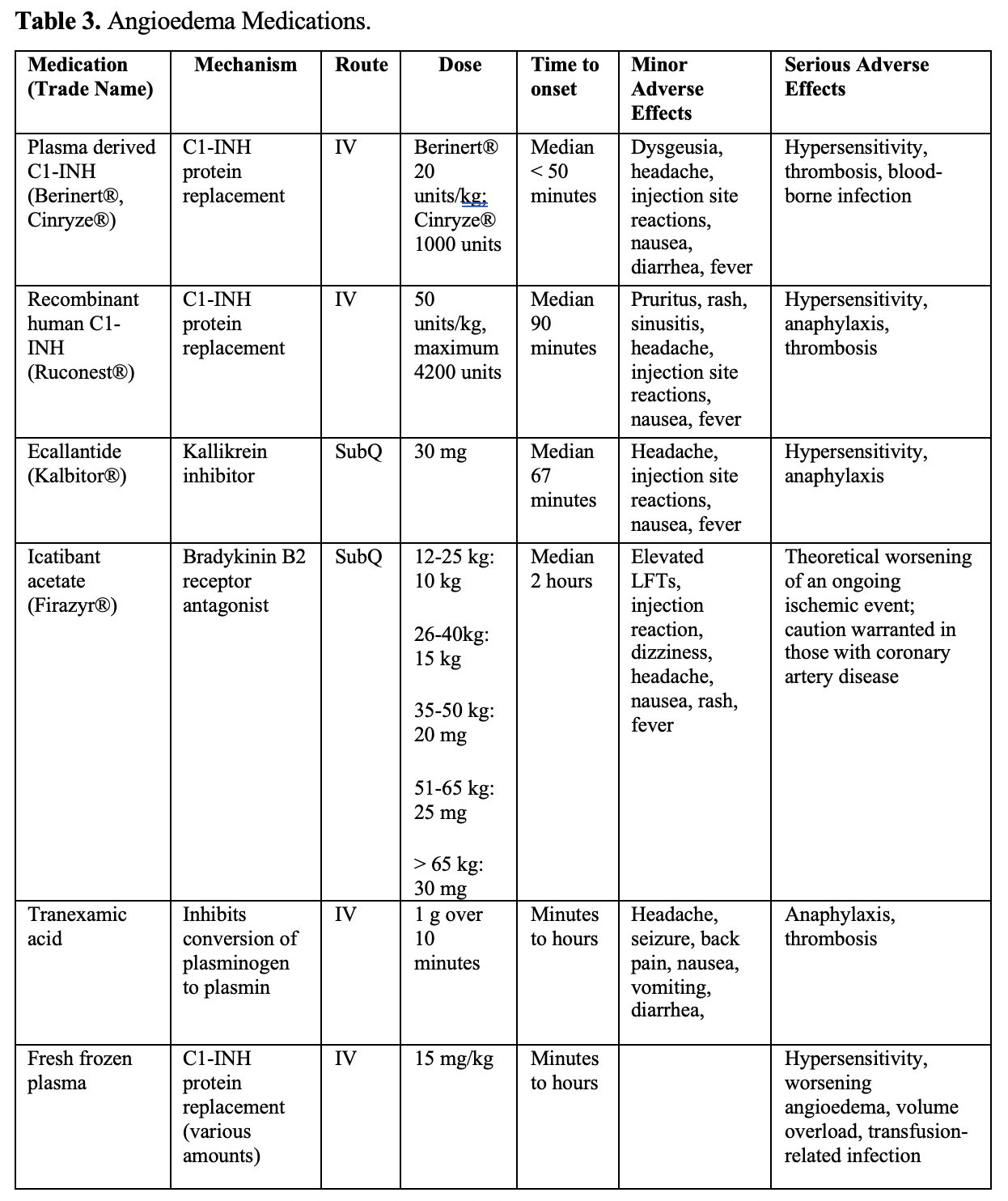
- C1 esterase inhibitor (C1-INH) replacements: inhibit proteases like kallikrein and the complement system to reduce bradykinin production (Berinert®, Cinryze®, Ruconest®).68-70
- Kallikrein inhibitors: reduce production of bradykinin (ecallantide/Kalbitor®).71
- Bradykinin B2 receptor antagonists: prevent bradykinin from binding the B2 receptor, limits the symptoms associated with angioedema (icatibant acetate/Firazyr®) (Table 3).3,4,33,68-72
- Literature suggests treatment within 6 hours of onset improves outcomes.33,66,67,73
- Follow individualized treatment plan if available.3,4,66,67,74-76
- C1-INH concentrates are currently the first-line recommended therapies for bradykinin-mediated angioedema in those over 2 years of age; they can be expensive.1,3,4,14,38,67-70,74-76
- Ruconest®: only available human recombinant C1-INH; can be self-administered.68
- Plasma-derived C1-INHs: Berinert® and Cinryze®.3,4,67,69,70
- Patients with recurrent attacks may need higher doses of plasma-derived C1-INH (C1-INH concentrates may become less effective over time).1,3,4,14,38,74-76
- Ecallantide; kallikrein inhibitor used in those ≥ 12 years.71
- Icatibant: bradykinin antagonist; can be self-administered.72
- May also use these for patients with acquired angioedema.
- If concerned for ACEI-related angioedema, may administer epinephrine, antihistamines, and steroids. Usually not effective because underlying pathophysiology is bradykinin.3,14,66,77,78
- C1-INH replacement, ecallantide, and icatibant have been evaluated in literature for ACEI-related angioedema. Case reports demonstrate a possible benefit with C1-INH therapy.66,79,80 RCT with 30 patients with ACEI-related angioedema found no benefit with C1-INH therapy.81
