
Author: Courtney Cassella, MD (EM Resident Physician, Icahn School of Medicine at Mount Sinai) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)

Definitions
- AF – Atrial fibrillation
- Paroxysmal – Terminates spontaneously or with intervention within 7d
- Persistent – Continuous >7d
- Long-standing persistent – >12mo
- Permanent – Persistent for which cardioversion has failed or has not been attempted
- Nonvalvular – AF in absence of rheumatic mitral stenosis, a mechanical or bioprosthetic heart valve, or mitral valve repair
- BB – β-blocker
- CCB – Nondihydropyridine Calcium Channel Blocker
Etiology/triggers
When a patient presents in new onset or rapid AF, a priority should be to identify and treat underlying disease or precipitating factors. The PIRATES mnemonic is a helpful reminder although it is not complete.
=>PIRATES mnemonic
Pulmonary disease (COPD, PE)
Ischemia (ACS)
Rheumatic heart disease (mitral stenosis)
Anemia (high output failure/tachycardia)/Atrial Myxoma
Thyrotoxicosis
Ethanol/Endocarditis
Sepsis/Sick Sinus Syndrome
=>Causes not included in the mnemonic:
Electrolyte abnormalities
Congestive heart failure
Medications/Drugs
Myocarditis/Pericarditis
High sympathetic tone states: sepsis, post-operative, hypovolemia
Acute Management
=>Rate versus Rhythm Control
The RACE1, 2 and AFFIRM3 studies demonstrate rhythm-control has no survival benefit over rate-control. It is prudent to purse rate control in the acute setting since it is contraindicated to cardiovert stable patients with AF >48 hours or unknown duration without anticoagulation. Therefore, for stable patients without pre-excitation, intravenous BB or CCB are recommended to slow rapid AF.4-12
=>β-Blocker (BB) versus Nondihydropyridine Calcium Channel Blocker (CCB)
Between a BB and CCB, which is the best medication? The decision often encompasses multiple factors including contraindications, physician comfort, home medications, pharmacodynamics, etc.
In regards to home medications, it may benefit patients to continue the same class of home medication. Mixing BB and CCB, although sometimes necessary for rate control, may act synergistically potentiating AV nodal blockade, bradycardia, and hypotension.13-15
-
β-Adrenergic Antagonist16
