Authors: Sarah Brubaker, MD (EM Resident at SAUSHEC, US Army) and Brit Long, MD (@long_brit, EM Attending Physician at SAUSHEC) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital)
A 22-year-old female presents to the emergency department with a “fast heart rate” and palpitations. She has experienced this before, but she came today because the current episode is lasting longer than usual. She is slightly dizzy but otherwise asymptomatic. She is in no apparent distress, is breathing comfortably, and has 2+ peripheral pulses. Her vitals are within normal limits except a heart rate of 162. Her EKG is shown below:
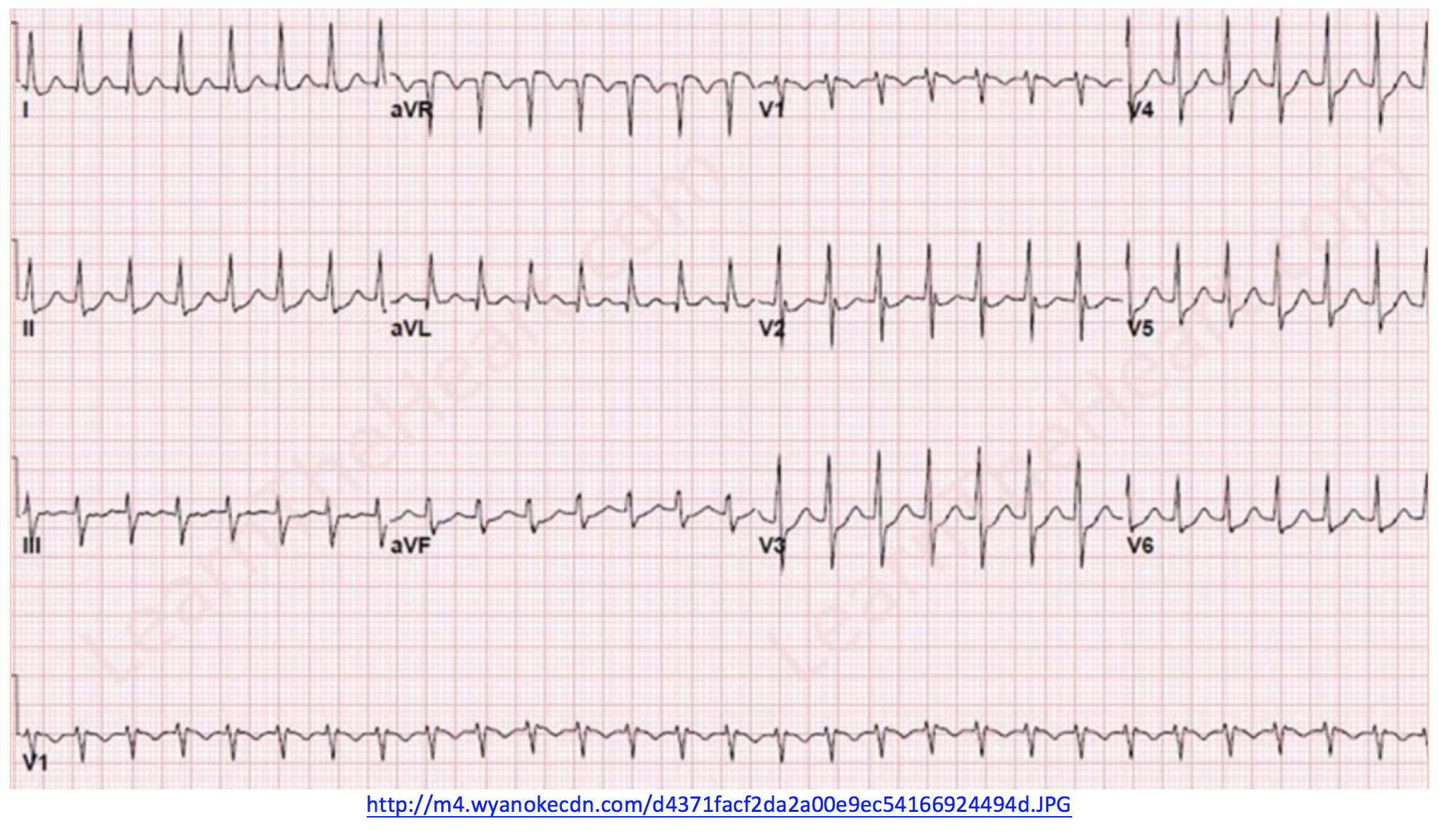
After seeing this EKG, what is your diagnosis? What are your treatment options?
