Originally published at R.E.B.E.L. EM on April 9, 2020. Reposted with permission. Follow Salim R. Rezaie at @srrezaie
The Novel Coronavirus 2019, was first reported on in Wuhan, China in late December 2019. The outbreak was declared a public health emergency of international concern in January 2020 and on March 11th, 2020, the outbreak was declared a global pandemic. The spread of this virus is now global with lots of media attention. The virus has been named SARS-CoV-2 and the disease it causes has become known as coronavirus disease 2019 (COVID-19). This new outbreak has been producing lots of hysteria and false truths being spread, however the data surrounding the biology, epidemiology, and clinical characteristics are growing daily, making this a moving target. This post will serve as a summary of thrombosis and hemoglobin in regard to COVID-19.
To go back to the main post, click on the image below…
Venothromboembolism (VTE):
- COVID-19 is most likely causing a hypercoaguable state, however the prevalence of acute VTE is still an evolving area
- D-dimer is a non-specific acute phase reactant
- Limited data suggest pulmonary microvascular thrombosis may play a role in progressive respiratory failure
- Early data suggest high rates of VTE without pharmacological prophylaxis
- Most evidence is limited due to retrospective, small trials
- Retrospective study done at single center with 25 COVID-19 patients who had CTPA [1]

-
- No significant difference was found between acute pulmonary embolism (APE) positive and acute pulmonary embolism (APE) negative groups for all laboratory data except for D-dimer
- 20 pts treated with LMWH 0.6mg/kg per 12hrs
- Regardless of findings of APE on CTPA, all pts had decrease in D-dimer levels
- 3 pts had follow-up CTPA after LMWH initiation and all had smaller APE lesions compared to first CTPA
- All filling defects were found in small branches
- Only one patient had lower extremity US in this study and therefore rate of DVT not known
- 3 patients with COVID-19 evaluated for anti-phospholipid antibody [2]
- Anticardiolipin IgA antibodies & anti–β2-glycoprotein I IgA and IgG antibodies were detected
- Lupus anticoagulant was not detected in any of the patients
- Retrospective review from two hospitals in China [4]
- 191 patients with COVID-19
- D-dimer > 1.0ug/mL had higher mortality vs patients with lower D-dimer values
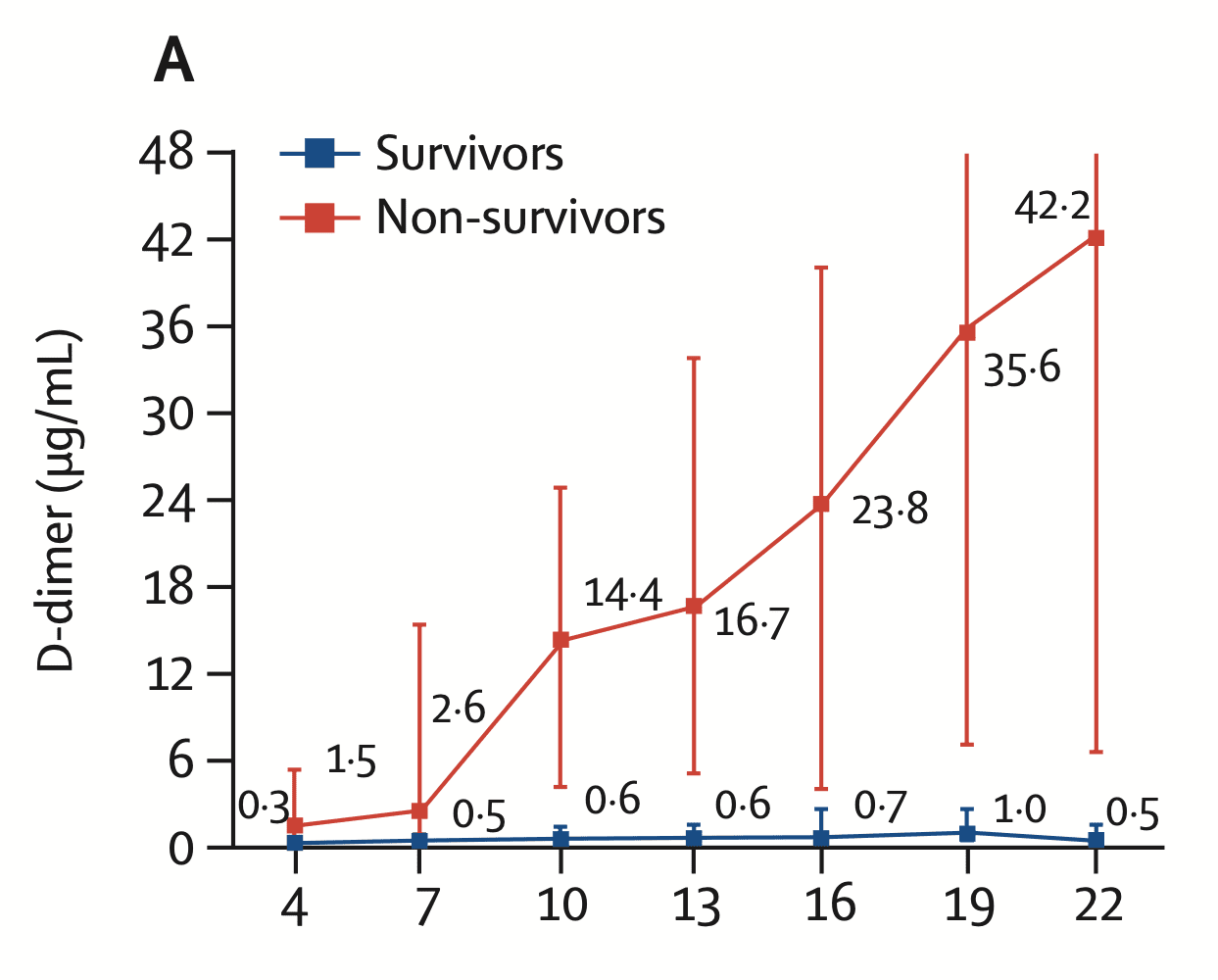
Image from [4]
- 81 ICU patients with COVID-19 [6]
- Wanted to determine the incidence of VTE in pts with severe COVID-19 PNA
- 81 patients with severe COVID-19 PNA admitted to ICU in China
- Coagulation parameters and lower extremity US data was retrospectively collected
- 20/81 (25%) had lower extremity DVT without VTE prophylaxis
- 8/20 (40%) of pts with lower extremity DVT died
- Using a D-dimer cutoff >1.5ug/mL to predict VTE
- Sensitivity = 85%
- Specificity = 88.5%
- NPV = 94.7%
- PPV = 70.8%
- 184 patients in 3 Dutch hospitals [8]
