Author: Natalie Sciano, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD(@long_brit, EM Physician at SAUSHEC, USAF)
A woman of reproductive age walks into your Emergency Department with nausea and vomiting. The differential is already broad, but what if she is pregnant? Yes, this may just be “morning sickness”, which can occur in up to 75% of pregnant women.1-3 But hey, we’re Emergency Physicians; what else could it be?
We should take into account the whole picture of the patient in front of us including their age, parity, gestational age, body habitus, and ethnicity. If nausea and vomiting have developed after 10 weeks we need to think of non-pregnancy related causes as well. If symptoms occur in the first trimester of pregnancy think of gestational trophoblastic disease (GTD), hyperemesis gravidarum, and multiple gestations. If symptoms occur late in pregnancy our differential should include preeclampsia, HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets), and acute fatty liver of pregnancy (AFLP).
Case Scenario
A 24 year-old G1P0A0 37 weeks by LMP presents to your ED with nausea and vomiting x1 day. She is complaining of mild right upper quadrant abdominal pain. Her pregnancy has been uneventful. Her vitals at T 98.7, HR 130, BP 105/75, RR 24, O2 99% on room air.
HELLP Syndrome and Preeclampsia
HELLP stands for hemolysis, elevated liver enzymes, and low platelets. It develops in roughly 1% of pregnancies overall and in 10-20% of cases with preeclampsia.4-5 Risk factors include history of HELLP or preeclampsia in a previous pregnancy and a family history of HELLP syndrome. For a woman to have HELLP syndrome she must have evidence of the following:6
- Thrombocytopenia (< 100K)
- Liver injury (AST ≥ 70, Total Bilirubin ≥ 1.2)
- Hemolysis which can include schistocytes on blood smear, low haptoglobin, or an elevated indirect bilirubin
Women with HELLP typically have worse outcomes when compared to women with preeclampsia alone. Outcomes can include eclampsia, preterm birth, perinatal mortality, pulmonary edema, subcapsular liver hematoma, and placental abruption. In a 2012 review including 180 pregnant women with hepatic hematoma or rupture, 90% had HELLP syndrome.5 So late in pregnancy, remember that blood in the abdomen may not be from a ruptured uterus, but from a ruptured hepatic hematoma. Hemorrhagic shock management requires resuscitation and consultation with obstetrics, surgery, and potentially interventional radiology.
Preeclampsia is gestational hypertension (≥ 140/90 mm Hg) with associated end organ damage which could include thrombocytopenia, kidney injury (>1.1 creatinine or 2x baseline), liver injury, pulmonary edema, and mental status changes. Risk factors include young maternal age, nulliparity (3-10%), obesity, multigestation pregnancy, previous pre-eclampsia, metabolic syndrome, and being African American (11%).1
