
Author: Erica Simon, DO, MHA (@E_M_Simon – EM Resident Physician, SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, SAUSHEC EM, USAF)
It’s the middle of a busy night shift in your ED when the phone rings for a patient transfer:
Eighteen year-old female, pedestrian vs. semi at highway speeds. The patient was GCS 3 upon EMS arrival and intubated in the field with subsequent needle decompression secondary to a right-sided tension pneumothorax. Secondary survey revealed an unstable pelvis, bilateral open femur fractures, and an open left tibial fracture. A pelvic binder was placed and lower extremities splinted.
Upon arrival to the OSH VS: SBP 62, HR 81. A massive transfusion protocol was initiated with temporary stabilization, allowing for trauma pan-scan: CT head/C-spine: negative. CT abdomen / pelvis: grade III liver lac, grade IV splenic lac, concern for duodenal hematoma, pelvic ring fractures x6 with apparent blush near the left internal iliac vein. After imaging completion, the patient was taken to the OR, where she underwent damage control splenectomy and pelvic packing.
The patient has been out of the OR for 2 hours. SBP 122/98, HR 71, T 99.8; intubated and ventilated with RR 18, FiO2 70%, ABG with PaO2 96.1 and lactate of 9.7. Blood product total: 16 U PRBCs, 14 U FFP, 14 U apheresis platelets. The hospital’s only trauma surgeon was unable to arrange air transport due to weather. The patient will be transported to your ED by ground, ETA 1.5 hours.
As you hang up the phone you mentally detail the scenario that will unfold upon her arrival: trauma team activated, VS, ABCs, secondary survey. Your internal monologue is a flurry of questions: CT angiography if she’s persistently hypotensive? Pressor of choice? Antibiotics for her open fractures? Is there a trauma ICU bed to accept her?
If you’re like this physician, and abdominal compartment syndrome hasn’t crossed your mind, the following will hopefully shed some light on why it should.

Abdominal Compartment Syndrome (ACS) Defined