- Evaluated incidence of the composite outcome of symptomatic acute PE, DVT, ischemic stroke, MI, or systemic arterial embolism of COVID-19 patients admitted to the ICU
- All patients received at least standard doses of thromboprophylaxis
- Cumulative incidence of thrombosis = 31%
- PE most common thrombotic complication = 25pts (81%)
- Prophylaxis Options:
- LMWH nadroparin 2850IU/d
- >100kg = LMWH nadroparin 5700IU/d
- Independent predictors of thrombotic complications = Prolonged aPTT >5sec & PT >3sec (aHR 4.1; 95% CI 1.9 – 9.1)
- Case series of 4 autopsies of COVID-19 infected pts in New Orleans [9]
- All cases had sudden respiratory decompensation prior to arrival to ED
- Notable lab findings were elevated ferritin, fibrinogen, & PT
- D-dimers drawn near the time of death in 2 pts were elevated: 1200 – 2900ng/mL
- Gross Pathology Findings:
- Pulmonary arteries at the hilum were free of thromboemboli
- Peripheral parenchyma had regions of dark-colored hemorrhage with focal demarcation
- In some cases, small, firm thrombi were present in sections of peripheral parenchyma
- Microscopic Findings:
- Small vessels contained platelets and small thrombi
- Scattered areas of diffuse alveolar damage
- Small vessel thrombus formation was seen in lung periphery in many cases
- Notable Finding: Lack of significant secondary infection in all cases
- Pathological Evidence of Pulmonary Thrombotic Phenomena in Severe COVID-19 [13]
- A group out of Sao Paulo, Brazil performed minimally invasive autopsies in fatal cases of COVID-19 in order to characterize the pathology and pathogenesis
- Used an ultrasound-based minimally invasive autopsy (MIA-US) that samples tissues from several organs and minimizes risks of the autopsy procedure
- This is a preliminary autopsy set of results looking for insights into the relationship between COVID-19 and DIC
- Authors did not have access to large vessels and cannot confirm or exclude PEs
- 10 total fatal cases were examined
- Histology:
- Intense epithelial viral cytopathic effects involving alveolar and small airway epithelium
- Variable number of small fibrinous thrombi in small pulmonary arterioles in areas of damaged and preserved lung parenchyma in 8/10 cases
- Endothelial tumefaction (swelling) and large numbers of pulmonary megakaryocytes in pulmonary capillaries (Indicate activation of coagulation cascade)
- Few and small foci of alveolar hemorrhage and pulmonary infarctions
- Signs of secondary bacterial pneumonia seen in 6/10 cases
- Bottom Line: this report supports the concept of hypercoagulative status, showing high frequency of pulmonary microthrombosis
- Histology:
- A group out of Sao Paulo, Brazil performed minimally invasive autopsies in fatal cases of COVID-19 in order to characterize the pathology and pathogenesis

- Prevalence of VTE in consecutively admitted patients to ICU in Italy [14]
- 54 pts total
- All pts treated with prophylactic LMWH adjusted to body weight since admission