Supraventricular Tachycardia
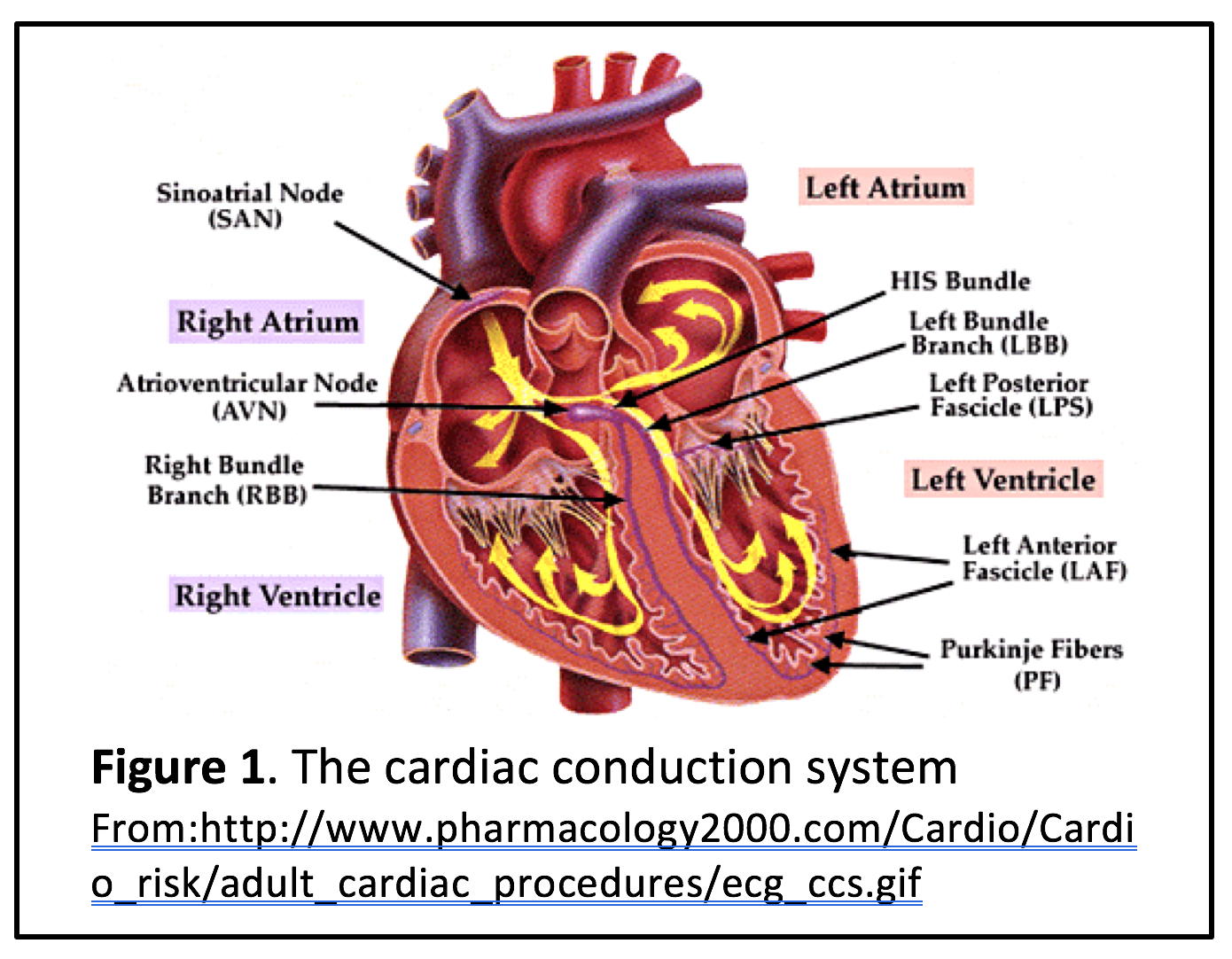
Supraventricular tachycardia (SVT) is a broad term that encompasses all tachydysrhythmias generated “supra” (above) “ventricular” (the ventricles), specifically from any point proximal to the bundle of His (see figure 1) [2]. The term “SVT” is commonly used synonymously with atrioventricular-nodal-reentry tachycardia (AVNRT). However, SVT encompasses AVNRT, atrioventricular re-entrant tachycardia (AVRT), atrial tachycardia, atrial fibrillation, atrial flutter, and multifocal atrial tachycardia (MAT) [3]. To avoid confusion, we will only evaluate AVNRT in this article.
 AVNRT is a regular, narrow-complex tachycardia with a ventricular rate higher than 160 beats per minute [3]. It is the most common cause of palpitations in patients with structurally healthy hearts [2], and its presence alone is rarely indicative of underlying pathology [4]. Patients with AVNRT typically present with rapid-onset, regular palpitations, sometimes with associated shortness of breath, anxiety, and light-headedness [4]. Chest pain is not usually present, but it may occur in patients with underlying CAD or true cardiac ischemia [2]. Although AVNRT can occur spontaneously, it is often provoked by physical activity, emotional stress, hyperthyroidism, or the use of stimulatory substances (caffeine, alcohol, amphetamines, etc.) [2, 3].