To define abdominal compartment syndrome, we need to address intra-abdominal pressure (IAP). As the name implies, IAP is a measurement of the pressure within the abdominal compartment. Although variability still exists in ACS literature, the World Society on Abdominal Compartment Syndrome’s (WSACS) consensus definitions are the most widely accepted. The WSACS cites an IAP of <5 mmHg as within normal limits.1 An IAP persistently elevated above 12mmHg is indicative of intra-abdominal hypertension (IAH), and per the WSACS, IAH (>20mmHg) with evidence of end organ dysfunction is known as abdominal compartment syndrome. 1,2,3
The WSACS identifies four classes of IAH, not discussed here. If you are interested in learning more, please see reference 1.
FYI: Today ACS in the setting of trauma has been further delineated into primary ACS and secondary ACS. Patients with primary ACS sustain direct abdominal or retroperitoneal trauma, and commonly present in shock states. These individuals require abbreviated laparotomy to control hemorrhage and address injuries. This is in contrast to persons who sustain no direct intra-abdominal or retroperitoneal trauma, yet due to their requirements for massive resuscitation, are at a significant risk of secondary ACS (pelvic fractures, penetrating chest injuries, etc.).4
Pathophysiology Review
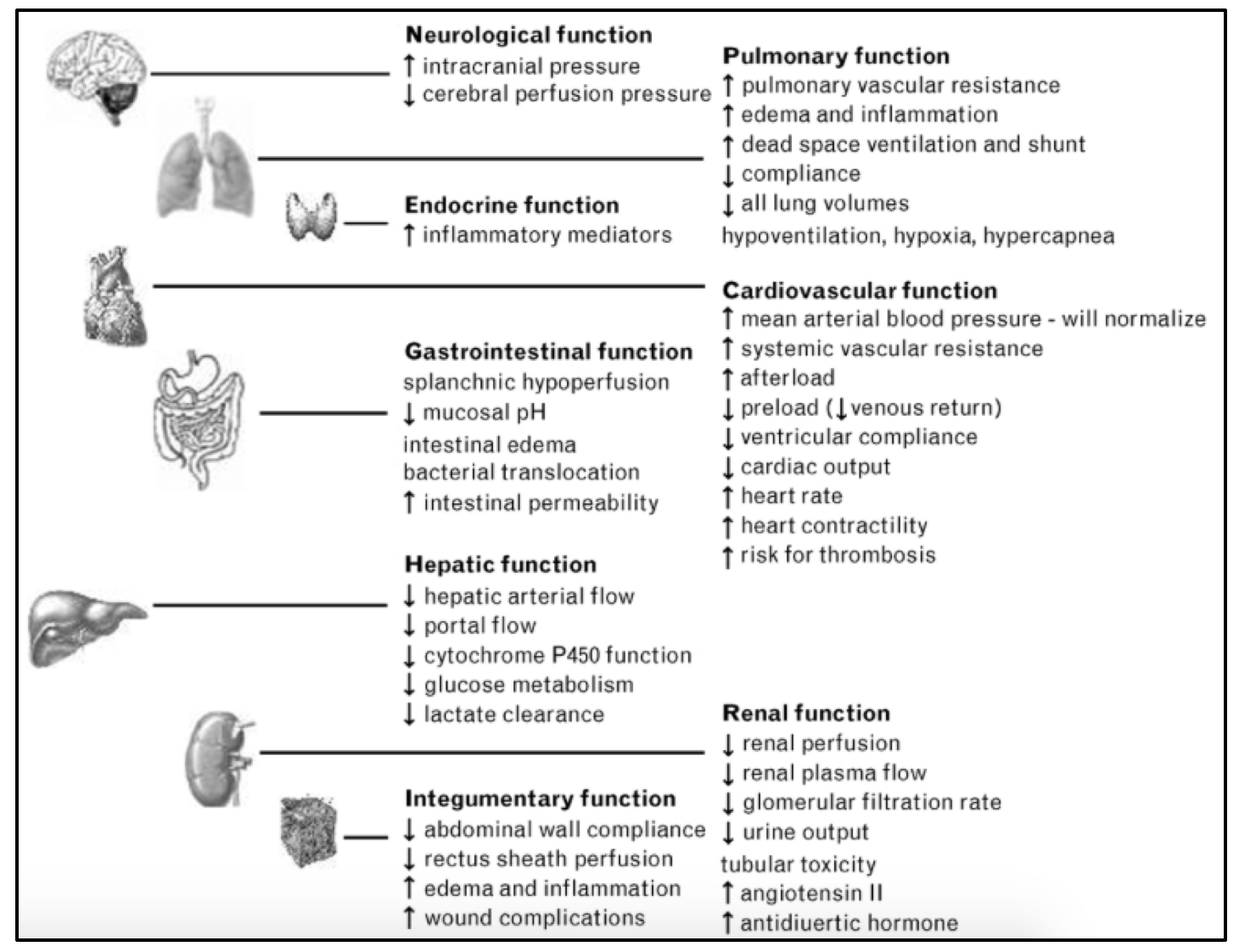
How does IAH/ACS result in systemic end organ dysfunction? Through direct transmission of intra-abdominal pressure:
- Brain: IAH transmits to the thoracic compartment => increased RA and SVC pressure => cerebral venous congestion.2,5
- CV: IAH raises the diaphragm => IVC compression => decreased preload (decreased stroke volume and reduced CO) => increased SVR which ultimately compromises perfusion.
- IAH also directly compresses the heart and increases RV afterload through increased pulmonary pressures => increased myocardial O2 demand and risk of ischemia. 2,5
- Pulm: IAH raises the diaphragm => decreased thoracic compliance => decreased FRC => worsening V/Q mismatch => poor oxygenation.2,5
- Hepatic: The liver is sensitive to small increases in IAP (IAH >10mmHg may result in hepatic dysfunction).6 Reduced hepatic arterial flow + compromised portal venous circulation => acute liver failure vs. exacerbation of chronic liver disease.2,5
- Renal: Presents as oliguria that progresses to anuria, despite fluid resuscitation. Increased IAP => renal parenchymal compression and decreased renal arterial flow, this + decreased CO addressed above => decreased renal perfusion and decreased GFR.