- β 1 (80% cardiac β receptors) receptor stimulation
- Increases inotropy and chronotropy
- β 2 receptor stimulation
- Increases inotropy, relaxation, and chronotropy
- Mediates bronchodilation
- Decreases systemic vascular resistance
- Mechanism: Blocks β -adrenergic stimulation
- β 1 selective antagonist – decrease inotropy and chronotropy
- Esmolol
- Metoprolol
- T1/2 3-4 hours
- Oral formulation both short and long acting
- Atenolol
- T1/2 5-9 hours
- Oral formulation
- Carvedilol
- Additional: Acebutolol, Betaxolol, Bisoprolol, Celiprolol, Nebivolol
- Contraindications:
- Active wheeze in reactive airway disease (asthma, COPD) – Although β 1-blockers are cardioselective, studies demonstrate they decrease FEV1 and PEFR. Therefore BB should be used with caution in severe or active reactive airway disease.17, 18
- Known II or III degree AV block – BB or CCB may cause II or III degree AV block in 15% of patients.15
- β 1 (80% cardiac β receptors) receptor stimulation
-
Non-dihydropyridine Calcium Channel Blocker19
- 4 classes of CCBs, but nondihydropyridines have the greatest affinity for myocardial calcium channels
- Mechanism: Impedes calcium influx and channel recovery in the myocardium
- Inhibitory effect on SA and AV nodal tissue
- Nondihydropyridines
- Diltiazem
- Verapamil
- More potent negative inotrope > more profound side effect of hypotension8
- Contraindications:
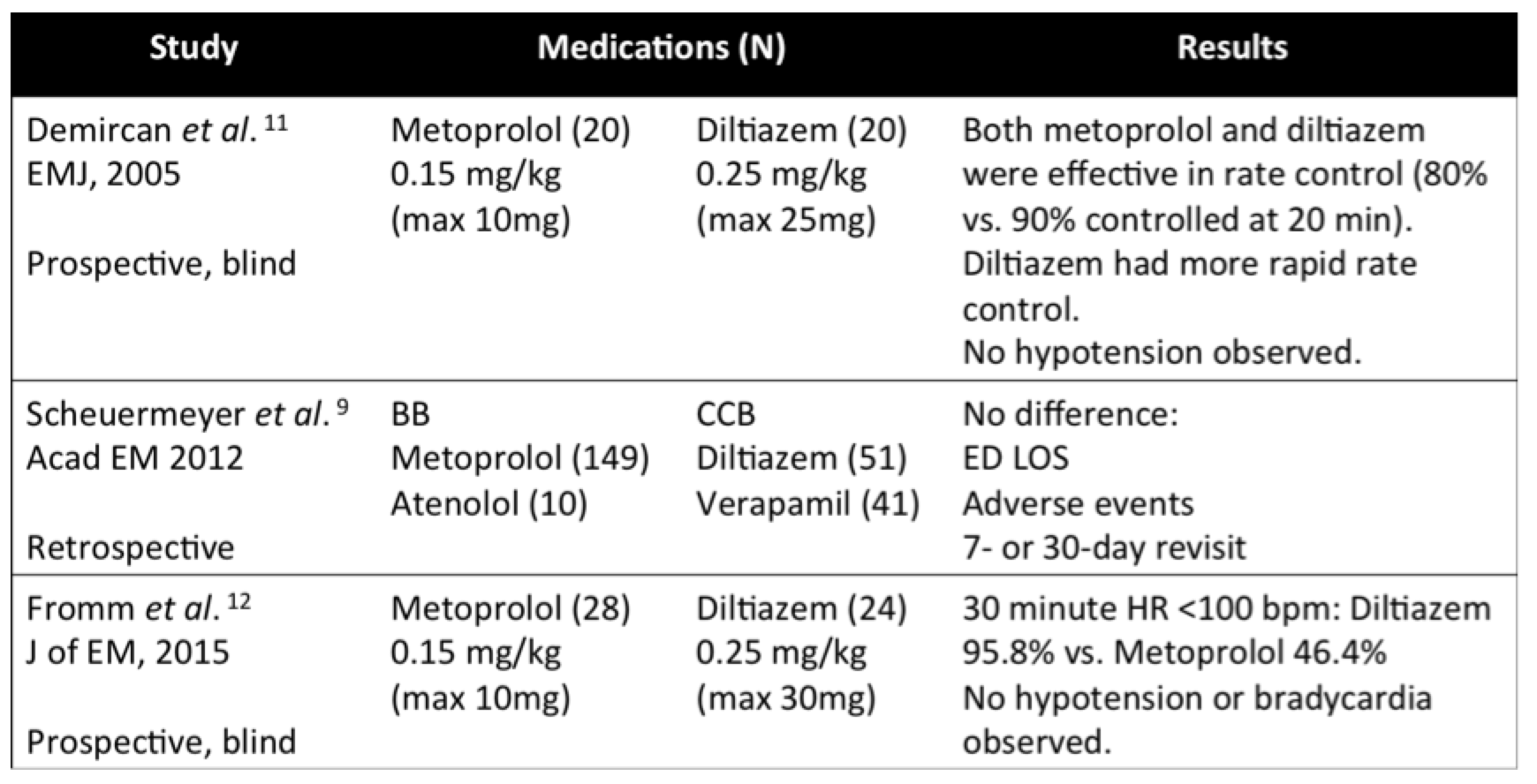
Metoprolol and diltiazem are the most commonly used BB and CCBs given their oral formulation and relative hemodynamic stability. There are two prospective studies directly comparing metoprolol and diltiazem. Fromm et al found diltiazem may provide superior rate control compared to metoprolol with no adverse events noted (no episodes of hypotension or bradycardia).12 It is important to note the inclusion/exclusion criteria of the studies.
- Inclusion: ventricular rate ≥120 bpm, SBP ≥90 mmHg
- Exclusion: SBP <90mmHg, ventricular rate ≥220 bpm, QRS >0.100s, 2nd or 3rd AV block, STEMI, NYHA Class IV HF, active wheezing with history of asthma/COPD, anemia (hemoglobin <11 g/dL), pregnancy.
=>Amiodarone:
DO consider amiodarone in critically ill patients. DON’T use amiodarone in AF >48 h or unknown duration without anticoagulation.