- 22.2% of patients admitted to ICU had VTE
- 8 DVTs
- 1 Tricuspid valve thrombosis
- 2 Sub-segmental PEs
- 1 Cardiac Arrest (PEA with RV Dilatation
- Patients with ARDS due to COVID-19 from 4 ICUs (2 centers) in France [15]
- Used a historical prospective cohort of “non-COVID-19 ARDS” patients (PMID: 27066082)
- All patients on prophylactic or therapeutic anticoagulation
- Primary Outcome: Comparison of the occurrence of thrombotic events (DVTs, PEs, MIs, mesenteric ischemia, lower limb ischemia, CVA) between patients with COVID-19 ARDS and historical patients with non-COVID-19 ARDS
- 150 COVID-19 patients
- Relevant thrombotic complications: 64/150 (42.7%)
- Mainly PEs = 25/150 (16.7%)
- Troncular = 9
- Lobar = 8
- Segmental = 5
- Subsegmental = 3
- Receiving Continuous Renal Replacement Therapy who Developed Circuit Clotting = 28/29 (96.6%)
- No MIs during ICU stay in this study
- Only 4 patients (2.7%) presented with hemorrhagic complications
- 2 with recent head trauma before ICU admission
- Elevated D-Dimer & Fibrinogen Levels: >95% of patients
- Positive Lupus Circulating Anticoagulant: 50/57 (87.7%)
- COVID-19 ARDS vs Historical Non-COVID-19 ARDS [16]
- Groups similar at baseline

-
-
- DIC:
- No COVID-19 patients were diagnosed with DIC using ISTH “overt” score
- 6 COVID-19 patients were diagnosed with DIC using JAAM-DIC score
- 22 COVID-19 patients were diagnosed with DIC using SIC score
- Limitations:
- No systematic standardized assessment of thromboembolic events, therefore thromboembolic events may be under-estimated in this study
- Prophylactic dosing was 4000 UI/day for low molecular weight heparin or if contra-indicated, unfractioned heparin at 5-8 U/kg/hour. LMWH may be under dosed in patients with higher BMIs
- Bottom Line: Despite anticoagulation, a high number of patients with ARDS secondary to COVID-19 in the ICU developed life-threatening thrombotic complications. Higher anticoagulation targets should be considered by following anti-Xa levels in critically ill patients with COVID-19 ARDS
- DIC:
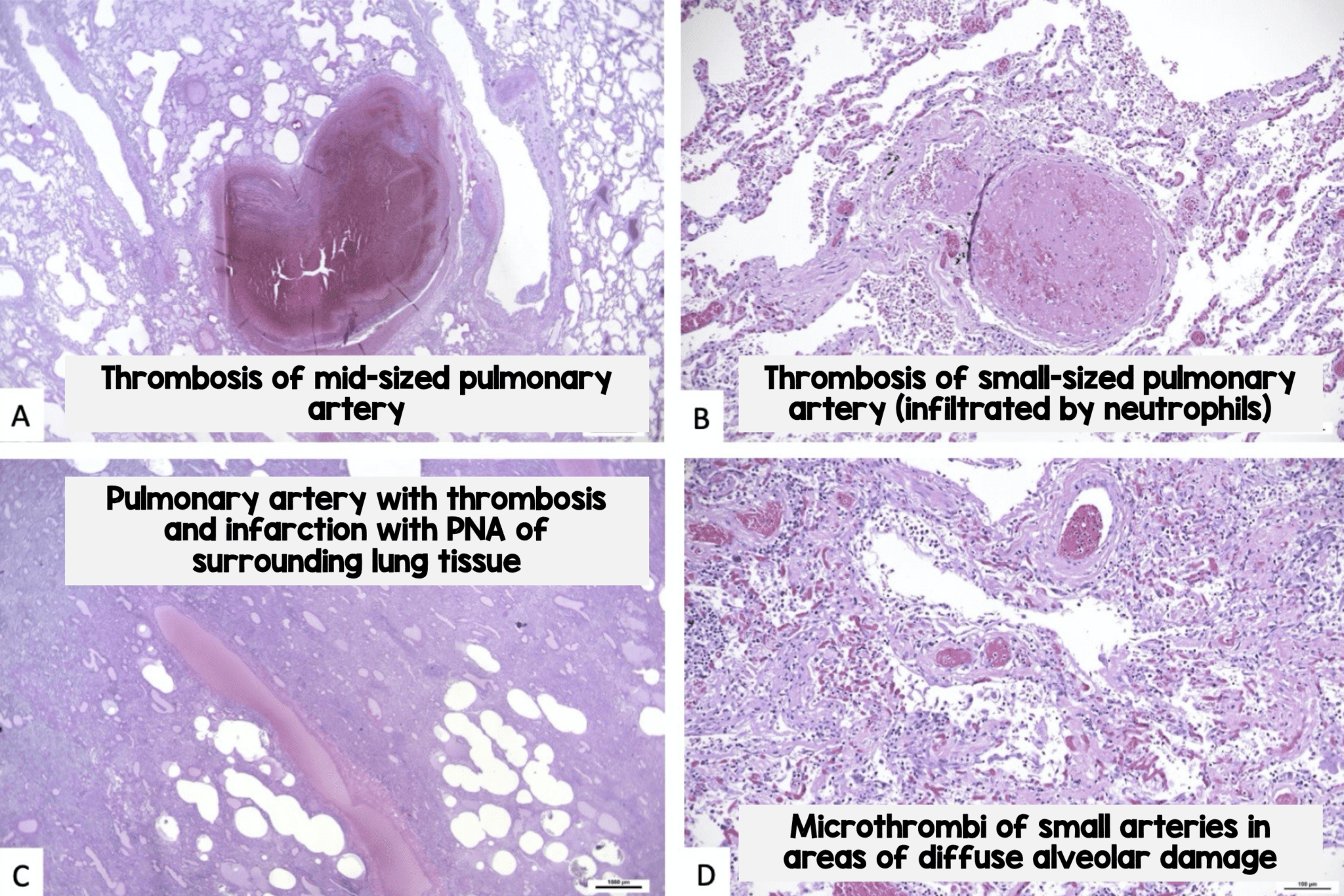
- Prospective, single center autopsy study of 11 deceased patients with COVID-19 [18]
- 10 of 11 patients received prophylactic anticoagulant therapy
- VTE was not clinically suspected antemortem in any of the patients
- Both lungs showed various stages of diffuse alveolar damage (DAD)
- edema
- hyaline membranes
- proliferation of pneumocystis and fibroblasts
- Thrombosis of small and mid-sized pulmonary arteries was found in various degrees in all 11 patients
- associated with infarction in 8 patients
- associated with bronchopneumonia in 6 patients
-
-
-
- Bottom Line: COVID-19 predominantly involved the lungs, caused DAD, and led to acute respiratory insufficiency. Death may have been the result of thrombosis observed in segmental and sub segmental pulmonary arteries despite prophylactic anticoagulation
-
VTE Prophylaxis