- Icatibant can improve symptoms; no studies demonstrate reduction in ICU admissions or intubation.82
- TXA is another option, especially for ACEI induced angioedema.3,14,38,79,83,84
- Inhibits conversion of plasminogen to plasmin.
- Several retrospective studies suggest TXA may reduce symptoms with no severe adverse events reported.14,38,84-89
- Dose: 1 g IV over 2-10 minutes, followed by a second dose if necessary.90
- TXA is cheap, safe, and universally available.
- FFP is another proposed treatment.
- FFP contains angiotensin-converting enzyme (degrades bradykinin and C1-INH). 1,3,4,14,38,67,74-76
- Retrospective studies suggest benefit with FFP if other therapies are not available; no high-quality RCTs show benefit..79,91-95
- Potential problem: FFP contains varying levels of C1-INH and substrates of the kallikrein system, which may worsen the angioedema79,91-95 However, no case reports suggest an exacerbation of angioedema with FFP.
- If no access to other medications, or attempted TXA and there’s no improvement, consider FFP.
- Dose: 15 mg/kg IV or 2 units.
- Medication summary: many limitations with the individual studies.
- While there might be an improvement in symptoms and edema with medications, individual studies have low sample sizes and bias and heterogeneity in patient selection, comparators, medication dosing, study design, and outcomes.1,3,4,6,14,67,79,96-98
- Medications have a delayed onset of action and variable efficacy; focus on the airway.
- If histamine-mediated or unclear, treat as anaphylaxis with epinephrine.
- If known bradykinin-mediated, administer C1-INH replacement as soon as possible if available.
- TXA is worth attempting if limited access to other medications.
What should we consider for disposition?
- If airway involved, admit patient to ICU.
