Author: Brett A Hayzen, MD (EM Chief Resident, UTSW / Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
Case:
A 23 year-old male who was riding a motorcycle in front of a High School crowd lost control and ran into the bleachers, with trauma to the anterior neck. EMS arrived and placed King Tube and C-collar. Upon arrival in ED, the patient was noted to have blood spurting out of King Tube, was tachycardic and hypotensive, GCS 5, but with no other outward signs of trauma (no abrasions, lacerations, ecchymosis) – impressively unimpressive visual appearance.
Initial vital signs – HR: 130s, BP: 80/60, O2: 61%
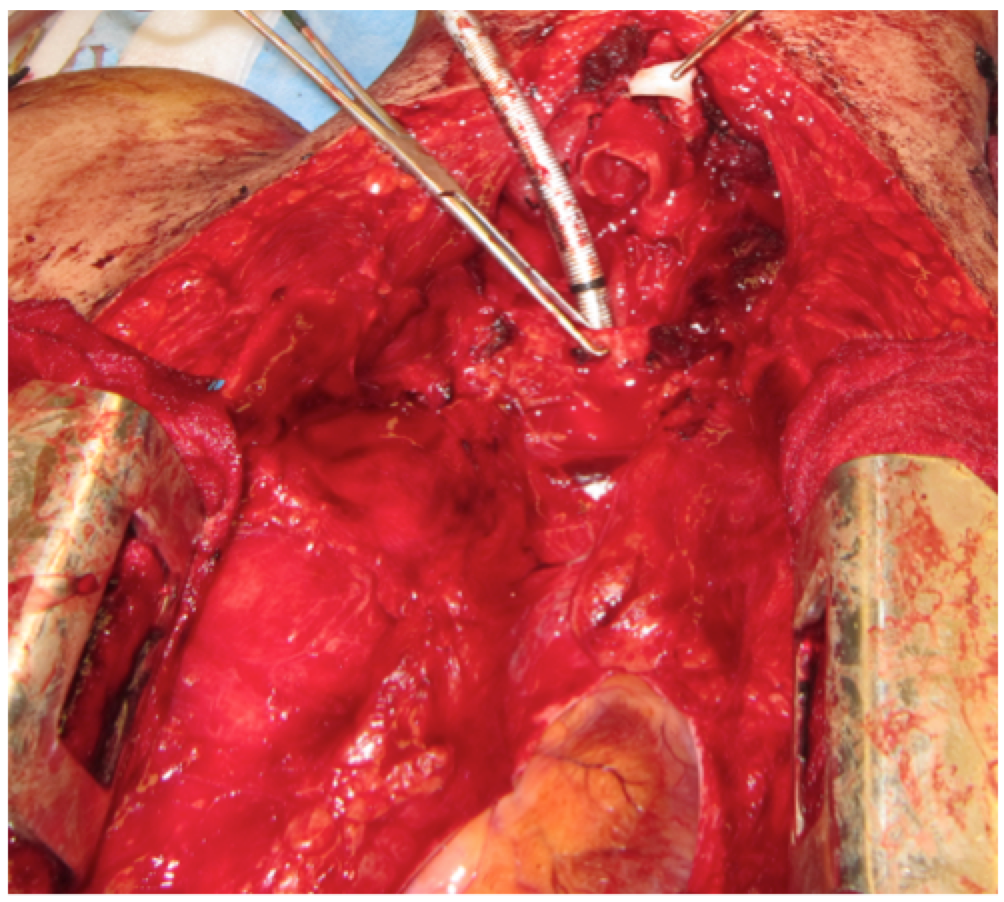
Upon exam, the patient had gurgling breath sounds bilaterally and significant crepitus from neck down to below the nipple line bilaterally. The ED team managing the airway immediately recognized that this would be a very difficult airway – the oropharynx was full of blood, tongue was swollen, and neck was enlarged secondary to subcutaneous emphysema. The decision was made to perform cricothyrotomy. A large vertical incision was made, and it was immediately apparent that the trachea was completely transected, with the distal portion at the level of the sternal notch. An endotracheal tube was placed in the distal portion. Bilateral chest tubes were also placed simultaneously with minimal return of air. The patient was taken emergently to the OR where a sternotomy was performed and ENT repaired the trachea and placed a tracheostomy. The cricoid cartilage and membrane were fractured and were therefore resected. He underwent a primary repair with an anastomosis from thyroid cartilage to 2nd tracheal ring. The patient also had esophageal repair and G-tube placed.