- No need to CT all patients who are getting admitted because they should all be on some form of anticoagulation whether you’ve definitively diagnosed PE or not
- Most patients will have microthrombi
- Patients may also have arterial thrombosis as well
- Retrospective analysis of 449 consecutive patients with severe COVID-19 [5]
- 94/99 patients received LMWH (40 – 60mg/day) for 7d or longer
- D-dimer and PT were correlated with 28d mortality
- In pts with Sepsis Induced Coagulopathy (SIC) score ≥4 mortality was significantly reduced with anticoagulation (40.0% vs 64.2%, P = 0.029)
- In pts with D-dimer >3.0ug/mL (6x upper limit of normal) anticoagulation resulted in 20% reduction in mortality (32.8% vs 52.4%, p = 0.017)
- American Society of Hematology (Link is HERE) recommends all hospitalized patients with COVID-19 should receive thromboprophylaxis with LMWH or fondaparinux (suggested over unfractionated heparin to reduce contact) unless the patient is judged to be at increased risk of bleeding. In patients with a history of heparin-induced thrombocytopenia (HIT) use fondaparinux
Treatment Dose Anticoagulation
- Clinical Question: What is the effect of treatment dose systemic anticoagulation vs no anticoagulation on mortality in patients admitted with COVID-19? [16]
- What They Did:
- Retrospective observational trial of patients admitted with confirmed COVID-19 within the Mount Sinai Health System in New York City
- Treatment dose systemic anticoagulation (oral, subcutaneous, or IV forms) vs no anticoagulation
- Results:
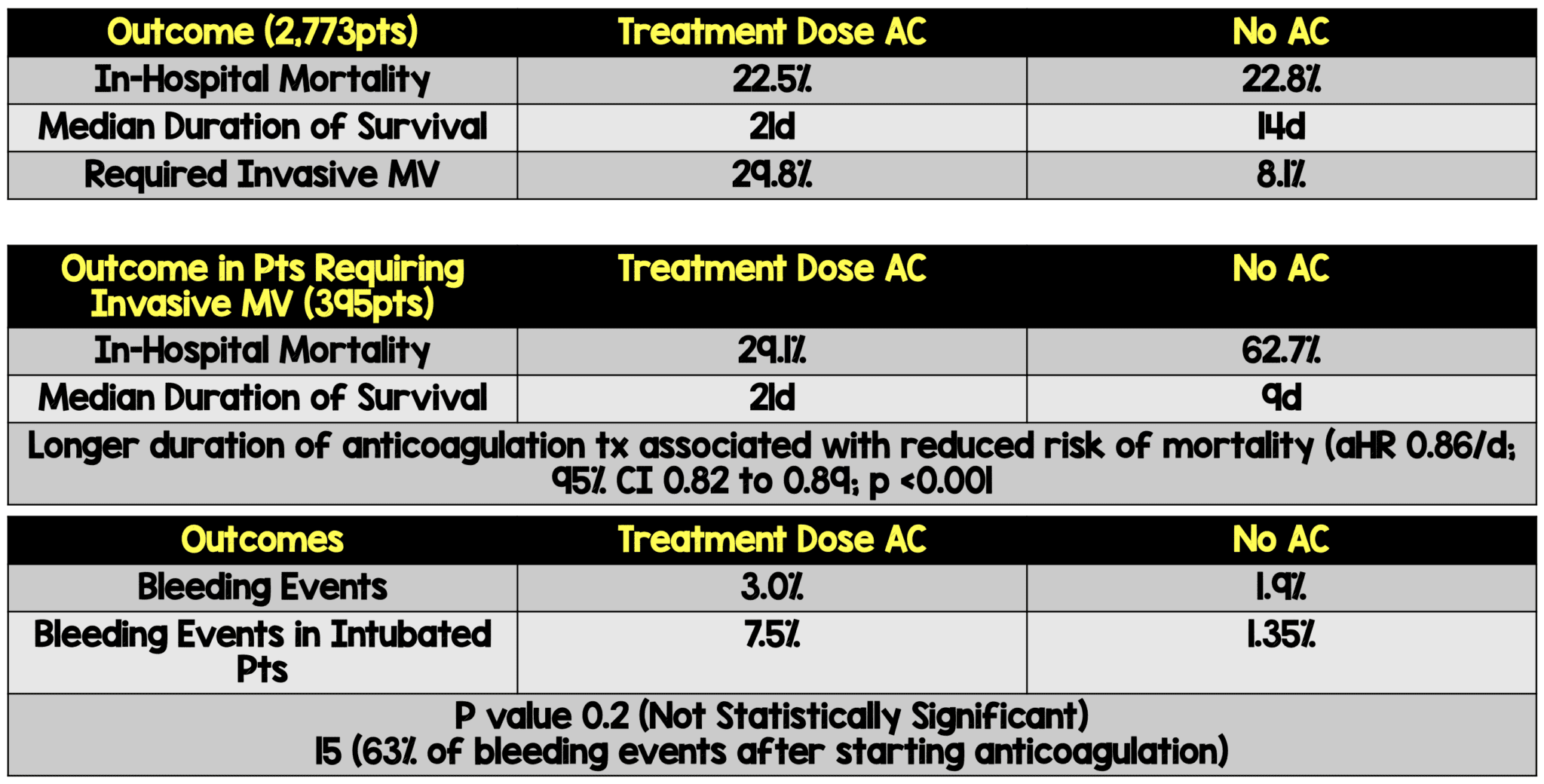
- 2,773 hospitalized patients hospitalized with COVID-19
- 786 (28%) received systemic anticoagulation during their hospital course
- Median hospitalization duration was 5 days (Range: 3 to 8 days)
- Median time from admission to anticoagulation initiation was 2 days (Range 0 to 5 days)
- Median duration of anticoagulation treatment was 3 days (Range 2 to 7 days)
- 2,773 hospitalized patients hospitalized with COVID-19
- Lots of Limitations:
- Observational study can only give association not causation
- Unclear confounders
- Unknown indication for anticoagulation
- Lack of metrics to further classify illness severity in mechanically ventilated subgroup
- Comparator no anticoagulation, not prophylactic dose anticoagulation (Standard care)
- Indication bias: Association between the exposure and the outcome confounded by the indication
- Clinical Take Home Point: Therapeutic anticoagulation was associated with improved in-hospital mortality in patients requiring mechanical ventilation in this trial, however due to the many limitations of the study, hard to make robust conclusions…The one positive thing in this trial is the rate of bleeding was low.
ISTH Interim Guidance on Recognition and Management of Coagulopathy in COVID-19 [7]
- One of the most significant poor prognostic features of severely ill COVID-19 patients is the development of coagulopathy