- Disposition can be more difficult for other patients; several studies have tried to predict airway compromise.42,56
- Ishoo staging system was derived from a retrospective study of 80 patients with 93 episodes of angioedema; categorizes severity based on the location of angioedema (Table 4).56
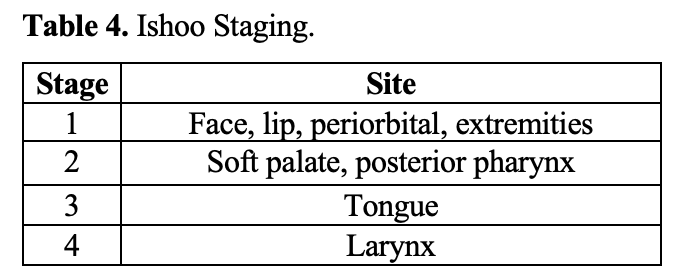
- 2021 ED retrospective chart review with 320 patients found patients with stage 4 findings required airway intervention in 67% of cases, but 16% of stage 3 and 8.6% of stage 2 patients needed airway intervetnion.64
- Issues with the score: limited by the need to directly visualize laryngeal structures.
- If using the score, patients with stage 1 may be discharged with follow-up after observation for several hours; stage 2 or higher should be admitted.11,60,64,74
- 2025 retrospective study with 94 patients found throat symptoms or throat/neck edema including difficulty speaking were associated with admission.42
- Observe patients with angioedema for several hours to monitor progression.14 Any worsening of angioedema despite treatments warrants admission.
- If patient appropriate for discharge, consider referring the patient to allergy/immunology specialist (especially recurrent angioedema).1,3,6,66,67,99-101
- May diagnose the underlying etiology, educate the patient on triggers, prescribe prophylactic medications.
- Must remove any triggers and discontinue medications that may be a causative agent (ACEIs, NSAIDs, and aspirin).1,3-7,10-12,14,66,74
- If on an ACEI, list it as an allergy; switch the patient to another agent.1,3,14,42,102-105
- Incidence of angioedema with an ARB approximates 0.11% (no different than placebo). While an ARB is likely safe in those with ACEI-induced angioedema, there may be a higher baseline risk of ARB angioedema in these patients.104,105
- If improve withtherapy for anaphylaxis, discharge with an epinephrine autoinjector; prior to discharge, educate on how to use it and potential triggers. If unsure of underlying trigger, follow up with allergy/immunology.3,66,67,101
Summary:
- Angioedema is non-dependent, non-pitting edema that can occur at a variety of sites including the external face, lips, and oropharyngeal structures.
- There are histamine-mediated and bradykinin-mediated forms.
- Initial evaluation and management has to focus on the airway.
- If concerned but you have time, perform flexible endoscopy. If this is not available, go with VL but prep for cricothyrotomy.
- If don’t know the etiology or concerned for histamine-mediated angioedema, treat with epinephrine, antihistamines, and steroids.
- For bradykinin mediated forms, first line treatment is C1 esterase inhibitor replacements. There are also kallikrein inhibitor, and bradykinin receptor antagonists.
- TXA and FFP may be effective in bradykinin mediated forms.
- Disposition depends on patient’s airway status and the involved sites.
References:
- Moellman JJ, Bernstein JA, Lindsell C, et al.; American College of Allergy Asthma & Immunology (ACAAI); Society for Academic Emergency Medicine (SAEM). A consensus parameter for the evaluation and management of angioedema in the emergency department. Acad Emerg Med. 2014;21:469–84.
- Bork K. An evidence based therapeutic approach to hereditary and acquired angioedema. Curr Opin Allergy Clin Immunol. 2014;14(4):354-362.
- Long BJ, Koyfman A, Gottlieb M. Evaluation and Management of Angioedema in the Emergency Department. West J Emerg Med. 2019 Jul;20(4):587-600.
- Lacuesta G, Betschel SD, Tsai E, Kim H. Angioedema. Allergy Asthma Clin Immunol. 2024 Dec 9;20(Suppl 3):65.
- Bork K. Angioedema. Immunol Allergy Clin North Am. 2014;34(1):23-31.
- Wilkerson RG. Angioedema in the emergency department: an evidence-based review. Emerg Med Pract. 2012;14(11): 1-24.
- Kim SJ, Brooks JC, Sheikh J, Kaplan MS, Goldberg BJ. Angioedema deaths in the United States, 1979-2010. Ann Allergy Asthma Immunol. 2014;113(6):630-634.