 If the patient develops vision changes such as scotomata (pictured to the right),7 RUQ pain, or thrombocytopenia, it should be a warning sign for possible progression to eclampsia.
If the patient develops vision changes such as scotomata (pictured to the right),7 RUQ pain, or thrombocytopenia, it should be a warning sign for possible progression to eclampsia.
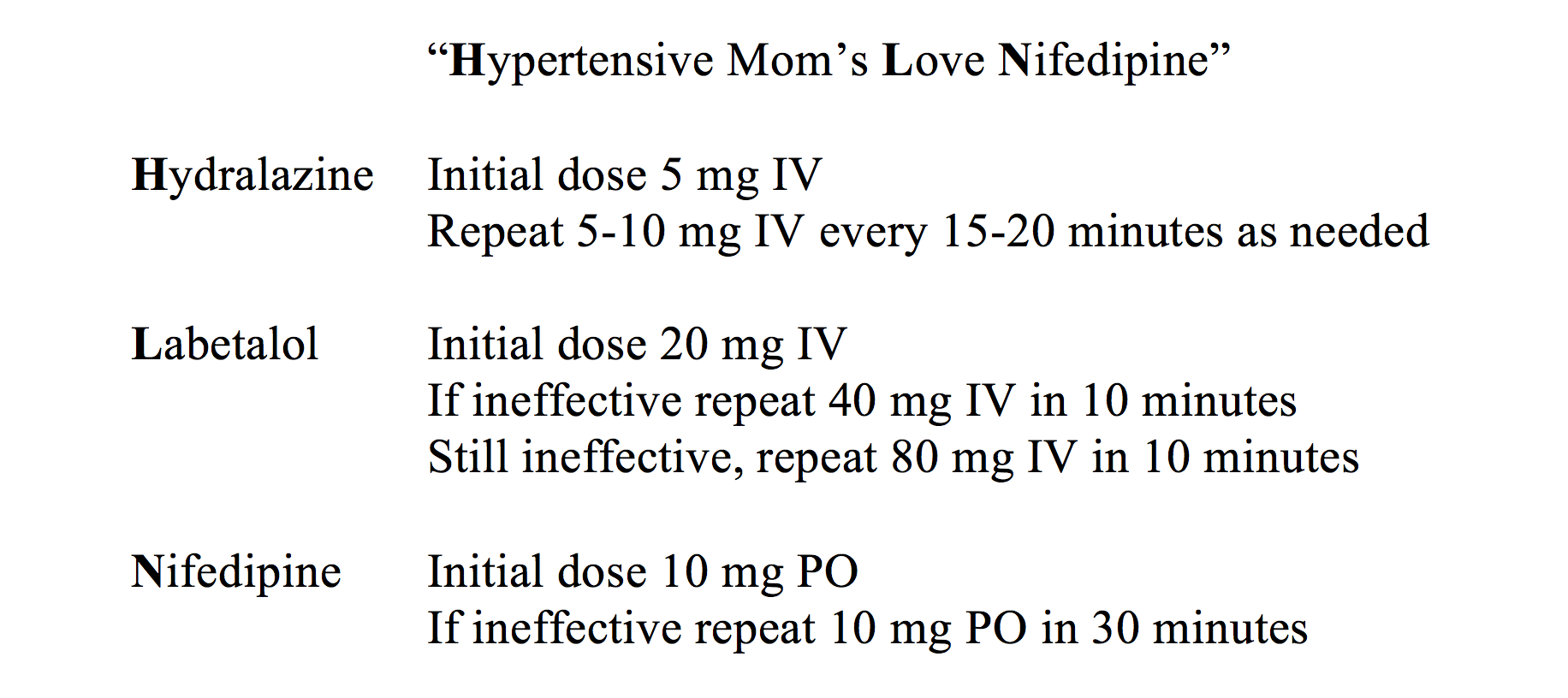
There continues to be varying opinions if HELLP is a severe form of preeclampsia or its own entity. Nonetheless, patients in HELLP who also present with hypertension must be managed due to the risk of developing congestive heart failure, placental abruption, cerebral hemorrhage, and hypertensive encephalopathy. Three drugs have become the mainstay of hypertensive treatment in HELLP or preeclampsia with the blood pressure goal of <160/110 mm Hg. Their dosing regimens are discussed below.1
Magnesium is also empirically started on these patients due to the risk of progression to eclampsia. A magnesium regimen is discussed below.1,8
- 4-6 grams loading dose of Mg sulfate diluted in 100 ml of IV fluid over 15-20 minutes
- Start 1-2g/hr in 100 mL of IV fluid as maintenance
- An additional 2g dose may be administered for recurrent seizures
- Barbiturates may be added if seizures continue
- Magnesium is discontinued 24 hours post delivery
Intramuscular (IM) administration is possible, but still requires a 4 g IV loading dose and then alternating IM buttock injections q4hours with an IV maintenance infusion. This seems more cumbersome than the above regimen.
Magnesium toxicity (>10 mEq/L) can develop and can be recognized by:
- Decreased patellar reflexes
- Decreased respiratory drive or paralysis
- Decreased mental status
To reverse Mg toxicity give 1 g IV calcium gluconate or calcium chloride, in addition to stopping the Mg infusion.1,8
Acute Fatty Liver of Pregnancy (AFLP)
Acute fatty liver of pregnancy occurs in 1 in 10,000 pregnancies and presents nearly always late in pregnancy. Fat vesicles accumulate within hepatocytes to the point the liver is unable to function. Unrelenting nausea and vomiting are common complaints, but some women may have confounding signs of preeclampsia such as hypertension, proteinuria, and edema.1,4
Laboratory findings may be helpful in differentiating the two. For example, in comparing the laboratory results of different studies, AFLP was more likely to have elevated bilirubin (mean of 11 mg/dl in AFLP4 vs 1.5 mg/dl in HELLP4,6), hypofibrinogenemia (mean of 105 mg/dl and 136 mg/dl in AFLP1,4 vs 480 mg/dl in HELLP),4 hypoglycemia, and ascites (30% of patients in AFLP4 vs 6.6% and 8% HELLP).4,6 If a coagulopathy develops, cryoprecipitate, platelets, and/or fresh-frozen plasma are often necessary.1,9-10 Hypoglycemia can be treated with an amp of D50 (50% dextrose 50 mL IV) as needed or dextrose infusion with 10% dextrose as indicated.9-10 Hepatic failure resolves after delivery so prompt consultation with obstetrics and immediate delivery is warranted.