AVNRT is a regular, narrow-complex tachycardia with a ventricular rate higher than 160 beats per minute [3]. It is the most common cause of palpitations in patients with structurally healthy hearts [2], and its presence alone is rarely indicative of underlying pathology [4]. Patients with AVNRT typically present with rapid-onset, regular palpitations, sometimes with associated shortness of breath, anxiety, and light-headedness [4]. Chest pain is not usually present, but it may occur in patients with underlying CAD or true cardiac ischemia [2]. Although AVNRT can occur spontaneously, it is often provoked by physical activity, emotional stress, hyperthyroidism, or the use of stimulatory substances (caffeine, alcohol, amphetamines, etc.) [2, 3].
Pathophysiology of AVNRT
In order to make an informed decision regarding the treatment of AVNRT, one must first understand its underlying pathophysiology. The name is actually quite descriptive: the arrhythmia arises secondary to a re-entry circuit within the AV node, generally in the presence of normal electrical conduction distal to the AV node. Because the ventricles are able to depolarize at a normal speed, the QRS complex is narrow-complex, with normal morphology. Wide-complex AVNRT can occur in patients with pre-existing bundle branch blocks. P-waves are usually either buried in the QRS complex or appear retrograde to the QRS complex. Diffuse ST depressions may be seen. However, these depressions are rate-dependent and should resolve with resolution of AVNRT to normal sinus rhythm. If the ST depressions persist and are new (compared to previous EKGs), the patient requires admission and further evaluation for cardiac ischemia.
To appropriately treat AVNRT, one must disrupt the cycles of refractory pathways that result in the re-entry circuit within the AV-node. Thus, AVNRT is usually highly responsive to agents that either block or slow conduction through the AV node. So with that background, let’s move on to the myriad agents that are available to serve this purpose.
Treatment options
Per ACLS and AHA guidelines, the first-line treatment for stable AVNRT is vagal maneuvers, such as Valsalva or carotid sinus massage. These maneuvers effectively achieve cardioversion in approximately 28% of patients [5]. However, the efficacy drastically increases when using the “modified Valsalva” technique described in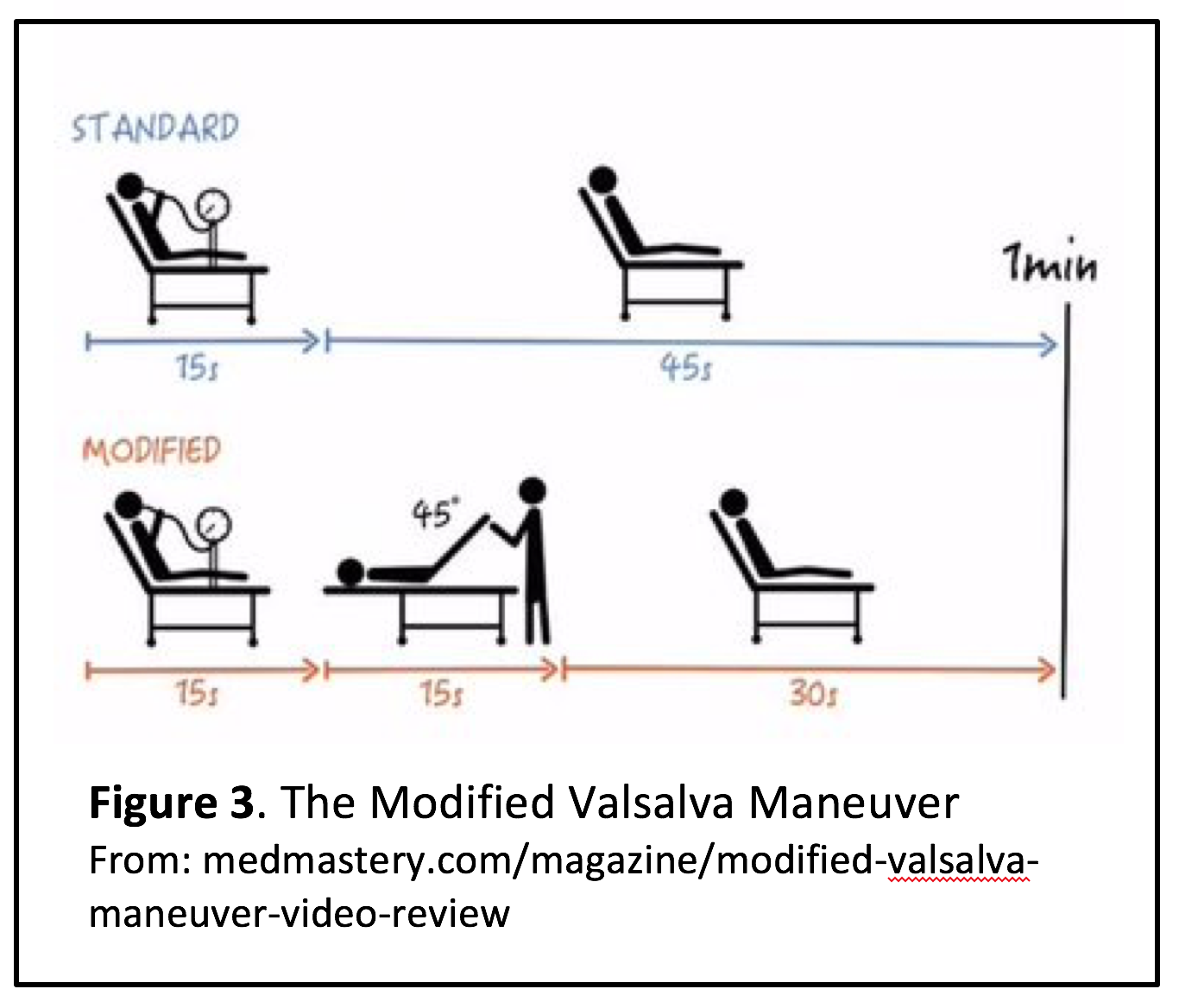 the REVERT trial [6]. In order to complete the maneuver, place the patient at a 30 degree angle, and then have him blow into a 10cc syringe for 15 seconds. Quickly lay the patient flat, and raise his legs to 45 degrees for 15 seconds. Lastly, sit the patient fully upright for 30 seconds (see figure 3). The initial study demonstrated successful conversion to sinus rhythm in 43% of patients [6], with a number needed to treat of 3 [7].