In cases where BB or CCB fail to reduce the heart rate or induce hypotension, amiodarone may be a reasonable option. Although amiodarone is an anti-arrhythmic, it has AV nodal blocking properties. An AHA class IIa recommendation states amiodarone can be used for rate control in critically ill patients.4 (Three studies provide the basis for this recommendation6, 22, 23)
- Class III antiarrhythmic
- Use in chemical cardioversion
- Sodium and potassium channel blocking properties
- β -blocking and calcium channel blocking properties => slows conduction through the AV node.
- Considerations: Amiodarone is an anti-arrhythmic, therefore in cases of AF or flutter >48h of unknown duration there is a possibility of cardioversion and risk of stroke.
- Pulmonary, hepatic, and thyroid toxicity
Clemo et al studied amiodarone for acute rate control in 33 ICU patients with hemodynamically destabilizing atrial tachycardia. This retrospective chart review targeted a cohort who failed conventional therapy including BB, CCB, digoxin, electrical cardioversion, and procainamide pharmacologic cardioversion. Amiodarone therapy was associated with a decrease in rate and increase in systolic blood pressure. Furthermore, there were no reported events of hypotension or bradycardia, possibly secondary to a lower loading dose of 2-3mg/kg. Of note, a significant amount of patients converted to sinus rhythm while on amiodarone infusion (29 at 24 hours, 20 at discharge).22
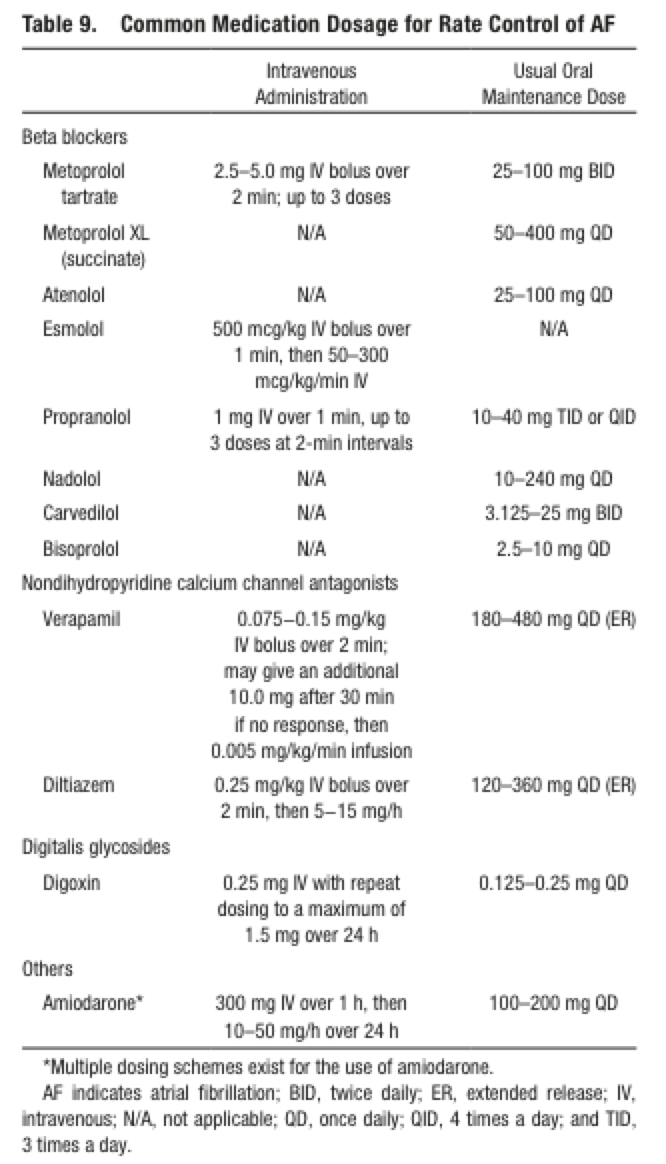
Table of Common Rate Control Agents via AHA/ACC/HRS Guidelines4
=>Goals of Rate Control: DO aim for ventricular rate less than 110 bpm.