Disseminated Intravascular Coagulation (DIC) Management:9-10
- Treat underlying disease, IV resuscitation, PRBCs, inotrope
- Cryoprecipitate with hypofibrinogenemia and active bleeding – goal to raise fibrinogen to 100-150
- Platelets transfuse if < 20K
- FFP if bleeding persists
- Vitamin K
HELLP syndrome and AFLP at first glance may be difficult to differentiate. AFLP patients more often present with malaise, nausea and vomiting, abdominal pain, and jaundice. Jaundice is uncommon in HELLP. Again, hypoglycemia, elevated bilirubin, hypofibrinogenemia, ascites, and encephalopathy are more common in AFLP.1,4
Gestational trophoblastic disease (GTD)
GTD can be divided into hydatidiform moles or non-molar trophoblastic neoplasms. Hydatidiform moles can be complete, partial, or invasive. Non-molar trophoblastic neoplasms include choriocarcinoma, placental site tumor, and epithelioid tumor.
Complete moles are completely abnormal, usually 46 XX with only paternal chromosomes. They appear as a mass of vesicles or a “grape-like” structure. Partial moles are partial fetuses and will contain some fetal parts. They are usually 69 XXY, 69 XXX due to fertilization of one egg by two sperm.
Risk factors include prior molar pregnancies and extremes of reproductive age. The incidence is about 1-2 in 1,000 deliveries. Molar pregnancies are more common in Asians, Hispanics, and American Indians.1
Symptoms are more pronounced with complete moles, and in addition to hyperemesis can include vaginal bleeding, enlarged uterus, and elevated β-hCG for gestational age. β-hCG can sometimes be in the millions predisposing to preeclampsia and eclampsia. Think of molar pregnancy when you see preeclamptic or eclamptic symptoms in early gestation. Partial moles have β-hCG concentrations more within normal gestational ranges.
Ultrasound of a complete mole is classically described as a “snowstorm” (A in picture below). A partial mole via ultrasound will show thickened, multi-cystic placenta with some fetal tissue (B in picture below). Dilation and curettage is the treatment of choice. Surveillance is recommended with serial β-hCG post evacuation due to the risk of trophoblastic neoplasm after a molar pregnancy. Malignancy can occur in 15-20% of complete moles and 1-5% of partial moles. If a patient has a history of molar pregnancy that was lost to follow-up presents with nausea and vomiting, think about a trophoblastic neoplasm.1

Bloom S, Cunningham F, Spong CY et al. Williams Obstetrics 24/E. Figure 20-4. Digital image. Access Medicine. McGraw-Hill Education / Medical; 2014. Web.
What else could it be?
Nausea and vomiting beginning after 10 weeks may not be pregnancy related…
Due to the uterus, the appendix often moves out of the right lower quadrant so appendicitis can be difficult to differentiate during pregnancy. There is already a mild leukocytosis in pregnancy, so blood work may not be helpful. For diagnosis, compression ultrasonography is often unhelpful due to anatomical shifts. An appendiceal CT will limit radiation to the fetus, but do consider MR imaging instead if available. Appendectomy is the treatment of choice, and should not be delayed. There is up to a 10% risk of preterm labor associated with appendectomy.11 Of note, the fetal mortality rate is about 5%, and rises significantly to 30-35% if the appendix is perforated.11-12 With these thoughts in mind, diagnostic accuracy is imperative due to the risk to the fetus.
Cholecystitis occurs in 1 in 1,000 pregnancies. The incidence of gallstones and biliary sludge often increase in pregnancy due to doubling of the fasting and residual postprandial gallbladder volumes. Medical management may be an option; however, symptoms often recur in 25-50% of women.1 Surgical management is now favored. As was discussed with appendectomies, the later in pregnancy surgical intervention occurs, the more likely preterm labor or abortion can occur.
Pregnant women do not have an increased risk of bowel obstruction. The most common cause of small bowel obstruction is due to adhesions (60%) from previous surgeries such as C-sections or appendectomies. Another 25% of obstructions in pregnancy are due to volvulus of the sigmoid, cecal, or small bowel. Obstruction most commonly presents in the 1st and 2nd trimester. Nearly 98% have abdominal pain, and 80% have nausea and vomiting.1 CT and MR imaging are preferred over radiographs. At baseline, there is a childhood cancer risk of 0.3%. If the fetus is exposed to <5 RADS, the risk is 0.3-1%. A CT scan is less than 5 RADS and help you identify several important diagnoses.13
The β-hCG structure can mimic the TSH molecule causing “transient thyrotoxicosis of hyperemesis”. Clinically the patient will lack classic signs of hyperthyroidism such as a goiter, ophthalmopathy, heat intolerance, tremor, or muscle weakness. However, if present, testing hormone function may be necessary. Transient thyrotoxicosis of pregnancy will resolve without treatment.