the REVERT trial [6]. In order to complete the maneuver, place the patient at a 30 degree angle, and then have him blow into a 10cc syringe for 15 seconds. Quickly lay the patient flat, and raise his legs to 45 degrees for 15 seconds. Lastly, sit the patient fully upright for 30 seconds (see figure 3). The initial study demonstrated successful conversion to sinus rhythm in 43% of patients [6], with a number needed to treat of 3 [7].
If vagal maneuvers fail, most guidelines recommend the use of adenosine [8, 9], which slows conduction at the AV node. Adenosine is initially administered as 6 mg IV rapid-push bolus, followed by a normal saline flush. Because adenosine’s onset of action and maximum duration of action are both approximately 10 seconds [10], a response should be seen rapidly. If the tachycardia recurs or persists within 1-2 minutes of adenosine administration, it can be re-administered as a 12 mg dose up to two times. Studies consistently demonstrate approximately 90% termination of SVT within 30 seconds when two or more doses are used [11-13]. However, there are several circumstances in which adenosine may not be efficacious at the standard doses. The most notable example is the recent use of caffeine (also methylxanthines). Caffeine binds to the same receptor as adenosine, so it acts as a competitive adenosine receptor antagonist [10]. One case-control study in 2010 concluded ingestion of caffeine within the last four hours significantly decreases the odds of successful termination of AVNRT with adenosine [14]. However, this effect has not been well-studied, and various factors such as chronicity of use and dose may play an important role in this interaction [15].
Because adenosine’s half-life is less than ten seconds [16], it is important to administer the medication through an intravenous line as proximally as possible. Peripheral intravenous access is acceptable, but one study did demonstrate increased efficacy of adenosine at lower doses if a central line is used [17].
Adenosine receptors are highly concentrated in the AV node, but they are also present throughout the body [10]. Therefore, adenosine dilates the coronary arteries and peripheral vasculature, while also causing transient bronchoconstriction. This results in the characteristic chest tightness, shortness of breath, and flushing that transiently occur within a few seconds of adenosine administration [16].
Although asthma is not a contraindication to adenosine use, it may be reasonable to avoid its use in asthmatic patients, due to its bronchoconstrictive effects [10]. In addition, adenosine use should be avoided in patients with recent dipyridamole use, as dipyridamole inhibits the metabolism of adenosine and prolongs its effects. Dosing should be reduced in patients with heart transplants or if the medication is provided via central access. One of the most significant contraindications to adenosine is its high side-effect profile. Many patients find the medication to be so intolerable that they may prefer alternate options.
—–
You attempt the modified Valsalva maneuver three times. With each attempt, the heart rate transiently decreases to 100, but returns to the 160s within thirty seconds. Next, you give the patient two doses of adenosine (6 mg, 12 mg bolus). Again, there is a transient response but the heart rate returns to the 160s. The adenosine made the patient temporarily miserable, but she is otherwise asymptomatic.
What are your treatment options, now that the patient has failed both vagal maneuvers and adenosine? And are there other options that won’t result in the horrible feeling associated with adenosine?