- They developed a guidance document that provides a risk stratification at admission for COVID-19 patients as well as the management of coagulopathy which may develop
- Patients with an elevated d-dimer (i.e. arbitrarily defined as 3 – 4 fold increase) will need admission to the hospital
- Monitoring for decreased fibrinogen levels later in the disease process (i.e. days 10 – 14) may be helpful in determining if a patient has developed disseminated intravascular coagulation (DIC)
- LMWH should be considered in ALL patients (including non-critically ill) who require hospital admission for COVID-19 infection, in the absence of any contraindications:
- Active bleeding
- Platelet count <25×109/L
- Monitoring advised in severe renal impairment
- Abnormal PT or aPTT is not a contraindication
- LMWH may have anti-inflammatory properties which can be an additional benefit in COVID-19 infection
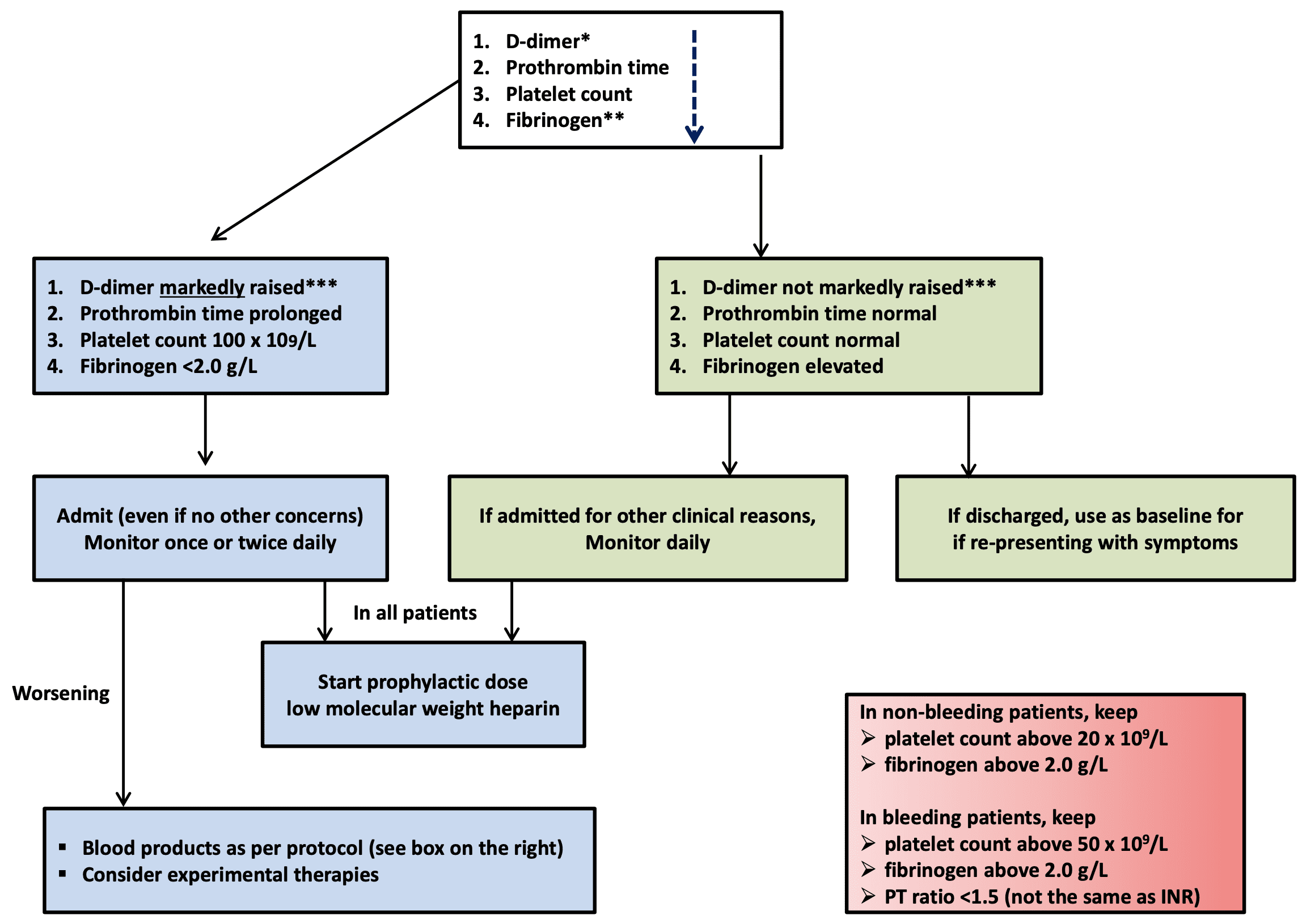
Algorithm for the Management of Coagulopathy in COVID-19 Based on Simple Laboratory Markers
* The list of markers is given in the decreasing order of importance.
** Performing fibrinogen assays may not be feasible in many laboratories but monitoring the levels can be helpful after patient admission
*** Although a specific cut-off cannot be defined, a 3-4-fold increase in D-dimer values may be considered significant. Any one of the values in this table may be considered significant
Anticoagulation Forum Interim Guidance Highlights [19]
- Pharmacologic VTE prophylaxis for all hospitalized non-pregnant patients with confirmed or highly suspected COVID-19, regardless of VTE risk assessment score unless contraindication exists (i.e. active bleeding profound thrombocytopenia)
- In patients with contraindications to pharmacologic VTE prophylaxis, consistent application of intermittent pneumatic compression devices with regular assessment for conversion to pharmacologic prophylaxis
- For all non-critically ill hospitalized patients (NOT in an ICU) with confirmed or highly suspected COVID-19, standard dose VTE prophylaxis
- For critically ill patients (IN an ICU) with confirmed or highly suspected COVID-19, suggest higher doses of VTE prophylaxis (i.e. Enoxaparin 40mg subq BID, enoxaparin 0.5mg/kg subq BID, heparin 7500U subq TID, or low-intensity heparin infusion)
- Recommend LMWH > UFH (Unless creatinine clearance <15 – 30mL/min)
- Use anti-Xa assay rather than aPTT to monitor therapeutic UFH in patients with COVID-19 whose aPTT is prolonged at baseline. If not elevated at baseline it is reasonable to monitor therapeutic UFH with either anti-Xa assay or aPTT
- Use anti-Xa assay rather than aPTT to monitor therapeutic UFH in patients with COVID-19 and heparin resistance (typically defined as need for >35,000U of heparin per 24hrs) as measured by aPTT
- Based on current available evidence, do not use daily d-dimer for purpose of guiding anticoagulant therapy. D-dimer measurement may be used as a marker of illness severity and prognosis.