- Alterations in renal blood flow also lead to renin-angiotensin-aldosterone system activation => further increased renal vascular resistance. 2,5
- Abdominal wall: Decreased blood flow => ischemia and edema => reduced abdominal wall compliance => exacerbation of IAH/ACS.2,5
- Bowel: Decreased CO secondary to increased IAP => decreased splanchnic perfusion and increased splanchnic vascular resistance => bowel ischemia and infarct => bacterial translocation and the potential for sepsis.2,5
A figure from Rizoli et al.’s work includes the effects summarized above1:
Pearls:
- If a patient is intubated, decrease in pulmonary compliance secondary to ACS may result in the requirement for high inspiratory pressures in order to deliver desired tidal volumes.2 This is complicated by the fact that patients with ACS are at an increased risk of developing ARDS.5
- ACS causing a substantial decrease in SVR and increase in RV afterload is devastating in pre-load dependent states.2
Populations at Risk for ACS
The following chart is a compilation of the works of Harrison, et al., and Hong et al. (references 3 and 4), and offers a summary of the conditions which place individuals at risk for abdominal compartment syndrome:
| Decr Abdominal Compliance | Incr Intraluminal Contents | Capillary Leak/Fluid Resuscitation | Abdominal Collections |
| Abdominal Wall Trauma | Paralytic Ileus After Trauma, | Shock (Tissue Ischemia) | Hemoperitoneum |
| (Open or Blunt) | Pancreatitis, or Sepsis | Acidosis | Pneumoperitoneum |
| Pneumoperitoneum | Gastroparesis | Hypothermia | Urine/Ascitic Fluids |
| S/P Repair of Ventral Hernias | Colonic Pseudo-Obstruction | Major Transfusion or Transfusion Reaction | Sepsis |
| Recent Abdominal Surgery | Retroperitoneal Hematoma | Severe Burns | Pancreatitis |
The more you know:
IAH and ACS are not adult-only conditions. Case reports cite ACS and subsequent multi-organ failure (MOF), occurring in the pediatric population s/p blunt abdominal trauma. 5
Mortality and ACS
Numerous prospective and retrospective studies have detailed a high incidence of mortality and multi-organ failure in the ACS population.6 Post-injury ACS has been consistently reported as possessing a mortality rate ranging from 25-75% (variability likely secondary to differences in IAH/ACS definitions).7 The following chart depicts prominent ACS prospective and retrospective studies. While not intended to be a comprehensive review of ACS literature, these works highlight the importance of ACS evaluation. As depicted below; definitive management of ACS is abdominal decompression.2,6,8
| Study Author | Methods | Results | Conclusions |
| Prospective Studies | |||
| Balogh, et al. 20038 | 188 torso trauma patients, presenting to a Level I trauma center in Houston, TX, underwent standardized resuscitation. Prospective data collected: occurrence of ACS, demographics, ISS, urinary bladder pressure, gastric tonometry (GAPCO2), laboratory, respiratory, and hemodynamic data. With 1° and 2° ACS as endpoints. Variables tested by uni- and multivariate logistic analysis (MLA). | 26 Patients (14%) developed ACS – 11 (6%) were 1° ACS and 15 (8%) 2° ACS. 1° and 2° ACS had similar demographics, shock, and injury severity. Significant univariate differences included: time to decompression from ICU admit (600 ± 112 vs. 360 ± 48 min), Emergency Department (ED) crystalloid (4 ± 1 vs. 7 ± 1 L), pre-ICU crystalloid (8 ± 1 vs. 12 ± 1L), ED blood administration (2 ± 1 vs. 6 ± 1 U), GAPCO2 (24 ± 3 vs. 36 ± 3 mmHg), requiring pelvic embolization (9 vs. 47%), and emergency operation (82% vs. 40%). Early predictors identified by MLA of 1° ACS included hemoglobin concentration, GAPCO2, temperature, and base deficit; and for 2° ACS they included crystalloid, urinary output, and GAPCO2. | ACS patients display higher rates of organ failure and death as compared to their non-ACS counterparts: multiple organ failure (55% vs. 53% vs. 12%), and mortality (64% vs. 53% vs. 17%). |