- Bernstein JA, Moellman J. Emerging concepts in the diagnosis and treatment of patients with undifferentiated angioedema. Int J Emerg Med. 2012;5:39.
- Bernstein JA, Cremonsei P, Hoffman TK, et al. Angioedema in the emergency department: a practical guide to differential diagnosis and management. Int J Emerg Med.2017 Dec;10(1):15.
- Bernstein JA. Update on angioedema: evaluation, diagnosis, and treatment. Allergy Asthma Proc. 2011;32:408–12.
- Moellman JJ, Bernstein JA. Diagnosis and management of hereditary angioedema: an emergency medicine perspective. J Emerg Med. 2012 Aug;43(2):391-400.
- Clinical Practice Guideline: Initial Evaluation and Management of Patients Presenting with Acute Urticaria or Angioedema. 2006. Available at https://www.aaem.org/statements/clinical-practice-guideline-initial-evaluation-and-management-of-patients-presenting-with-acute-urticaria-or-angioedema/. Accessed 12 March 2025.
- Bluestein HM, Hoover TA, Banerji AS, Camargo CA Jr, Reshef A, Herscu P. Angiotensin-converting enzyme inhibitor-induced angioedema in a community hospital emergency department. Ann Allergy Asthma Immunol. 2009 Dec;103(6):502-7.
- Craig T, Aygören-Pürsün E, Bork K, Bowen T, Boysen H, Farkas H, et al. WAO Guideline for the Management of Hereditary Angioedema. World Allergy Organ J. 2012 Dec;5(12):182-99.
- Carrillo-Martin I, Gonzalez-Estrada A, Funni SA, Sandefur BJ, Jeffery MM, Campbell RL. Angioedema-related emergency department visits in the United States: Epidemiology and time trends, 2006–2015. J Allergy Clin Immunol Pract. 2020; S2213–2198(20): 30351–2.
- Jolles S, Williams P, Carne E, et al. A UK national audit of hereditary and acquired angioedema. Clin Exp Immunol. 2014; 175(1): 59–67.
- Gaeta TJ, Clark S, Pelletier AJ, Camargo CA Jr. National study of US emergency department visits for acute allergic reactions, 1993 to 2004. Ann Allergy Asthma Immunol 2007;98:360–5.
- Zilberberg MD, Jacobsen T, Tillotson G. The burden of hospitalizations and emergency department visits with hereditary angioedema and angioedema in the United States, 2007. Allergy Asthma Proc. 2010;31:511–9.
- Lin RY, Anderson AS, Shah SN, Nurruzzaman F. Increasing anaphylaxis hospitalizations in the first 2 decades of life: New York State, 1990-2006. Ann Allergy Asthma Immunol. 2008;101:387–93.
- Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J Med. 2008;359(10):1027-1036.
- Bas M, Adams V, Suvorava T, et al. Nonallergic angioedema: role of bradykinin. 2007;62:842–56.
- Blanch A, Roche O, Urrutia I, et al. First case of homozygous C1 inhibitor deficiency. J Allergy Clin Immunol.2006;118(6):1330-1335.
- Bork K, Meng G, Staubach P, Hardt J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. 2006;119:267–74.
- Nordenfelt P, Nilsson M, Björkander J, Mallbris L, Lindfors A, Wahlgren CF. Hereditary Angioedema in Swedish Adults: Report From the National Cohort. Acta Derm Venereol. 2016 May;96(4):540-5.
- Schöffl C, Wiednig M, Koch L, Blagojevic D, Duschet P, Hawranek T, Kinaciyan T, Öllinger A, Aberer W. Hereditary angioedema in Austria: prevalence and regional peculiarities. J Dtsch Dermatol Ges. 2019 Apr;17(4):416-423.
- Troelnikov A, Milburn K, Hissaria P, Thao Adriana Le T, Smith W. Hereditary angioedema prevalence and satisfaction with prophylaxis in South Australia. World Allergy Organ 2024 Jun 18;17(7):100918.