Earlier guidelines recommend the goal heart rate to be less than 80 bpm. RACE II provided the basis for a lenient rate-control strategy by investigating a resting heart rate <110 bpm versus <80 bpm. RACE II found lenient-control was non-inferior to strict-control for composite death from cardiovascular causes, hospitalization for heart failure, stroke, systemic embolism, major bleeding, arrhythmic events (syncope, sustained VT, cardiac arrest, life-threatening adverse effects of drugs, implantation of pacemaker or ICD). 24
- Asymptomatic/hemodynamically stable: <110 bpm
- Symptomatic: Rate to point of asymptomatic
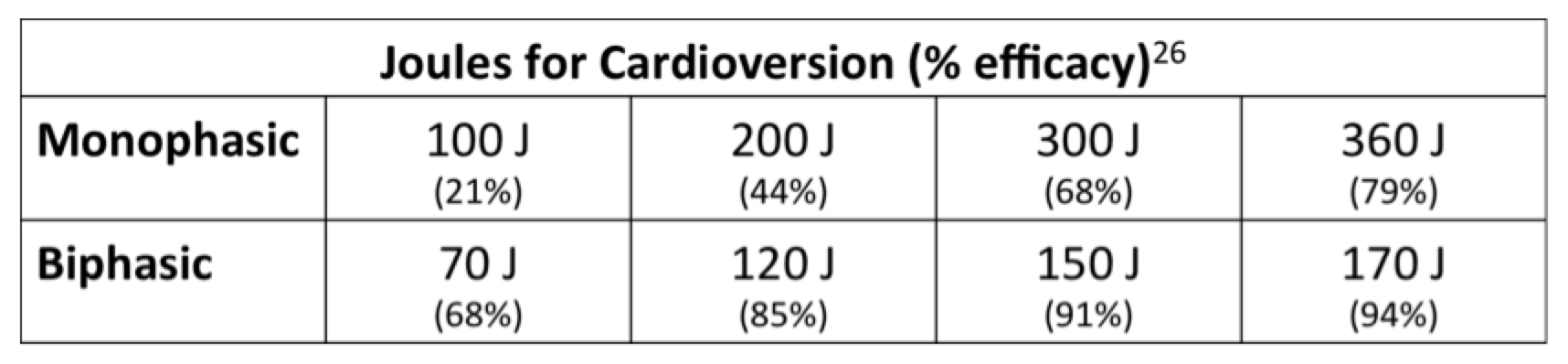
=>Electrical Cardioversion (Unstable AF): DO cardiovert unstable AF.
Patients with hemodynamic instability, ongoing ischemia, or worsening heart failure should undergo direct current cardioversion.4 If the choice is available, biphasic waveform devices have greater efficacy than monophasic.25, 26 In terms of the selection of energy level, Mittal et al provides a protocol for escalating shock energies on monophasic and biphasic devices with reported efficacy of each energy level.26 Some advocate starting at maximum energy to optimize success as studies have shown higher energy does not increase cardiac injury.27, 28
In regards to pad placement, a systematic review by Kirkland et al found no difference in anterolateral (right parasternal-left midaxillary) and anteroposterior (right parasternal-left infrascapular) pad placement in the success of cardioversion. However, a subgroup analysis indicated anterolateral placement might be more effective when using biphasic shocks.29
Managing Atrial Fibrillation Secondary to…
=>Sepsis: Do use BBs
AF is an independent predictor of mortality the critically ill, AF confers 31% mortality versus patients without AF at 17% mortality (P<0.001).30 A retrospective cohort by Walkey et al of 39,693 septic patients with AF analyzed practice patterns and mortality. CCBs were most commonly initiated in AF during sepsis (36%); however, BBs were associated with lower hospital mortality compared to CCB (RR 0.92), digoxin (R 0.79), and amiodarone (RR 0.64).31
=>Hyperthyroid: Do use BBs
BBs are recommended to control AF complicating thyrotoxicosis unless contraindicated (Level C).4 The rationale is two-fold, first hyperthyroidism is a state of increased β -adrenergic receptors thus BB reduce symptoms.32 Second, propranolol, atenolol, and metoprolol slowly decrease serum T3 concentrations by inhibiting the conversion from thyroxine (T4).33, 34
=>Heart Failure: Do use BBs
The AF-CHF study by Dydra et al compared rate versus rhythm control strategies in CHF. The study enrolled 1,376 patients with an EF <35% and recent history of AF, patients were randomized to rate control utilizing BB or rhythm control utilizing electrical cardioversion and amiodarone. Rhythm control was abandoned more frequently than rate control, 21% versus 9.1% respectively. The predominant reason to abandon rate control was worsening heart failure. Importantly, crossover from rhythm to rate control did not increase cardiovascular or all cause mortality.35 Although rate control is an acceptable strategy in CHF, BB therapy does not confer the same mortality benefit in AF as it does in sinus rhythm.36 Therefore, BB can be used in HF but does not need to be the only or first line agent.