—–
Treatment of AVNRT refractory to adenosine
If the tachycardia does not appropriately respond to adenosine, you should first ask the question, “Is this actually AVNRT?” It can often 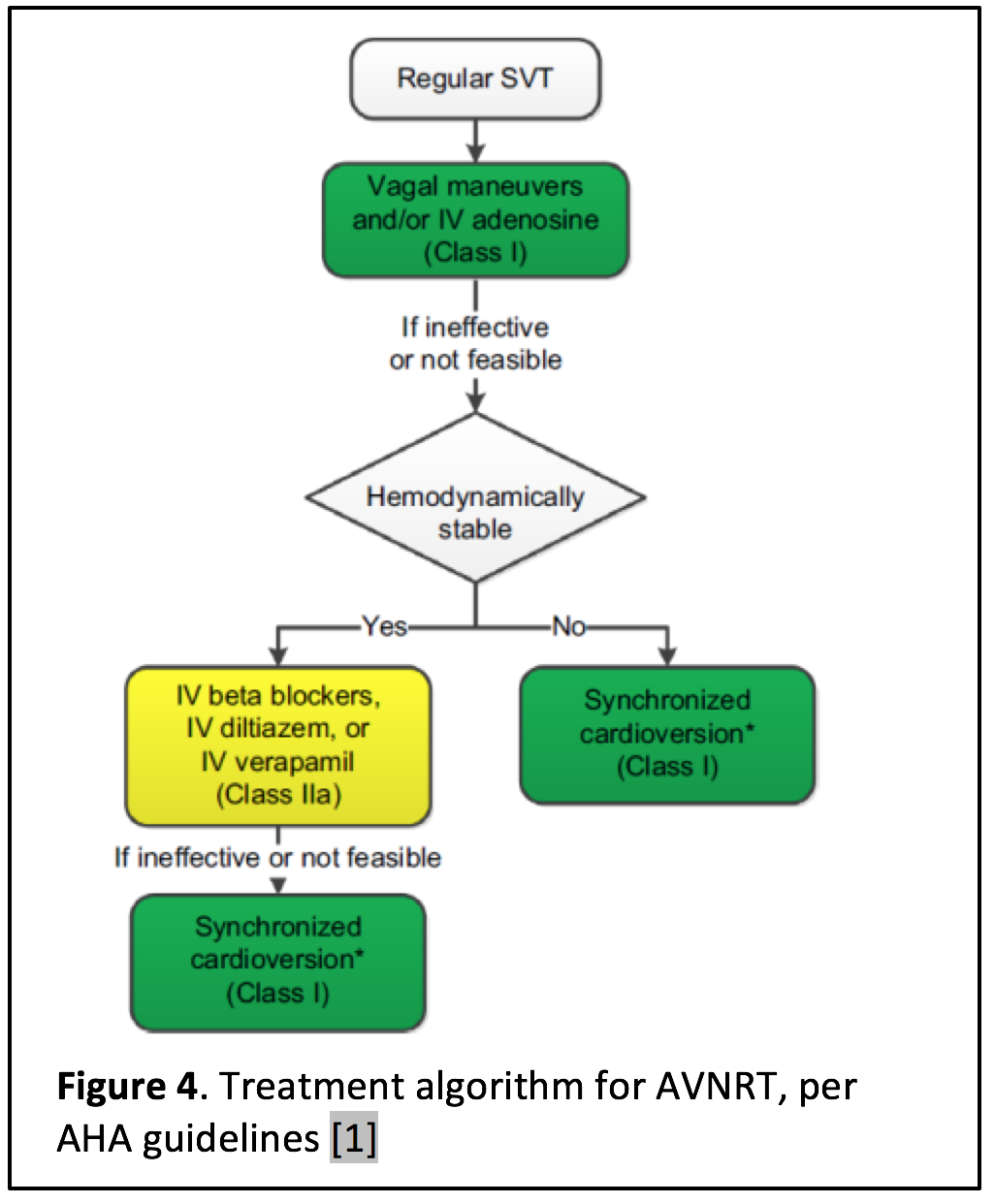 be difficult to distinguish AVNRT from other types of SVT. Because adenosine slows conduction at the AV node but does not affect automaticity of atrial dysrhythmias, the administration of adenosine may unmask an underlying rhythm such as atrial flutter or atrial fibrillation [1, 2, 4, 18]. Inappropriate sinus rhythm can also mimic AVNRT.
be difficult to distinguish AVNRT from other types of SVT. Because adenosine slows conduction at the AV node but does not affect automaticity of atrial dysrhythmias, the administration of adenosine may unmask an underlying rhythm such as atrial flutter or atrial fibrillation [1, 2, 4, 18]. Inappropriate sinus rhythm can also mimic AVNRT.
If you confidently believe the 12-lead EKG is consistent with AVNRT, then you can proceed down the “refractory AVNRT pathway” as depicted in the figure 4, extracted from 2015 AHA guidelines.
Calcium-Channel Blockers
Although adenosine is recommended by the AHA as first-line treatment for AVNRT [9], the evidence supporting this recommendation is almost solely derived from studies performed in the 1990s. In addition, recent literature suggests that non-dihydropyridine calcium channel blockers (verapamil and diltiazem) may be equally as efficacious as adenosine [5, 18-20].
Adenosine has a much shorter half-life compared to verapamil and diltiazem, so while adenosine acts more rapidly than calcium channel blockers, its effects are also more short-lived. Adenosine’s onset of action is approximately 10 seconds [10], compared to 2 to 5 minutes for diltiazem and verapamil [21, 22]. Remember, the duration of action for adenosine is approximately 10 seconds, compared to a median value of more than four minutes for either verapamil or diltiazem [21-23].
Two meta-analyses of high-quality randomized controlled trials demonstrated that while adenosine is more rapid-acting than verapamil, there is no statistically significant difference in conversion rate between the two medications [19,20]. Both medications resulted in a conversion rate of approximately 90%, but there were significantly more “minor adverse effects” (flushing, chest discomfort, etc.) when adenosine was used. Diltiazem has not been extensively studied as a treatment for AVNRT, but one study demonstrates successful conversion to sinus rhythm in 90-100% of cases, at efficacy rates comparable or superior to adenosine [24].