- Banerji A, Blumenthal KG, Lai KH, Zhou L. Epidemiology of ACE Inhibitor Angioedema Utilizing a Large Electronic Health Record. J Allergy Clin Immunol Pract. 2017 May-Jun;5(3):744-749.
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26:725–737.
- Landry L, Witten T, Anwar AI, Jackson CN, Talbot NC, Ahmadzadeh S, et al. Angiotensin-Converting Enzyme Inhibitors and Other Medications Associated With Angioedema. 2023 Nov 23;15(11):e49306.
- Guan X, Sheng Y, Liu S, He M, Chen T, Zhi Y. Epidemiology, economic, and humanistic burden of hereditary angioedema: a systematic review. Orphanet J Rare Dis. 2024 Jul 8;19(1):256.
- Sinnathamby ES, Issa PP, Roberts L, Norwood H, Malone K, Vemulapalli H, et al. Hereditary Angioedema: Diagnosis, Clinical Implications, and Pathophysiology. Adv Ther. 2023 Mar;40(3):814-827.
- Henao MP, Kraschnewski JL, Kelbel T, Craig TJ. Diagnosis and screening of patients with hereditary angioedema in primary care. Ther Clin Risk Manag. 2016;12:701.
- Bernstein JA. Severity of hereditary angioedema, prevalence, and diagnostic considerations. Am J Manag Care. 2018;24(14 Suppl):S292–8.
- Minafra FG, Gonçalves TR, Alves TM, Pinto JA. The Mortality from Hereditary Angioedema Worldwide: a Review of the Real-World Data Literature. Clin Rev Allergy Immunol. 2022 Feb;62(1):232-239.
- Christiansen SC, Wilmot J, Castaldo AJ, Zuraw BL. The US Hereditary Angioedema Association Scientific Registry: hereditary angioedema demographics, disease severity, and comorbidities. Ann Allergy Asthma Immunol. 2023 Dec;131(6):766-774.e8.
- Jayasinghe M, Caldera D, Prathiraja O, Jena R, Coffie-Pierre JA, Agyei J, et al. A Comprehensive Review of Bradykinin-Induced Angioedema Versus Histamine-Induced Angioedema in the Emergency Department. Cureus.2022 Nov 30;14(11):e32075.
- Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol. 2012;130:692–7.
- Bork K. Recurrent angioedema and the threat of asphyxiation. Dtsch Arztebl Int. 2010;107:408–14.
- Cousins KL, Ogundipe F, Ahmad B, Suryakumar L, Mehari A. Hereditary Angioedema Exacerbation Precipitated by Heroin Use. J Allergy Clin Immunol. 2019 Feb;143(2):AB48.
- Briggs B, Cline D, Husain I. Disposition of emergency department patients presenting with angiotensin-converting enzyme inhibitor-induced angioedema. Int J Emerg Med. 2025 Jan 10;18(1):11.
- Kieu MC, Bangiyev JN, Thottam PJ, Levy PD. Predictors of Airway Intervention in Angiotensin-Converting Enzyme Inhibitor-Induced Angioedema. Otolaryngol Head Neck Surg. 2015 Oct;153(4):544-50.
- Mudd PA, Hooker EA, Stolz U, Hart KW, Bernstein JA, Moellman JJ. Emergency department evaluation of patients with angiotensin converting enzyme inhibitor associated angioedema. Am J Emerg Med. 2020 Dec;38(12):2596-2601.
- Gill P, Betschel SD. The Clinical Evaluation of Angioedema. Immunol Allergy Clin N Am. 2017;37:449–466.
- Grigoriadou S, Longhurst HJ. Clinical immunology review series: an approach to the patient with angio-oedema. Clin Exp Immunol. 2008;155(3):367–77.
- Vazquez Nava F, Almeida Arvizu VM, Sanchez Nuncio HR, et al. [Prevalence and potential triggering factors of chronic urticaria and angioedema in an urban area of northeastern Mexico] (article in Spanish). Rev Alerg Me.x2004;51:181–8.