The decrease in SVR, anti-ischemic effects, and LV relaxation of CCBs indicate theoretical benefit in CHF. However, the negative inotropic effect may impair left ventricular function.37 Furthermore, the MDPIT study by Goldstein et al showed post-MI patients on CCBs with early LV dysfunction (EF <40%) were found to have increased late onset heart failure.21 Although the evidence is not overwhelming, in cases of rapid AF and CHF, particularly decompensated HF, rate control with CCBs can be detrimental.
Briefly on Antithrombotic Therapy: DO anticoagulate.4,38
Patients with AF greater than 48 hours or less than 48 hours but high risk of stroke and no contraindications for anticoagulation should initiate anticoagulation as soon as possible before or immediately after cardioversion.4
Nonvalvular
- Patients with nonvalvular AF, CHA2DS2-VASc is recommended for stroke risk assessment (Level B evidence).4
- CHA2DS2-VASc39
- Congestive Heart Failure
- Hypertension
- Age >75 (2 points)
- Diabetes mellitus
- Prior Stroke or TIA or Thromboembolism (2 points)
- Vascular disease – prior MI, PAD, aortic plaque
- Age 65 to 74 years
- Female Sex
- Scoring (% risk of stroke/year)
- 0 No therapy (0%/year)
- 1 Aspirin 325mg or oral anticoagulants (1.3%/year)
- ≥2 Oral Anticoagulants recommended (2.2%/year)
- Warfarin, Dabigatran, Rivaroxaban, Apixaban
- Anticoagulants
- Renal function should be assessed in NOACs (Direct thrombin or factor Xa inhibitors)
Valvular
- Valve replacement – anticoagulation with warfarin INR 2 to 3 or 2.5 to 3.5 depending on tissue versus mechanical valve selection
Summary
-
Do
- Reverse/treat any underlying process (remember PIRATES)
- Use β1-selective BBs or non-dihydropyridine CCBs in rapid AF
- Use BB in patients with concurrent hyperthyroid
- Use CHA2DS2-VASc to risk stratify for stroke
-
Don’t
- Mix BB and CCB (if possible)
- Use a BB in severe asthma
- Use a CCB in decompensated HF
- Cardiovert stable AF with duration >48h or unknown duration if the patient isn’t on anticoagulation
References / Further Reading
- Hagens VE, Van Gelder IC, Crijns HJ, Group RACVECOPAFS. The RACE study in perspective of randomized studies on management of persistent atrial fibrillation. Cardiac electrophysiology review. 2003;7(2):118-121.
- Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. The New England journal of medicine. 2002;347(23):1834-1840.
- Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. The New England journal of medicine. 2002;347(23):1825-1833.
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr., et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):2071-2104.
- Abrams J, Allen J, Allin D, Anderson J, Anderson S, Blanski L, et al. Efficacy and safety of esmolol vs propranolol in the treatment of supraventricular tachyarrhythmias: a multicenter double-blind clinical trial. American heart journal. 1985;110(5):913-922.
- Delle Karth G, Geppert A, Neunteufl T, Priglinger U, Haumer M, Gschwandtner M, et al. Amiodarone versus diltiazem for rate control in critically ill patients with atrial tachyarrhythmias. Critical care medicine. 2001;29(6):1149-1153.
- Ellenbogen KA, Dias VC, Plumb VJ, Heywood JT, Mirvis DM. A placebo-controlled trial of continuous intravenous diltiazem infusion for 24-hour heart rate control during atrial fibrillation and atrial flutter: a multicenter study. Journal of the American College of Cardiology. 1991;18(4):891-897.
- Platia EV, Michelson EL, Porterfield JK, Das G. Esmolol versus verapamil in the acute treatment of atrial fibrillation or atrial flutter. The American journal of cardiology. 1989;63(13):925-929.
- Scheuermeyer FX, Grafstein E, Stenstrom R, Christenson J, Heslop C, Heilbron B, et al. Safety and efficiency of calcium channel blockers versus beta-blockers for rate control in patients with atrial fibrillation and no acute underlying medical illness. Academic emergency medicine: official journal of the Society for Academic Emergency Medicine. 2013;20(3):222-230.