Per current ACLS and AHA guidelines, the recommended dose of verapamil is 2.5-5.0 mg IV bolus given over 2-4 minutes. A dose of 5 mg can be repeated every 15-30 minutes, until a total dose of 20 mg is reached [5, 9]. Verapamil can also be given as an infusion at a rate of 1 mg/min, until termination of AVNRT or a total dose of 20 mg. Diltiazem is initially given at a dose of 0.25 mg/kg (max dose 20 mg) given over 2 minutes, followed by a second dose of 0.35 mg/kg (max dose 25) if the SVT does not resolve within 15 minutes. Alternatively, diltiazem can be given as an infusion at a rate of 2.5 mg/min, until termination of AVNRT or a total dose of 50 mg.
A prospective randomized control trial in 2009 investigated the efficacy of slow-infusion of calcium channel blockers compared to adenosine bolus [25]. The study demonstrated a significantly higher conversion rate in the calcium channel blocker group (98%) compared to the adenosine group (86.5%). While patients receiving calcium channel blockers did experience greater decreases in blood pressure compared to the adenosine group, only 1% of patients developed true hypotension. Thus, administering calcium channel blockers as a slow-infusion may be superior to bolus-dosing, as it may lower the risk for hypotension. Although it has not been well-studied, one study in 1987 posited that the concomitant administration of calcium with verapamil may increase the efficacy and decrease the risk of hypotension without affecting its efficacy [26]. However, this study only evaluated six patients with AVNRT, and no studies have confirmed this finding.
In addition to the possibility of hypotension, the administration of these medications in the setting of ventricular tachycardia may lead to hemodynamic instability or ventricular fibrillation [1]. Other contraindications include hypotension, systolic heart failure, shock, pregnancy, and history of Wolf-Parkinson-White syndrome or heart block [21].
Beta Blockers
There is little evidence to support the use of beta blockers to treat AVNRT; even the current AHA guidelines are based on studies from the 1980s and 1990s. Initial studies demonstrated a 93% percent success rate for the conversion of AVNRT to sinus rhythm [27]. However, later studies found beta blockers to have a lower conversion rate and higher risk of hypotension compared to calcium channel blockers. A study in 1999 that compared esmolol to diltiazem was terminated early because diltiazem was clearly superior to esmolol [28, 29]. Nonetheless, AHA guidelines recommend the use of beta blockers in hemodynamically stable patients who are unable to tolerate calcium channel blockers [9].
Electrical Cardioversion
AVNRT is generally not indicative of underlying structural pathology [4]. In addition, it rarely results in end-organ hypoperfusion. Thus, although synchronized cardioversion is highly effective in terminating all types of SVT [30], it is generally not necessary in suspected AVNRT. Electrical cardioversion is generally reserved for hemodynamically unstable patients or patients who fail pharmacologic cardioversion [1, 9]. The procedure is highly uncomfortable, and the patient should be adequately sedated before cardioversion is pursued.
If electrical cardioversion is necessary, AHA guidelines recommend biphasic cardioversion, at a starting dose of 50J to 100J [1, 9]. If the initial electrical impulse fails, the dose can be doubled before a second dose is administered.
—–
Because your patient is stable, you administer 15 mg diltiazem intravenously based on weight. Within 10 minutes, her heart rate is consistently in the 90s. After you monitor her for AVNRT recurrence, she continues to have no complaints, her palpitations have resolved, her heart rate is in the high 90s, and you believe she is ready for discharge.
As you are preparing her discharge instructions, you ask yourself, “should I send her home with any maintenance medications?”
—–
Discharge recommendations
Most patients with paroxysmal AVNRT can safely be discharged after successful cardioversion [1, 3, 9]. The patient should receive an outpatient referral to a cardiologist, who may choose to obtain electrophysiological testing. If the patient experiences several episodes of AVNRT, or symptomatic AVNRT, then the cardiologist may choose to proceed with ablation therapy.
Before discharge, the patient should be taught how to perform vagal maneuvers (AHA Class I, Level C recommendation). If the patient experiences recurrent AVNRT and is able to terminate the dysrhythmia at home, then the episode does not warrant an ED visit. Medications are not routinely recommended after a single episode of AVNRT. However, it may be appropriate to prescribe an oral beta blocker or calcium channel blocker to patients with frequent recurrences. Oral verapamil, prescribed in doses up to 480 mg/day, has been demonstrated to reduce the number and duration of episodes [31]. Although beta-blockers are also commonly prescribed for this purpose, evidence is limited [9].
Conclusion
As emergency medicine physicians, we often take an algorithmic approach to tachydysrhythmias. Although this is appropriate in cases of unstable tachycardia, patients with AVNRT are usually stable. Thus, such patients present optimal opportunities to consider the pathophysiology of the underlying disease and treat as such. In addition, this is an appropriate time to discuss treatment options with the patient and utilize shared-decision making.