- Do not recommend the use of thrombolytics in patients with COVID-19 outside of a clinical trial setting unless there is another clinical indication for thrombolysis (STEMI, CVA, high-risk (massive)PE with hemodynamic compromise)
My Thoughts/Workflow for LMWH + COVID-19 Positive Patients Being Admitted:
- All patients admitted with COVID-19 should receive thromboprophylaxis in the ED in the absence of any contraindications (Active bleeding or platelet count <25,000)
- The true prevalence of VTE in the ED is unknown at this time
- Treatment and Dosing Decisions:
- No Clot (DVT/PE) + D-dimer <1 – 2ug/L = Lovenox 0.5mg/kg qD (Prophylaxis dose)
- No Clot (DVT/PE) + D-dimer >1 – 2ug/L = Lovenox 1.0mg/kg qD (Higher prophylaxis dose)
- This is a very controversial recommendation and will be dependent on your institution and may change based on newer data
- Clot (DVT/PE) + any D-dimer = Lovenox 1mg/kg BID (Treatment dose)
- If history of HIT or HITT, use a non-heparin alternative
- If anticoagulation contraindicated, use mechanical prophylaxis
- Pts on outpatient DOACs or warfarin as an outpatient (Atrial fibrillation, history of VTE, prosthetic valve) should be switched to treatment dose LMWH
- Anticoagulation at my Shop (San Antonio, TX):
- For Inpatients:
- High Risk: D-Dimer >6x ULN (>3ug/L) = Therapeutic Anticoagulation (TAC)
- Low Risk: D-Dimer <6x ULN (<3ug/L) = Prophylactic Dosing
- For Outpatients (Deemed High Risk for DVT/PE Discharge Plan):
- If no DVT/PE and on TAC during hospital stay + High risk (D-Dimer Still >6x ULN) –> 2 weeks of AC post discharge
- If no DVT/PE and on TAC during hospital stay + High risk (D-Dimer <6x ULN) –> No AC post discharge
- If confirmed DVT/PE, then normal provoked protocol –> AC for 3 – 6mos
- For Inpatients:
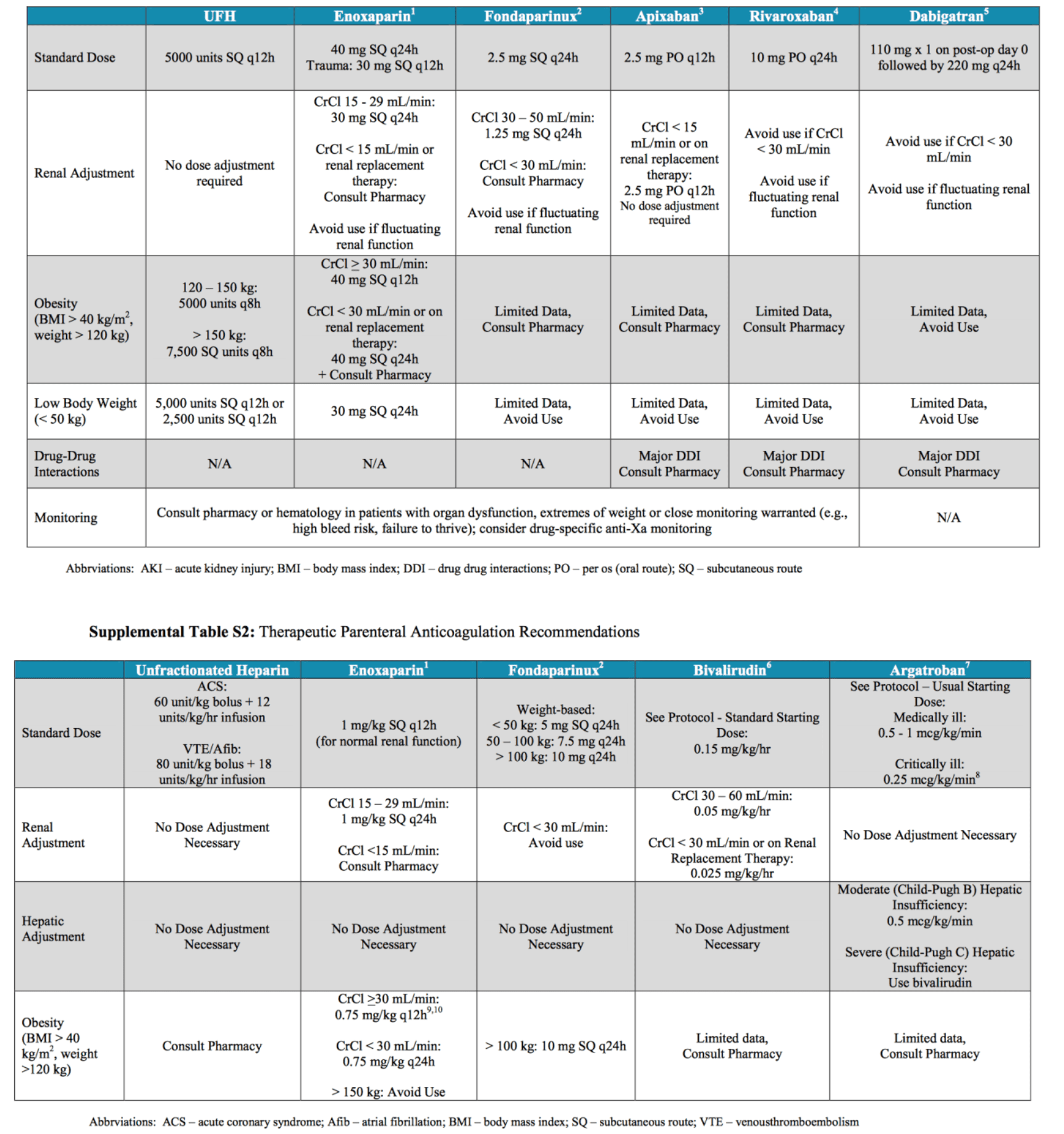
Dosing Guidelines from Massachusetts General Hospital [Link is HERE]
- PDF of Massachusetts General Hospital: Mass Gen Anticoag Recs
JACC Recommendations (Published April 17th, 2020)[11]
- The data derived for recommendations is primary from small and retrospective analyses
- Although older age and comorbidities such as cardiovascular disease have a higher risk for severe disease, young and otherwise healthy patients are also at risk for complications
- Elevated D-dimer levels are associated with higher risk of requiring mechanical ventilation, ICU admission, or death
- Risk Stratification/In-Hospital Prophylaxis
- Prophylactic anticoagulation reduces the risk of VTE in hospitalized medical patients
- The choice of specific risk assessment models will vary across health systems
- Prophylactic daily LMWHs are recommended over twice daily subcutaneous unfractionated heparin (to reduce personal protective equipment use and exposure of staff)
- If pharmacological prophylaxis is contraindicated, mechanical VTE prophylaxis (intermittent pneumatic compression) should be considered in immobilized patients
- Extended (Post-Discharge) VTE Prophylaxis
- Extended prophylaxis with LMWH or DOACs can reduce risk of VTE but comes with a risk of bleeding
- No data specific to COVID-19 exist, however it is reasonable to employ individualized risk stratification for thrombotic and hemorrhagic risk followed by consideration of extended prophylaxis (for up to 45d) for:
- Patients with elevated risk of VTE: Reduced mobility, co-morbidities such as active cancer, and elevated D-dimer>2x the upper limit who have low risk of bleeding
- Quarantined patients with mild COVID-19 but significant co-morbidities, or for patients without COVID-19 who are less active because of quarantine requires more study
- In absence of high-quality data, pharmacological prophylaxis should be reserved for those at highest risk of VTE (limited mobility, history of VTE, or active malignancy)
- Diagnosis of VTE
- Elevated D-dimer is a common finding in patients with CovID-19 and DOES NOT currently warrant routine investigation for acute VTE in absence of clinical manifestations or other supporting information
- Role for Empiric Therapeutic Anticoagulation Without a Diagnosis of VTE
- Some clinicians are using intermediate-dose or full dose therapeutic parenteral anticoagulation
- Existing data on this are very limited, primarily based on subgroup analyses
- The optimal dosing in patients with severe COVID-19 remains unknown
- Medical Therapy for VTE
- Therapeutic anticoagulation is the mainstay of VTE treatment
- Parenteral UFH is preferred as it may be temporarily withheld and has no known drug-drug interactions with investigational COVID-19 therapies
- Concerns with UFH: time to achieve therapeutic aPTT, increased healthcare worker exposure for frequent blood draws
- LMWHs may be the preferred agent in patients unlikely to need procedures
- DOACs lack the need for monitoring, facilitation of discharge planning, and outpatient management
- For patients who are ready for discharge, DOACs or LMWH would be preferred to limit contact of patients with healthcare services
- Interventional Therapies for VTE
- Use of catheter-directed therapies should be limited to the most critical situations
- Intermediate-risk HD stable patients (sub-massive PE) should be managed initially with anticoagulation and close monitoring. Further deterioration should receive rescue systemic fibrinolysis with catheter-directed options as an alternative