- Siu CW, Lau CP, Lee WL, Lam KF, Tse HF. Intravenous diltiazem is superior to intravenous amiodarone or digoxin for achieving ventricular rate control in patients with acute uncomplicated atrial fibrillation. Critical care medicine. 2009;37(7):2174-2179; quiz 2180.
- Demircan C, Cikriklar HI, Engindeniz Z, Cebicci H, Atar N, Guler V, et al. Comparison of the effectiveness of intravenous diltiazem and metoprolol in the management of rapid ventricular rate in atrial fibrillation. Emergency medicine journal: EMJ. 2005;22(6):411-414.
- Fromm C, Suau SJ, Cohen V, Likourezos A, Jellinek-Cohen S, Rose J, et al. Diltiazem vs. Metoprolol in the Management of Atrial Fibrillation or Flutter with Rapid Ventricular Rate in the Emergency Department. The Journal of emergency medicine. 2015;49(2):175-182.
- Bailey DG, Carruthers SG. Interaction between oral verapamil and beta-blockers during submaximal exercise: relevance of ancillary properties. Clinical pharmacology and therapeutics. 1991;49(4):370-376.
- Johnston DL, Lesoway R, Humen DP, Kostuk WJ. Clinical and hemodynamic evaluation of propranolol in combination with verapamil, nifedipine and diltiazem in exertional angina pectoris: a placebo-controlled, double-blind, randomized, crossover study. The American journal of cardiology. 1985;55(6):680-687.
- Zeltser D, Justo D, Halkin A, Rosso R, Ish-Shalom M, Hochenberg M, et al. Drug-induced atrioventricular block: prognosis after discontinuation of the culprit drug. Journal of the American College of Cardiology. 2004;44(1):105-108.
- Brubacher JR. Beta-Adrenergic Antagonists. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR, editors. Goldfrank’s Toxicologic Emergencies. 10e ed. New York, NY: McGraw-Hill; 2015.
- Greefhorst AP, van Herwaarden CL. Comparative study of the ventilatory effects of three beta 1-selective blocking agents in asthmatic patients. European journal of clinical pharmacology. 1981;20(6):417-421.
- Self TH, Wallace JL, Soberman JE. Cardioselective beta-blocker treatment of hypertension in patients with asthma: when do benefits outweigh risks? The Journal of asthma : official journal of the Association for the Care of Asthma. 2012;49(9):947-951.
- Jang DH, DeRoos F. Calcium Channel Blockers. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR, editors. Goldfrank’s Toxicologic Emergencies. 10e ed. New York, NY: McGraw-Hill; 2015.
- Materne P, Legrand V, Vandormael M, Collignon P, Kulbertus HE. Hemodynamic effects of intravenous diltiazem with impaired left ventricular function. The American journal of cardiology. 1984;54(7):733-737.
- Goldstein RE, Boccuzzi SJ, Cruess D, Nattel S. Diltiazem increases late-onset congestive heart failure in postinfarction patients with early reduction in ejection fraction. The Adverse Experience Committee; and the Multicenter Diltiazem Postinfarction Research Group. Circulation. 1991;83(1):52-60.
- Clemo HF, Wood MA, Gilligan DM, Ellenbogen KA. Intravenous amiodarone for acute heart rate control in the critically ill patient with atrial tachyarrhythmias. The American journal of cardiology. 1998;81(5):594-598.
- Hou ZY, Chang MS, Chen CY, Tu MS, Lin SL, Chiang HT, et al. Acute treatment of recent-onset atrial fibrillation and flutter with a tailored dosing regimen of intravenous amiodarone. A randomized, digoxin-controlled study. European heart journal. 1995;16(4):521-528.
- Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, et al. Lenient versus strict rate control in patients with atrial fibrillation. The New England journal of medicine. 2010;362(15):1363-1373.
- Bardy GH, Ivey TD, Allen MD, Johnson G, Mehra R, Greene HL. A prospective randomized evaluation of biphasic versus monophasic waveform pulses on defibrillation efficacy in humans. Journal of the American College of Cardiology. 1989;14(3):728-733.
- Mittal S, Ayati S, Stein KM, Schwartzman D, Cavlovich D, Tchou PJ, et al. Transthoracic cardioversion of atrial fibrillation: comparison of rectilinear biphasic versus damped sine wave monophasic shocks. Circulation. 2000;101(11):1282-1287.