Adenosine is currently recommended by several guidelines, in part because it is well-established and efficacious in treating AVNRT. However, adenosine is associated with significantly unpleasant, albeit short-lived, side effects. Literature within the past ten years suggests that other options, such as non-dihydropyridine calcium channel blockers and beta blockers, are equally effective as adenosine and are also more tolerable. Beta blockers are known to be less efficacious than other pharmacologic options, but they may be used in patients who are unable to tolerate calcium channel blockers.
Summary
-For treatment of narrow-complex tachycardia, ACLS and AHA guidelines recommend the use of vagal maneuvers, followed by adenosine.
-Adenosine causes short-lived unpleasant flushing, chest pain, lightheadedness, or shortness of breath.
-However, non-dihydropyridine calcium channel blockers (verapamil and diltiazem) are equally efficacious, without the negative (albeit short-lived) side effects of adenosine. If given over 20 minutes, the risk for hypotension is low.
| Intervention | Dose | Advantages | Disadvantages |
| Vagal maneuvers
(modified Valsalva) |
-Place patient at a 30 degree angle, have patient blow into a 10cc syringe for 15 seconds
-Lie patient flat, raise legs to 45 degrees for 15 seconds -Sit patient fully upright for 30 seconds |
-No-cost, easy, does not require pharmacologic intervention
-Low-risk |
-Efficacy rate ~50% (with modified Valsalva maneuver) |
| Adenosine | 6 mg bolus, followed by flush
If unsuccessful, 12 mg bolus (up to two 12 mg doses, if each bolus is unsuccessful after 1-2 minutes) |
-Rapid onset of action
-AV-nodal-blocking activity may unveil an alternate form of SVT (e.g. atrial fibrillation, atrial flutter) -Efficacy rate ~90% |
-Significant short-term side effects and discomfort to patient
-Higher recurrence rate than CCBs |
| Calcium channel blockers | Verapamil: Bolus – 2.5-5.0 mg IV, given over 2-4 minutes (may repeat 5 mg dose every 15-30 minutes to max dose 20 mg). Infusion: 1mg/min, until termination of AVNRT or total dose of 20 mg
Diltiazem: Bolus – 0.25 mg/kg (max dose 20 mg), given over 2 minutes; may repeat dose at 0.35 mg (max dose 25 mg) in 15 minutes. Infusion: 2.5 mg/min, until termination of AVNRT or total dose of 50 mg |
-Lower recurrence rate than adenosine
-Efficacy rate ~90% (perhaps as high as 98% if given as slow infusion) |
-Longer onset of action
-Contraindicated in systolic heart failure, hypotension (SBP <120), shock, pregnancy, history of WPW or heart block |
| Beta blockers | Propranolol: 1 mg IV bolus over 2 minutes
Esmolol: 500 mcg/kg IV bolus over 1 minute |
May be used if patient is unable to tolerate calcium channel blockers
|
**Not as efficacious as calcium channel blockers or adenosine, although poorly studied |
There are several great FOAM resources regarding up-to-date practice of SVT management. Here are some of our favorites:
- https://www.aliem.com/2016/calcium-channel-blockers-stable-svt-alternative-to-adenosine/
- https://coreem.net/core/avnrt/
If you are curious about the REVERT trial, here are some resources:
- Original study: Appelboam, A., et al. (2015). “Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial.” The Lancet 386(10005): 1747-1753.
- Lancet video on how to properly perform the maneuver: https://youtu.be/8DIRiOA_OsA
- http://rebelem.com/the-revert-trial-a-modified-valsalva-maneuver-to-convert-svt/
- http://www.acepnow.com/article/modified-valsalva-maneuver-better-way-manage-supraventricular-tachycardia/2/
References/Further Reading
- Link, M.S., et al., Part 6: Electrical Therapies Automated External Defibrillators, Defibrillation, Cardioversion, and Pacing2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2010. 122(18 suppl 3): p. S706-S719.
- Burns, E., Supraventricular Tachycardia (SVT), in Life in the Fast Lane, M. Cadogan and C. Nickson, Editors. 2012.
- Yealy, D.M. and J.M. Kosowsky, Dysrhythmias, in Rosen’s emergency medicine-concepts and clinical practice. J. Marx, R. Walls, and R. Hockberger, Editors. 2013, Elsevier Health Sciences: St. Louis, MO. p. 1034-1063.
- Delacrétaz, E., Supraventricular tachycardia. New England Journal of Medicine, 2006. 354(10): p. 1039-1051.
- Craig, S.A., Tachyarrythmias in the ED: Best evidence. Emergency Medicine Practice, 2003. 5(2): p. 24.
- Appelboam, A., et al., Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. The Lancet, 2015. 386(10005): p. 1747-1753.
- Rezaie, S., The REVERT Trial: A modified Valsalva maneuver to convert SVT. R.E.B.E.L. EM, 2016.
- Link, M.S., et al., Part 7: adult advanced cardiovascular life support 2015 american heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation, 2015. 132(18 suppl 2): p. S444-S464.