- Pigman EC, Scott JL. Angioedema in the emergency department: the impact of angiotensin-converting enzyme inhibitors. Am J Emerg Med. 1993;11:350–4.
- Saxena S, Gierl B, Eibling DE. Supraglottic swelling may not correlate with tongue swelling in angiotensin converting enzyme inhibitor-induced angioedema. 2010;120:62–4.
- Sandefur BJ, Driver BE, Long B. Managing Awake Intubation. Ann Emerg Med. 2025 Jan;85(1):21-30.
- Ishigami K, Averill SL, Pollard JH, McDonald JM, Sato Y. Radiologic manifestations of angioedema. Insights Imaging. 2014 Jun;5(3):365-74.
- Schick M, Grether-Jones K. Point-of-Care Sonographic Findings in Acute Upper Airway Edema. West J Emerg Med. 2016 Nov;17(6):822-826.
- Lin DH, Meyers B, Nisar S, Heinz ER. Role of Submandibular Ultrasound in Airway Management of a Patient With Angioedema. Cureus. 2022 Mar 3;14(3):e22823.
- Tay ET, Ngai KM, Tsung JW, Sanders JE. Point-of-Care Ultrasound on Management of Cellulitis Versus Local Angioedema in the Pediatric Emergency Department. Pediatr Emerg Care. 2022 Feb 1;38(2):e674-e677.
- Ishoo E, Shah UK, Grillone GA, et al. Predicting airway risk in angioedema: staging system based on presentation. Otolaryngol Head Neck Surg. 1999;121:263–8.
- Agah R, Bandi V, Guntupalli KK. Angioedema: the role of ACE inhibitors and factors associated with poor clinical outcome. Intensive Care Med. 1997;23:793–6.
- Al-Khudari S, Loochtan MJ, Peterson E, Yaremchuk KL. Management of angiotensin-converting enzyme inhibitor-induced angioedema. 2011; 121:2327–34.
- Gannon TH, Eby TL. Angioedema from angiotensin converting enzyme inhibitors: a cause of upper airway obstruction. 1990;100:1156–60.
- McCormick M, Folbe AJ, Lin HS, et al. Site involvement as a predictor of airway intervention in angioedema. 2011;121:262–6.
- Stojiljkovic L. Renin-angiotensin system inhibitors and angioedema: anesthetic implications. Curr Opin Anaesthesiol.2012;25:356–62.
- Stone CA Jr, Choi JJ. Effect of use of inhaled epinephrine on intramuscular epinephrine use in patients with idiopathic anaphylaxis and angioedema. Ann Allergy Asthma Immunol. 2016 Feb;116(2):170-1.
- Jaiganesh T, Wiese M, Hollingsworth J, et al. Acute angioedema: recognition and management in the emergency department. Eur J Emerg Med. 2013;20:10–7.
- Dass C, Mahaffa M, Dang E, Campbell R, Ballas Z, Lee S. Evaluation of staging criteria for disposition and airway intervention in emergency department angioedema patients. Acute Med Surg. 2021 Oct 26;8(1):e704.
- Long B, Gottlieb M. Emergency medicine updates: Anaphylaxis. Am J Emerg Med. 2021 Nov;49:35-39.
- Zuraw BL, Bernstein JA, Lang DM, Craig T, Dreyfus D, Hsieh F, et al; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. A focused parameter update: hereditary angioedema, acquired C1 inhibitor deficiency, and angiotensin-converting enzyme inhibitor-associated angioedema. J Allergy Clin Immunol. 2013 Jun;131(6):1491-3.
- Riha HM, Summers BB, Rivera JV. Novel therapies for angiotensin-converting enzyme inhibitor-induced angioedema: a systematic review of current evidence. J Emerg Med. 2017;53(5):662-79.
- 2022. Available at https://www.ruconest.com/wp-content/uploads/Ruconest_PI_Apr2020.pdf. Accessed April 28, 2025.
- 2022. Available at https://www.berinert.com/professional. Accessed April 28, 2025.