In the end, this may simply be nausea and vomiting of pregnancy, or the lay term “morning sickness”. This has a mean onset of 5-6 weeks, often peaks at 9 weeks, and over 90% will receive relief by 22 weeks. However, complete relief of symptoms rarely occurs. These patients will generally have normal vitals and labs. Prenatal vitamins if initiated 3 months prior to conception may decrease nausea and vomiting in pregnancy. Daily Vitamin B6 (10 mg) with doxylamine (10 mg) is the first line pharmacotherapy treatment.3 Other recommendations for these patients may include eating smaller more frequent meals, ginger extract, anticholinergics, antihistamines, ondansetron, and metoclopramide.13-14
In more severe cases, women may develop hyperemesis gravidarum that may result in dehydration (>5% weight loss), orthostatic hypotension, starvation ketosis with ketonuria, elevated specific gravity and BUN, and a hypochloremic hypokalemic metabolic alkalosis.1,3,15 It is recommended to replete with thiamine if significant electrolyte abnormalities exist to protect against Wernicke’s. In addition to the above regimen, corticosteroids may be helpful. Methylprednisolone 16 mg TID with a 2 week taper may decrease hospitalization rates and readmissions.3 If no prior ultrasounds exist, obtain one to make sure hyperemesis is not due to a molar pregnancy. Risk factors for hyperemesis gravidarum include young maternal age, history of acid reflux, multiple gestations, obesity, and nulliparity.1,3, 15 Be aware of the risk of prolonged QT in some antiemetic medications mentioned above, like ondansetron, when administering to potentially hypokalemic or hypomagnesemic patients.3
Key Points
- Take into account the whole picture including parity, age, gestational age, and previous pregnancy complications.
- Nausea and vomiting in early pregnancy think molar pregnancy, multiple gestations, and hyperemesis gravidarum. Replete thiamine in hyperemesis.
- Obtain an ultrasound if there is no documentation of one previously.
- Nausea and vomiting late in pregnancy think of HELLP, AFLP, and preeclampsia.
- Check your sixth vital sign: Glucose. This may help differentiate AFLP from HELLP.
- Onset of nausea and vomiting after 10 weeks may be non-pregnancy related.
- Remember “Hypertensive Mom’s Love Nifedipine”
- Magnesium 4-6 grams in 15-20 minutes, followed by maintenance infusion of 1-2 grams/hour.
References / Further Reading:
- Bloom S, Cunningham F, Spong CY et al. Williams Obstetrics 24/E. McGraw-Hill Education / Medical; 2014
- Mylonas, Ioannis, Andrea Gingelmaier, and Franz Kainer. “Nausea and Vomiting in Pregnancy.” Dtsch Arztebl 104.25 (2007): 1821-826. Web.
- Practice Bulletin No. 153: Nausea and Vomiting of Pregnancy. Obstet Gynecol. 2015;126(3):e12-24.
- Vigil-de Gracia P. Acute fatty liver and HELLP syndrome: two distinct pregnancy disorders. Int J Gynaecol Obstet. 2001;73(3):215-20.
- Vigil-De Gracia P, Ortega-Paz L: Pre-eclampsia/eclampsia and hepatic rupture. Int J Gynaecol Obstet 118(3):186, 2012
- Sibai BM, Ramadan MK, Usta I, et al. Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome). Am J Obstet Gynecol 1993; 169:1000.
- Digital image. Vecto2000. 29 Jan. 2013. Web. <http://vecto2000.com/free-vector-cute-cartoon-landscape-vector/>.
- Lu JF, Nightingale CH. Magnesium sulfate in eclampsia and pre-eclampsia: pharmacokinetic principles. Clin Pharmacokinet. 2000;38(4):305-14.
- Tintinalli JE, Cline D, Ma OJ et al. Tintinalli’s Emergency Medicine Manual 7/E. McGraw Hill Professional; 2012.
- Marx JA, Hockberger R, Walls RM. Rosen’s Emergency Medicine, Concepts and Clinical Practice. Saunders; 2013.
- Brunicardi FC, Andersen DK. Schwartz’s Principles of Surgery. McGraw Hill Professional; 2010.
- Hardin DM. Acute appendicitis: review and update. Am Fam Physician. 1999;60(7):2027-34.
- Williams PM, Fletcher S. Health effects of prenatal radiation exposure. Am Fam Physician. 2010;82(5):488-93.
- Quinla JD, Hill DA. Nausea and vomiting of pregnancy. Am Fam Physician. 2003;68(1):121-8.
- Mylonas, Ioannis, Andrea Gingelmaier, and Franz Kainer. “Nausea and Vomiting in Pregnancy.” Dtsch Arztebl 104.25 (2007): 1821-826. Web.