| Hong, et al. 20029 | 706 patients presenting to a trauma ICU at a Level I center in Miami, FL underwent prospective evaluation for IAH and ACS. Data collected included abdominal pressures, requirement for laparotomy, and subsequent patient outcomes. | 15 of 706 patients displayed IAH, of the 15, six developed ACS. The six patients with abdominal compartment syndrome had a mean (s.d.) ISS of 34(12) and an intra-abdominal pressure of 42(11) mmHg. Three of the six patients died from progressive multiple organ failure despite abdominal decompression. Notably, two of the six patients developed abdominal compartment syndrome despite ‘prophylactic’ temporary abdominal closure. The nine patients with intra-abdominal hypertension who did not undergo abdominal decompression had a mean (s.d.) ISS of 27(12) and a mean (s.d.) intra-abdominal pressure of 26(4) mmHg. Two of these nine patients died, one from a late pulmonary embolus during rehabilitation after discharge from the ICU and one from complications of a severe closed head injury. | There were trends toward increased ISS and increased mortality rate in the patients with abdominal compartment syndrome vs. those with IAH, however, the only statistically significant difference between those with IAH and ACS were intra-abdominal pressure: 26(4) versus 42(11) mmHg (P < 0·05). |
| Meldrum, et al. 199710 | I45 patients with an injury severity score (ISS) >15, presenting to a Level I trauma center in Denver, CO; were prospectively evaluated for the development of ACS. Time to laparotomy, mean IAP at time of laparotomy were recorded. Cardiopulmonary function, renal function, pulmonary capillary wedge pressure, and SVR were determined prior to and upon completion of laparotomy. | 21 Patients (14%) developed ACS requiring laparotomy; mean age 39± 9 years; injury mechanism: blunt in 60%; ISS 26±6. Mean IAP prior to laparotomy 27±2.3mmHg, time from laparotomy to decompression 27±4 hours. Laparotomy planed in 24% of cases, prompted in the remaining secondary to cardiopulmonary deterioration (43%), renal dysfunction (19%), and both cardiopulmonary and renal dysfunction (14%). | ACS develops in a significant number of severely injured patients. Cardiopulmonary deterioration is the most frequent reason prompting decompression. Timely decompression results in the improvement of cardiopulmonary and renal function. |
| Study Author | Methods | Results | Conclusions |
| Retrospective Study | |||
| Offner, et al. 200111 | Retrospective cohort study of 52 trauma patients requiring damage control laparotomy, who survived >48 hours; during the 5 years of the study. Patients presented to a Denver, CO Level I trauma center. Main outcome measures: ACS, ARDS, MOF. | Mean (± SD) age: 33 ± 2 years; 38 (73%) male. Mechanism of injury was blunt in 29 patients (56%), and mean (± SD) Injury Severity Score was 28 ± 2. Development of ARDS and/or MOF was seen in 23 patients (44%); ARDS and MOF increased mortality from 12% (3/26) to 42% (11/26). Abdominal compartment syndrome was a common complication (17/52), and was associated with an increase in ARDS and/or MOF (12 patients [71%] vs. 11 patients [31%] without ACS; P =.02, [chi]2 test) and death (6 [35%] vs. 8 patients [23%] without ACS). | ACS is a serious complication that increases ARDS and/or MOF and mortality. |
Diagnosing Abdominal Compartment Syndrome in the ED
The diagnosis of IAH and ACS begins with clinical suspicion. By maintaining a broad differential, to include ACS in the appropriate setting, the ED physician can take steps to address the morbidity and mortality associated with this condition.
In reference to our patient…
Blunt abdominal injury and pelvic ring injuries requiring massive transfusion, damage control laparotomy, and pelvic packing => primary and secondary etiologies pre-dispose her to ACS. In addition to a neurological exam to assess cerebral function, laboratory studies, monitoring vitals and I&Os, the ED physician possesses an additional tool to aid in making the diagnosis:
Courtesy of Clare Roepke and her EM:RAP co-authors12:
Craft Your Own IAP Gauge:
IAP measurements are taken through the bladder. The only materials required for obtaining an IAP in the ED are a Foley catheter with pressure monitor side port +/- an arterial line kit.
Method One:
Insert the Foley into a supine patient, lying flat; drain the bladder and then clamp the Foley tubing. Insert 25mL NS into the side port and clamp the port (to maintain the fluid in the bladder). Next, attach the Foley to the pressure transducer and connect it to the arterial line. Zero the pressure to the level of the bladder and this is your IAP.