- 2024. Available at https://pi.shirecontent.com/PI/PDFs/Cinryze_USA_ENG.pdf. Accessed April 28, 2025.
- 2025. Available at https://www.kalbitor.com/hcp/how-kalbitor-works. Accessed April 28, 2025.
- 2025. Availalbe at https://www.firazyr.com/hcp. Accessed April 28, 2025.
- Murphy E, Donahue C, Omert L, Persons S, Tyma TJ, Chiao J, et al. Training patients for self-administration of a new subcutaneous C1-inhibitor concentrate for hereditary angioedema. Nurs Open. 2019;6(1):126–35.
- Bowen T, Cicardi M, Farkas H, et al. 2010 International consensus algorithm for the diagnosis, therapy and management of hereditary angioedema. Allergy Asthma Clin Immunol. 2010;6:24.
- Wahn V, Aberer W, Eberl W, et al. Hereditary angioedema (HAE) in children and adolescents–a consensus on therapeutic strategies. Eur J Pediatr.. 2012;171:1339–48.
- Epstein TG, Bernstein JA. Current and emerging management options for hereditary angioedema in the US. 2008;68:2561–73.
- Lang DM, Aberer W, Bernstein JA, Chng HH, Grumach AS, Hide M, et al. International consensus on hereditary and acquired angioedema. Ann Allergy Asthma Immunol. 2012 Dec;109(6):395-402.
- Cicardi M, Aberer W, Banerji A, Bas M, Bernstein JA, Bork K, et al; HAWK under the patronage of EAACI (European Academy of Allergy and Clinical Immunology). Classification, diagnosis, and approach to treatment for angioedema: consensus report from the Hereditary Angioedema International Working Group. Allergy. 2014 May;69(5):602-16.
- van den Elzen M, Go MFCL, Knulst AC, Blankestijn MA, van Os-Medendorp H, Otten HG. Efficacy of Treatment of Non-hereditary Angioedema. Clin Rev Allergy Immunol. 2018 Jun;54(3):412-431.
- Ibarra F Jr, Cruz M. C1 esterase inhibitor use in the management of lisinopril-induced angioedema: A case series. J Am Pharm Assoc (2003). 2020 Nov-Dec;60(6):e361-e364.
- Strassen U, Bas M, Wirth M, Wirth M, Gröger M, Stelter K, et al. Efficacy of human C1 esterase inhibitor concentrate for treatment of ACE-inhibitor induced angioedema. Am J Emerg Med. 2023 Feb;64:121-128.
- Baş M, Greve J, Stelter K, Havel M, Strassen U, Rotter N, et al. A randomized trial of icatibant in ACE-inhibitor-induced angioedema. N Engl J Med. 2015 Jan 29;372(5):418-25.
- De Knop KJ, Hagendorens MM, Stevens WJ, De Clerck LS, Ebo DG. Angioedema beyond histamine: an educational case series. Acta Clin Belg. 2009 Nov-Dec;64(6):520-8.
- Beauchene C, Martins-Hericher J, Denis D, Martin L, Maillard H. Tranexamic acid as first-line emergency treatment for episodes of bradykinin-mediated angioedema induced by ACE inhibitors. Rev Med Interne. 2018; 39:772-6.
- Pathak GN, Truong TM, Chakraborty A, Rao B, Monteleone C. Tranexamic acid for angiotensin-converting enzyme inhibitor-induced angioedema. Clin Exp Emerg Med. 2024 Mar;11(1):94-99.
- Hasara S, Wilson K, Amatea J, Anderson J. Tranexamic acid for the emergency treatment of angiotensin-converting enzyme inhibitor-induced angioedema. Cureus. 2021; 13:e18116.
- Martinez Manzano JM, Lo KB, Patarroyo-Aponte G, Azmaiparashvili Z. The use of intravenous tranexamic acid for patients with angiotensin-converting enzyme inhibitor-induced angioedema: a case series. Ann Allergy Asthma Immunol. 2021; 126:725-6.