- High-risk HD unstable patients (massive PE) should be managed with systemic fibrinolysis with catheter-based therapies reserved for scenarios that are not suitable for systemic fibrinolysis. May also consider ECMO over catheterization laboratory or an operating room
- Incident Acute Coronary Syndromes
- Elevated cardiac troponin or ECG abnormalities are associated with severe disease, however not all such abnormalities are due to thrombotic ACS
- In true ACS due to plaque rupture (Type I MI) dual antiplatelet therapy (DAPT) and full dose anticoagulation are recommended unless there is a contraindication
- In patients with perceived elevated bleeding risk clopidogrel should be considered given that hemorrhagic complications are not uncommon
- It is reasonable to continue optimal medical therapy and defer non-urgent cardiac procedures, in order to preserve PPE, hospital resources including inpatient and ICU beds
- A low threshold to use TTE to identify wall motion abnormalities should be considered prior to catheterization laboratory activation
- Consideration of fibrinolytic therapy in selected patients with STEMI is reasonable however in the setting of myocarditis, fibrinolytic therapy must be used with caution
- Critical Illness and management of Antithrombotic Agents
- Immobility, systemic inflammation, mechanical ventilation, and CVCs contribute to VTE risk within the ICU
- Parenteral anticoagulation is recommended in most cases. UFH can be used in the setting of anticipated procedures or in patients with deteriorating renal function. If no urgent procedures are anticipated LMWHs are a reasonable alternative
- Currently, insufficient data to recommend anticoagulation targets in patients on ECMO
- Additional Considerations:
- Insufficient data to recommend transfusion thresholds that differ from those recommended for other critically ill patients. If invasive procedures are planned, prophylactic transfusion of platelets, FFP, fibrinogen, and PCC may be considered
- TTM may exhibit prolongations of both PT and aPTT without evidence of bleeding. Correction of coagulopathy in unselected patients without overt bleeding is not currently recommended
- DIC
- Diagnosis is best established using the ISTH DIC score calculator
- Monitoring of platelet count, PT, D-dimer, and fibrinogen is recommended
- LMWH prophylaxis may decrease thrombin generation and modify the course of DIC
- Long-acting antiplatelet agents should be discontinued in most patients with DIC unless required (i.e. recent ACS or stent placement)
- Management of Bleeding in DIC
- Overt bleeding is uncommon, but if it occurs:
- Maintain platelet count >50×109/L with active bleeding or >20×109/L in those with high risk of bleeding or requiring invasive procedures
- FFP 15 – 25mL/kg) in patients with active bleeding with prolonged PT and/or aPTT ratios (>1.5x normal) or decreased fibrinogen (<1.5g/L)
- Fibrinogen concentrate or cryoprecipitate is recommended in patients with severe hypofibrinogenemia (<1.5g/L)
- PCC is recommended if FFP transfusion is not possible
- TXA should not be routinely used in COVID-19 associated DIC
Alteplase (tPa) [10]
- Case series of 3 patients mechanically ventilated with COVID-19 ARDS + use of tPA
- Case 1:
- Initial Values:
- P/F ratio = 73
- D-dimer level >50k ng/mL
- Fibrinogen levels 375 – 541 mg/dL
- On day 8 P/F ratio 140 – 240
- Given 25mg tPA IV over 2hrs followed by 25mg infusion over 22hrs
- No bleeding or other complications
- 11hrs into tPA infusion P/F ratio improved to 408
- After tPA started on heparin infusion 10U/kg/hr with PTT goal of 60 – 80
- 1hr into heparin infusion = P/F ratio = 136
- 48hrs post tPA: P/F ratio 188 – 250
- Fibrinogen = 351 mg/dL
- D-dimer = 16,678 ng/mL
- Pt made DNR and expired shortly after
- Case 2:
- Initial Values:
- P/F ratio = 82 (supine) & 130 (prone)
- D-dimer = 545 ng/mL and increased to 20,293 ng/ML by day 9
- Fibrinogen = 939 mg/dL
- IV tPA administered at 25mg IV over 2hrs, followed by 25mg over subsequent 22hrs
- No bleeding or other complications
- After tPA started on heparin infusion 10U/kg/hr with PTT goal of 60 – 80
- At 4hrs into heparin infusion P/F ratio = 135 (prone)
- D-dimer: 40,490 mg/mL
- P/F ratio improved to 135 (supine)
- Case3:
- Initial Values:
- P/F ratio = 120 (prone) and 72 – 90 (supine)
- D-dimer = 33,228 ng/mL
- Fibrinogen 874 mg/dL
- On day 2 given 25mg tPA over 2hrs followed by 25mg infusion over 22hrs
- After tPA re-started on heparin infusion 10U/kg/hr with PTT goal of 60 – 80
- 3hrs after tPA P/F ratio 125
- No bleeding or complications
- 33hrs after tPa infusion:
- P/F ratio 71 (supine) and 118 (prone)
- D-dimer = 37,215 ng/mL
- Fibrinogen = 544 mg/dL
- Initial Values:
- Initial Values:
- Initial Values:
- Case 1:
- Bottom Line: All 3 patients had initial improvement of P/F ratio after tPA, however improvements were transient and lost over time in all 3 patients
Hemoglobin (This section is theoretical at this point and it’s clinical relevance is unknown):
- Hb has 4 subunits
- 2-alpha
- 2-beta
- Each subunit has an iron-bound heme
- Heme = Porphyrin containing iron
- Without iron called porphyrin
- Divalent iron Hb can release CO2 and capture O2 which forms trivalent iron
- When Hb releases O2 the iron becomes divalent
- A study using conserved domain analysis homology modeling, and molecular docking were used to compare biological roles of certain proteins of the SARS-CoV-2 virus and its interaction with hemoglobin [3]