- Grubb NR, Cuthbert D, Cawood P, Flapan AD, Fox KA. Effect of DC shock on serum levels of total creatine kinase, MB-creatine kinase mass and troponin T. Resuscitation. 1998;36(3):193-199.
- Rao AC, Naeem N, John C, Collinson PO, Canepa-Anson R, Joseph SP. Direct current cardioversion does not cause cardiac damage: evidence from cardiac troponin T estimation. Heart. 1998;80(3):229-230.
- Kirkland S, Stiell I, AlShawabkeh T, Campbell S, Dickinson G, Rowe BH. The efficacy of pad placement for electrical cardioversion of atrial fibrillation/flutter: a systematic review. Academic emergency medicine: official journal of the Society for Academic Emergency Medicine. 2014;21(7):717-726.
- Shaver CM, Chen W, Janz DR, May AK, Darbar D, Bernard GR, et al. Atrial Fibrillation Is an Independent Predictor of Mortality in Critically Ill Patients. Critical care medicine. 2015;43(10):2104-2111.
- Walkey AJ, Evans SR, Winter MR, Benjamin EJ. Practice patterns and outcomes of treatments for atrial fibrillation during sepsis: A propensity-matched cohort study. Chest. 2015.
- Bilezikian JP, Loeb JN. The influence of hyperthyroidism and hypothyroidism on alpha- and beta-adrenergic receptor systems and adrenergic responsiveness. Endocrine reviews. 1983;4(4):378-388.
- Perrild H, Hansen JM, Skovsted L, Christensen LK. Different effects of propranolol, alprenolol, sotalol, atenolol and metoprolol on serum T3 and serum rT3 in hyperthyroidism. Clinical endocrinology. 1983;18(2):139-142.
- Wiersinga WM, Touber JL. The influence of beta-adrenoceptor blocking agents on plasma thyroxine and triiodothyronine. The Journal of clinical endocrinology and metabolism. 1977;45(2):293-298.
- Dyrda K, Roy D, Leduc H, Talajic M, Stevenson LW, Guerra PG, et al. Treatment Failure With Rhythm and Rate Control Strategies in Patients With Atrial Fibrillation and Congestive Heart Failure: An AF-CHF Substudy. Journal of cardiovascular electrophysiology. 2015.
- Kotecha D, Holmes J, Krum H, Altman DG, Manzano L, Cleland JG, et al. Efficacy of beta blockers in patients with heart failure plus atrial fibrillation: an individual-patient data meta-analysis. Lancet. 2014;384(9961):2235-2243.
- Elkayam U. Calcium channel blockers in heart failure. Cardiology. 1998;89 Suppl 1:38-46.
- Moukabary T, Gonzalez MD. Management of atrial fibrillation. The Medical clinics of North America. 2015;99(4):781-794.
- Mason PK, Lake DE, DiMarco JP, Ferguson JD, Mangrum JM, Bilchick K, et al. Impact of the CHA2DS2-VASc score on anticoagulation recommendations for atrial fibrillation. The American journal of medicine. 2012;125(6):603 e601-606.






8 thoughts on “Management of Atrial Fibrillation: Do’s and Don’ts”
And what about digoxin ? in this article ( => http://www.healio.com/cardiology/learn-the-heart/blogs/hyperthyroid-induced-atrial-fibrillation ), we are told not to give BB but digoxin for EF < 50%
Great point! I included the AHA table of rate control agents specifically because it included digoxin. Beta-blockers are an option in compensated heart failure, however per the AHA there is level C evidence against BB/CCB in decompensated HF. Digoxin is an option in decompensated heart failure but the time to effect can be longer and some studies indicate long term digoxin therapy is associated with increased all-cause mortality (PMID: 26717399, 27064796). In the stable (not immediately requiring electrical cardioversion) patient, it is reasonable to discuss/consult with our cardiology colleagues regarding the use of digoxin or other agents.
Pingback: Länkar v17-19 | Internmedicin
Thank you. good details.
Pingback: Förmaksflimmer akut- Översikt – Mind palace of an ER doc
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Atrial Fibrillation - emDOCs.net - Emergency Medicine Education
Pingback: Case Conference Summary, August 16, 2017 | AMP EM
Pingback: Revisiting AF with Heart Failure: Time To Let Go Digoxin – edhsredu