List of injuries: Tracheal transection, esophageal injury, acute right MCA infarct, subdural hematoma, C1 posterior arch fracture, type III Odontoid fracture, T2 burst fx with minimal retropulsion, right 1st rib fracture, bilateral hemopneumothoraces, and bilateral pulmonary contusions.
Tracheal Injuries are rare diagnoses with < 2% occurring after chest trauma. Injuries sufficient to result in severe laryngotracheal damage can also easily damage the cervical spine (as many as 50% of cases), esophagus, and vascular structures.
Iatrogenic damage is more common with up to 18% of emergent intubations end up with tracheal injuries, often as a result of overinflated cuffs, or perforation from the stylet/ETT. Those most likely to suffer tracheal injuries are the elderly, very young, or patients with history of heavy steroid use or chemotherapy and/or radiation.
There is significant mortality associated with tracheal injuries (approximately 30%), half of which occurring in the first hour due to inadequate airway and tension pneumothorax. Associated morbidity includes tracheal stenosis, atelectasis, pneumonia, mediastinitis, sepsis, and decreased pulmonary function.
The two main classifications of trauma are blunt and penetrating:
Blunt trauma – The most common cause of blunt laryngotracheal trauma is motor vehicle accidents. Patients typically present with dyspnea, dysphonia, neck pain, dysphagia, odynophagia, and hemoptysis. Physical findings may include subcutaneous emphysema, tenderness, edema, hematoma, ecchymosis, and distortion or loss of laryngeal landmarks. Laryngotracheal injuries are often unrecognized because the severity of the symptoms does not always correspond with the extent of injury.
Penetrating trauma – Usually more obvious, but it is vital to fully assess both entry and exit wounds carefully as there may be bone/cartilage fragments causing obstruction. Additionally, penetrating objects are more likely to causes damage to surrounding structures. Injuries may be obscured by subcutaneous emphysema. Patients often have pneumothoraces / pneumomediastinum – which may delay detection of laryngotracheal injuries.
Initial management – As always, securing an adequate airway and immobilizing the cervical spine should be the first steps. Airway management may entail cricothyroidotomy / tracheotomy. Endotracheal intubation may be difficult in the presence of spinal, facial, or cervical trauma. Even in cases of only limited intraluminal injury, intubation may exacerbate the situation, so tracheotomy is preferred for patients with a severe laryngeal injury. Also concomitant injuries – such as those to the tongue, jaw, or spine – may preclude safe intubation. In these cases, a controlled tracheotomy over a laryngeal mask airway or over a rigid ventilating bronchoscope can be performed.
Intubation is best performed under direct vision (preferably fiber-optic or rigid endoscopy). A smaller tube with a high-volume, low-pressure cuff is preferable. Early involvement of ENT is highly recommended, as the larynx and trachea need to be fully assessed as they may become affected by secondary inflammation, infection, and further damage secondary to the superimposed presence of the tube. Prolonged intubation poses a significant risk of complications that must not be overlooked or underestimated.
Take home points:
-Traumatic injuries to the larynx or trachea are not always very obvious – have a high suspicion when you have trauma to the anterior neck
-Always look for concomitant injuries to adjacent structures (c-spine, vascular, esophagus)
-Use fiber-optics to intubate and to fully assess the oropharynx and laryngotracheal structures
-Get ENT involved early
References / Further Reading:
-Walter et al. Acute external laryngotracheal trauma: Diagnosis and management. Ear Nose & Throat J 2006 v85 p179-84
-Brett T. Comer, MD, and Thomas J. Gal, MD; Recognition and Management of the Spectrum of Acute Laryngeal Trauma; The Journal of Emergency Medicine, Vol. 43, No. 5, pp. e289–e293, 2012
-Randall et al.: Laryngotracheal Trauma Incidence and Outcomes; Laryngoscope 124: April 2014
-Natarajan A, Sanders GM, et al. A case of anterior tracheal rupture following trivial trauma. Chest Medicine On Line. January 2006. January 23, 2008. On-Line
-Barmada H, Gibbons JR, et al. Tracheobronchial injury in blunt and penetrating chest trauma. Chest 1994. July;106 (1):74 78.