- ORF8 protein and surface glycoprotein bind to porphyrin respectively
- Orf1 ab, ORF10, and ORF3a proteins attack the heme on the 1-beta chain of hemoglobin to dissociate the iron to form porphyrin
- This reduces hemoglobin’s ability to carry oxygen and carbon dioxide
- SARS-CoV-2 binds to porphyrin & attacks heme on Beta-1 chain of Hb -> Dissociates iron from heme -> Hb with decreased O2 affinity -> O2 dissociation curve shifted to right -> release of O2
- Reasons why this theory is most likely wrong:
- It is unclear how SARS-CoV-2 would enter RBCs
- RBCs have no DNA
- Hemoglobin tends to cause hemolysis when altered
- This most likely plays very little role in the low oxygen saturations as the SpO2 seems to match the PaO2 on ABGs
- This just in [12]…
- The authors of this papers give many reasons why the above study should be considered erroneous. Two of the bigger reasons are listed below:
- The above paper [3] is a computational experiment without appropriately assessing clinical significance or considering alternative explanations
- The docking studies used to assess molecular interactions, however there is a huge error..the docking used was evaluated based on the basis of the highest energy, but most stable molecules/complexes are the ones that use the lowest energy
- The authors of this papers give many reasons why the above study should be considered erroneous. Two of the bigger reasons are listed below:
References:
- Chen J et al. Findings of Acute Pulmonary Embolism in COVID-19 Patients. Lancet 2020. [Epub Ahead of Print]
- Zhang Y et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. NEJM 2020. [Epub Ahead of Print]
- COVID-19: Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism. ChemRxiv Preprint 2020. [Epub Ahead of Print]
- Zhou F et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020. PMID: 32171076
- Tang N et al. Anticoagulant Treatment is Associated with Decreased Mortality in Severe Coronavirus Disease 2019 Patients with Coagulopathy. J Thromb Haemost 2020. PMID: 32220112
- Cui S et al. Prevalence of Venous Thromboembolism in Patients with Severe Novel Coronavirus Pneumonia. Journal of Thrombosis and Haemostasis 2020. [Epub Ahead of Print]
- Thachil J et al. ISTH Interim Guidance on Recognition and Management of Coagulopathy in COVID-19. Journal of Thrombosis and Haemostasis 2020. [Epub Ahead of Print]
- Klok FA et al. Incidence of Thrombotic Complications in Critically Ill ICU Patients with COVID-19. Thrombosis Research. [Epub Ahead of Print]
- Fox SE et al. Pulmonary and Cardiac Pathology in COVID-19: The First Autopsy Series from New Orleans. Chemrxiv Pre-Print 2020. [Epub Ahead of Print]
- Wang J et al. Tissue Plasminogen Activator (tPA) Treatment for COVID-19 Associated Acute Respiratory Distress Syndrome (ARDS): A Case Series. J Thromb Haemost 2020. PMID: 32267998
- Bikdeli B et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up. JACC 2020. [Epub Ahead of Print]
- Read RJ et al. Flawed Methods in “COVID-19: Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism” ChemRxiv Prepring 2020 [Epub Ahead of Print]
- Dolhnikoff M et al. Pathological Evidence of Pulmonary Thrombotic Phenomena in Severe COVID-19. Journal of Thrombosis and Haemostasis 2020. [Epub Ahead of Print]
- Tavazzi G et al. Thrombotic Events in SARS-CoV-2 Patients: An Urgent Call for Ultrasound Screening. Intensive Care Med 2020. PMID: 32322918
- Helms J et al. High Risk of Thrombosis in Patients in Severe SARS-CoV-2 Infection: A Multicenter Prospective Cohort Study. Intensive Care Medicine 2020 [Epub Ahead of Print]
- Paranjpe I et al. Association of Treatment Dose Anticoagulation with In-Hospital Survival Among Hospitalized Patients with COVID19. JACC 2020. [Epub Ahead of Print]
- Barnes GD et al. Thromboembolism and Anticoagulant Therapy during the COVID-19 Pandemic: Interim Clinical Guidance from the Anticoagulation Forum. Journal of Thrombosis and Thrombolysis 2020. [Epub Ahead of Print]
- Lax SF et al. Pulmonary Arterial Thrombosis in COVID-19 with Fatal Outcome: Results From a Prospective, Single-Center, Clinicopathologic Case Series. Ann Intern Med 2020. [Epub Ahead of Print]
- Barnes GD et al. Thromboembolism and Anticoagulant Therapy During the COVID-19 Pandemic: Interim Clinical Guidance From the Anticoagulation Forum. J of Thrombosis and Thrombolysis 2020. [Epub Ahead of Print]
For More Thoughts on This Topic Checkout:
- REBEL EM: COVID-19 – The Novel Coronavirus 2019
- PulmCrit: D-Dimer Cutoffs to Predict Thrombosis in COVID-19
- ERCast: COVID-19 – Dimers, Clots, and DIC
- St. Emlyn’s: COVID-19 and Clotting: Diagnosis, D-Dimers, and Dilemmas
- FOAMCast: Autopsy Studies & Venous Thromboembolism
- PulmCrit: Thrombosis Update in COVID-19 – Data from Mount Sinai System in NYC
- Core Ultrasound: COVID and Thrombosis
- PulmCrit: Lupus Anticoagulant in COVID-19 – Culprit or Correlate?
- St. Emlyn’s: Diagnosis and Treatment of VTE in the COVID-19 Era
- PulmCrit: Mythbusting 40mg Enoxaparin Daily for DVT Prophylaxis in Critical Illness
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
Cite this article as: Salim Rezaie, “COVID-19: Thrombosis and Hemoglobin”, REBEL EM blog, April 9, 2020. Available at: https://rebelem.com/covid-19-thrombosis-and-hemoglobin/.