Method Two:
Insert the Foley into a supine patient, lying flat; drain the bladder and clamp the Foley. Instill 25mL NS into the side port and clamp the port. Raise the Foley tubing into the air (perpendicular to the patient), unclamp the tubing, and measure how far the fluid rises against gravity – record this in centimeters. Finally, employ your favorite search engine to convert from cm to mmHg.
Managing Abdominal Compartment Syndrome in the ED
The most important step in managing ACS in the ED is specialty consultation. As mentioned above, the only accepted definitive management of ACS is surgical decompression.2,6,8,10
Temporizing measures to be taken:
- Decompress what you can, while you can:
- Place an NGT, place a Foley, consider administering an enema if clinically appropriate.1, 12
- Improve abdominal wall compliance:
- Consider sedation, elevate the head of the bed >20-30 degrees, consider reverse Trendelenberg. 1,12
- Optimize fluid administration:
- Avoid gross fluid overload if possible. 1,12
- Optimize tissue perfusion:
- Initiate MAP goal directed resuscitation and hemodynamic monitoring. 1,12
- Consider abdominal imaging if the etiology is unknown (atraumatic):
- CT vs. US 1,12
Let’s Recap a Few ACS Take-Aways
- IAH is prolonged IAP >12mmHg; ACS is IAP >20mmHg with end organ dysfunction.
- ACS has significant morbidity and mortality.
- IAH and ACS should be on your differential for common ED presentations.
- Trauma, shock, severe burns, pancreatitis, sepsis => anybody requiring massive resuscitation.
- Remember: ACS can occur s/p abdominal procedures, and can also occur in children.
- Perform your H&P, send appropriate studies, and if you suspect IAH or ACS => check a bladder pressure.
- ACS = Consult a surgeon
- Temporize by evacuating intraluminal contents, improving abdominal wall compliance, optimizing fluid administration, optimizing tissue perfusion, and evaluating for undiagnosed etiologies in atraumatic ACS.
References / Further Reading
1. Rizoli S, Mamtani A, Scarpelini S, and Kirkpatrick A. Abdominal compartment syndrome in trauma resuscitation. Curr Opin Anaesthesiol 2010; 23: 251-257.
2. De Backer, D. Abdominal compartment syndrome. Crit Care 1999; 3(6): R103-R104.
3. Harrison S, Smith J, Lambert A, Midwinter M. Abdominal compartment syndrome: an emergency department perspective. Emerg Med J 2008; 25: 128-132.
4 . Hong J, Cohn S, Perez J, et al. Prospective study of the incidence and outcome of intra-abdominal hypertension and the abdominal compartment syndrome. Br J Surg 2002; 89: 591-596.
5. Perks D, Grewal H. Abdominal compartment syndrome in pediatric patient with blunt trauma. J Trauma Nurs 2005; 12(2): 50-54.
6. Balogh Z, Lumsdaine W, Moore E, Moore F. Postinjury abdominal compartment syndrome: from recognition to prevention. Lancet 2014; 384: 1466-1475.
7. Diebel L, Wilson R, Dulchavsky S, Saxe J. Effect of increased intra-abdominal pressure on hepatic arterial, portal venous, and hepatic microcirculatory blood flow. J Trauma 1992; 33: 279-282.
8. Balogh Z, McKinley B, Holcomb J, et al. Both primary and secondary abdominal compartment syndrome can be predicted early and are harbingers of multiple organ failure. J Trauma 2003; 54: 848-859
9. Hong J, Cohn S, Perez J, Dolich M, Brown M, et al. Prospective study of the incidence and outcome of intra-abdominal hypertension and the abdominal compartment syndrome. Br J Surg 2002; 89: 591-596.
10. Meldrum D, Moore F, Moore E, Franciose R, Sauaia A, et al. Prospective characterization and selective management of the abdominal compartment syndrome. Am J Surg 1997; 174: 667-672.
11. Offner P, De Souza A, Moore E, et al. Avoidance of abdominal compartment syndrome in damage control laparotomy after trauma. Arch Surg 2001; 136: 676-681.
12. Roepke C, Benjamin E, Jhun P, Bright A, Herbert M. Air in the Belly: A discussion of abdominal compartment syndrome. Ann Emerg Med 2016; 67:17-19.