- Du-Thanh A, Raison-Peyron N, Drouet C, Guillot B. Efficacy of tranexamic acid in sporadic idiopathic bradykinin angioedema. 2010; 65:793-5.
- Lindauer KE, Lo BM, Weingart GS, Karpov MV, Gartman GH, Neubauer LE, Kaplan MC. Tranexamic acid for angiotensin converting enzyme inhibitor induced angioedema: A retrospective multicenter study. Am J Emerg Med. 2024 May;79:33-37.
- Caballero T, Baeza ML, Cabañas R, Campos A, Cimbollek S, Gómez-Traseira C, et al; Spanish Study Group on Bradykinin-Induced Angioedema; Grupo Español de Estudio del Angioedema mediado por Bradicinina. Consensus statement on the diagnosis, management, and treatment of angioedema mediated by bradykinin. Part I. Classification, epidemiology, pathophysiology, genetics, clinical symptoms, and diagnosis. J Investig Allergol Clin Immunol. 2011;21(5):333-47; quiz follow 347. Erratum in: J Investig Allergol Clin Immunol. 2012;22(2):3 p following 153.
- Hill BJ, Thomas SH, McCabe C. Fresh frozen plasma for acute exacerbations of hereditary angioedema. Am J Emerg Med. 2004 Nov;22(7):633.
- Hassen GW, Kalantari H, Parraga M, Chirurgi R, Meletiche C, Chan C, et al. Fresh frozen plasma for progressive and refractory angiotensin-converting enzyme inhibitor-induced angioedema. J Emerg Med. 2013 Apr;44(4):764-72.
- Pekdemir M, Ersel M, Aksay E, Yanturali S, Akturk A, Kiyan S. Effective treatment of hereditary angioedema with fresh frozen plasma in an emergency department. J Emerg Med. 2007 Aug;33(2):137-9.
- Prematta M, Gibbs JG, Pratt EL, Stoughton TR, Craig TJ. Fresh frozen plasma for the treatment of hereditary angioedema. Ann Allergy Asthma Immunol. 2007 Apr;98(4):383-8.
- Tang R, Chen S, Zhang HY. Fresh frozen plasma for the treatment of hereditary angioedema acute attacks. Chin Med Sci J. 2012 Jun;27(2):92-5.
- Wilkerson RG, Martinelli AN, Oliver WD. Treatment of Angioedema Induced by Angiotensin-Converting Enzyme Inhibitor. J Emerg Med. 2018;55(1):132-33.
- Sinert R, Levy P, Bernstein JA, et al. Randomized trial of icatibant for angiotensin-converting enzyme inhibitor-induced upper airway angioedema. J Allergy Clin Immunol Pract. 2017;5:1402–9.
- Straka BT, Ramirez CE, Byrd JB, et al. Effect of bradykinin receptor antagonism on ACE inhibitor-associated angioedema. J Allergy Clin Immunol. 2017;140:242–2482.
- Kreuz W, Rusicke E, Martinez-Saguer I, et al. Home therapy with intravenous human C1-inhibitor in children and adolescents with hereditary angioedema. 2012;52:100–7.
- Cicardi M, Bork K, Caballero T, et al. Evidence based recommendations for the therapeutic management of angioedema owing to hereditary C1 inhibitor deficiency: consensus report of an International Working Group. 2012;67:147–57.
- Busse PJ. Angioedema: differential diagnosis and treatment. Allergy Asthma Proc. 2011;32(Suppl 1): S3–11.
- Cicardi M, Zingale LC, Bergamaschini L, Agostoni A. Angioedema associated with angiotensin-converting enzyme inhibitor use: outcome after switching to a different treatment. Arch Intern Med. 2004;164:910–3.
- Haymore BR, Yoon J, Mikita CP, et al. Risk of angioedema with angiotensin receptor blockers in patients with prior angioedema associated with angiotensin-converting enzyme inhibitors: a meta-analysis. Ann Allergy Asthma Immunol.2008;101:495–9.