- Page, R.L., et al., 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation, 2015: p. 10.1161/CIR. 0000000000000311.
- Wilbur, S.L. and F.E. Marchlinski, Adenosine as an antiarrhythmic agent. The American journal of cardiology, 1997. 79(12): p. 30-37.
- Hood, M.A. and W.M. Smith, Adenosine versus verapamil in the treatment of supraventricular tachycardia: a randomized double-crossover trial. American heart journal, 1992. 123(6): p. 1543-1549.
- Marco, C.A. and J.F. Cardinale, Adenosine for the treatment of supraventricular tachycardia in the ED. The American journal of emergency medicine, 1994. 12(4): p. 485-488.
- Hood, M.A. and W.M. Smith, Adenosine versus verapamil in the treatment of supraventricular tachycardia: a randomized double-crossover trial. American heart journal, 1992. 123(6): p. 1543-1549.
- Cabalag, M.S., et al., Recent caffeine ingestion reduces adenosine efficacy in the treatment of paroxysmal supraventricular tachycardia. Academic Emergency Medicine, 2010. 17(1): p. 44-49.
- Karydes, H.C. and S.M. Bryant, Adenosine and Caffeine‐induced Paroxysmal Supraventricular Tachycardia. Academic Emergency Medicine, 2010. 17(5): p. 570-570.
- Adenoscan IV (adenosine injection) for rapid bolus intravenous use. U.S. Food and Drug Administration, 2015.
- Chang, M. and K. Wrenn, Adenosine dose should be less when administered through a central line. The Journal of emergency medicine, 2002. 22(2): p. 195-198.
- Al-Khatib, S.M. and R.L. Page, Ongoing Management of Patients With Supraventricular Tachycardia. JAMA cardiology, 2016.
- Delaney, B., J. Loy, and A.-M. Kelly, The relative efficacy of adenosine versus verapamil for the treatment of stable paroxysmal supraventricular tachycardia in adults: a meta-analysis. European Journal of Emergency Medicine, 2011. 18(3): p. 148-152.
- Holdgate, A. and A. Foo, Adenosine versus intravenous calcium channel antagonists for the treatment of supraventricular tachycardia in adults. The Cochrane Library, 2006.
- Cardizem (Diltiazem). Package Insert.
- Hospira, I., Verapamil Hydrochloride Injection. Package Insert.
- Diltiazem package insert. Hospira, Inc.
- Dogan, H., et al., To decide medical therapy according to ECG criteria in patients with supraventricular tachycardia in emergency department: adenosine or diltiazem. International journal of clinical and experimental medicine, 2015. 8(6): p. 9692.
- Lim, S., et al., Slow infusion of calcium channel blockers compared with intravenous adenosine in the emergency treatment of supraventricular tachycardia. Resuscitation, 2009. 80(5): p. 523-528.
- Haft, J.I. and M.A. Habbab, Treatment of atrial arrhythmias: Effectiveness of verapamil when preceded by calcium infusion. Archives of internal medicine, 1986. 146(6): p. 1085-1089.
- Das, G., et al., Efficacy of esmolol in the treatment and transfer of patients with supraventricular tachyarrhythmias to alternate oral antiarrhythmic agents. The Journal of Clinical Pharmacology, 1988. 28(8): p. 746-750.
- Sohinki, D. and O.A. Obel, Current trends in supraventricular tachycardia management. The Ochsner Journal, 2014. 14(4): p. 586-595.
- Gupta, A., et al., Comparison of efficacy of intravenous diltiazem and esmolol in terminating supraventricular tachycardia. The Journal of the Association of Physicians of India, 1999. 47(10): p. 969-972.
- Roth, A., et al., Effectiveness of prehospital synchronous direct-current cardioversion for supraventricular tachyarrhythmias causing unstable hemodynamic states. The American journal of cardiology, 2003. 91(4): p. 489-491.
- Mauritson, D.R., et al., Oral Verapamil for Paroxysmal Supraventricular TachycardiaA Long-Term, Double-Blind Randomized Trial. Annals of internal medicine, 1982. 96(4): p. 409-412.








4 thoughts on “Treatment of Refractory SVT: Pearls and Pitfalls”
Hi Sarah, thank you.
This is a crystalline, amazing contribution in clarifying each single step of managing patients with AVNRT.
As a quite mature Emergency Physician, I believe your comment matches my last ten years of practice.
This is what I try to pass everyday onto our juniors in order to gain their competence, confidence and joy in a truly unique discipline.
Well done!!!
Hi Sarah, thank you.
This is a crystalline, amazing contribution in clarifying each single step of managing patients with AVNRT.
As a quite mature Emergency Physician, I believe your comment matches my last ten years of practice.
This is what I try to pass everyday onto our juniors in order to gain their competence, confidence and joy in a truly unique discipline.
Well done!!!
Pingback: Länkar v10 | Internmedicin
Great summary. Succinct and to the point. Thanks for posting. I’m teaching this to medical students and will refer them to your site.