Authors: Colton Langridge, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital) and Dustin Williams, MD (EM Attending Physician / APD, UTSW / Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
Case
A 65-year-old female of Vietnamese descent with past medical history of hypertension and diabetes mellitus type 2 presents with acute onset right sided headache that began while reading in dim light 3 hours prior to arrival. The location of the pain is in the peri/retroorbital region on the right and radiates to the right temple. She is seeing halos around lights and has vomited twice on the way to the ED. She has never had a headache of this quality in the past. The remainder of her review of systems is negative, including trauma. She has a history of “sulfa allergy” 5 years ago while taking Bactrim in which she developed hives and shortness of breath.
She is hypertensive, while the remainder of her vital signs are unremarkable. On exam, she has scleral injection, a hazy cornea, and mid-dilated, fixed pupil. The globe itself feels rock hard on palpation. There is no proptosis or palpable cord in the R temporal region. Extraocular muscles are intact, and she has a normal neurological exam including no meningismus.
Visual acuity is performed, and she has 20/80 OS and 20/200 OD. Her baseline is 20/80 in each eye, and she does wear reading glasses. Her fluorescein stain reveals no abnormal uptake. Fundoscopic exam is difficult due to corneal haziness. Tonometry in the L eye shows a pressure of 28 mmHg. The pressure in her R eye is elevated to 72 mmHg.
Timolol and brimonidine eye drops are ordered and administered with repeat tonometry performed every 30 minutes, while awaiting ophthalmology’s arrival. Her OD pressure consistently drops until her IOP is under 35 mmHg. Ophthalmology recommends starting topical steroids and informs you that they plan to perform Laser Peripheral Iridotomy in the next 24 to 48 hours after the haziness in her cornea subsides.
Introduction
Acute angle closure glaucoma (AACG) is the acute elevation of intraocular pressure due to diminished outflow of aqueous humor through the anterior chamber of the eye into the peripherally located canal of Schlemm. It occurs in 1 in 1000 whites and as frequently as 1 in 100 Asians. It occurs even more frequently in those of Inuit descent with estimates of 2-4 in 100 (1). The importance of this disease entity lies in its proclivity to cause optic nerve ischemia. As a result, AACG can lead to visual impairment or blindness if not treated early and appropriately.
Pathophysiology
Aqueous humor is produced by the ciliary epithelium covering the ciliary body in the posterior chamber of the eye. Production is under the control of sympathetic β receptors. After production, aqueous humor flows from the posterior chamber, then between the angle of the lens and iris, through the pupil into the anterior chamber, and finally into the trabecular meshwork located anterior to the ciliary body at the junction of the cornea and sclera. From the trabecular meshwork, aqueous humor flows through the canal of Schlemm where it is resorbed. Two types of acute angle closure glaucoma exist; primary and secondary. Primary AACG occurs in the absence of a precipitating event or insult. In Primary AACG aqueous humor is restricted from flowing through the more anteriorly located pupil due to the posterior iris becoming attached to the lens behind it causing diminished outflow. (6) As aqueous humor accumulates, the iris is pushed forward, especially at its peripheral margin, causing a bowing effect that then causes impingement on the trabecular network and canal of Schlemm. This further restricts outflow. Patients who already have shallow anterior chambers are particularly at risk, as the angle between the peripheral iris and trabecular meshwork is already narrow and predisposed to sudden closure. Those of Asian (especially Inuit descent) and women tend to have a more narrow anterior chamber, which increases the risk of developing AACG.
There are many precipitants that can contribute to the development of AACG. A classic story is the acute onset of eye pain after walking into a movie theater (i.e. a dimly lit room). Reading in dim light can also precipitate AACG. Sympathomimetics and anticholinergics can both cause pupillary dilatation and thus AACG.
Diagnosis
AACG, for the emergency physician, is a clinical entity that is diagnosed based on a combination of clinical suspicion and exam findings. IOP as detected by applanation tonometry will be elevated. Acute onset eye pain and a minimally reactive mid-dilated pupil with elevated intra-ocular pressure (usually greater than 30 mmHg) is highly suggestive of AACG.
In recent years, more formal criteria have been used to diagnose AACG. These criteria include at least 2 of the following complaints/symptoms: ocular pain, a history of intermittent visual blurring which may include the complaint of seeing halos, and nausea or vomiting. At least 3 of the following signs are required: IOP greater than 21 mm Hg, corneal edema, conjunctival injection, a mid-dilated minimally reactive pupil, and a shallow anterior chamber (11).
A narrow anterior chamber can be determined by oblique flashlight test. This test is performed by shining a flashlight tangentially in a lateral to medial direction across the patient’s eye in a dark room. If there is a shadow over the medial aspect of the iris then the anterior chamber is narrow (5).
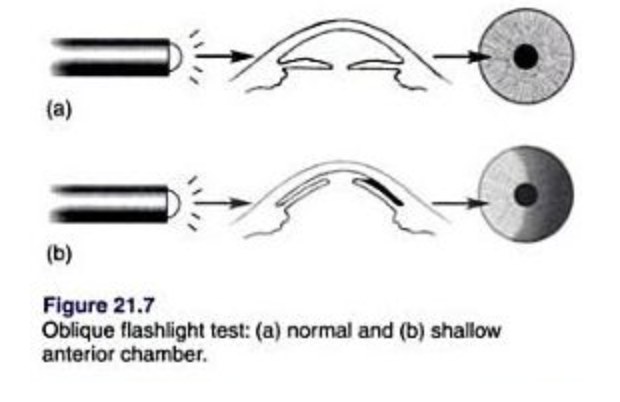
From: http://littlewhitecoats.blogspot.com/2010/12/what-is-oblique-flashlight-test.html
Consultation
An immediate ophthalmology consultation should be made once the Emergency physician suspects this diagnosis. As more time elapses, more optic nerve atrophy will occur (10).
Treatment
In the acute setting, the goal is to emergently reduce IOP, not to perform definitive therapy. This can be started before ophthalmology arrives. Several types of eye drops and a few intravenous medications are effective in rapidly reducing IOP. Most of these medications used for one of the following two mechanisms: increasing aqueous humor outflow or reducing production of aqueous humor altogether. The particular medication regimen that is chosen should be tailored based on a patients’ past medical history and previous drug allergies. The table below summarizes the various medication choices frequently chosen in the acute management of AACG.
| Medication Class | Medication | Pharmacology | Adverse Effects/Cautions |
| Beta Blockers | Timolol 0.5% | Decrease production of aqueous humor | Systematically absorbed/caution in asthma/COPD |
| Alpha 2 Agonists | Brimonidine 0.15% | Decrease production of aqueous humor and increase outflow | |
| Carbonic Anhydrase Inhibitors | Acetazolamide (Diamox) 500 mg IV or PO | Decrease production of aqueous humor | Sulfa drug; Use caution in Sulfa allergic patients; Avoid in patients with Sickle cell disease (increased sickling) |
| Prostaglandin Analogs | Latanoprost 0.005% | Increase aqueous humor outflow | Browning of the iris |
| Muscarinic Agonists | Pilocarpine 1-2% | Increase aqueous humor outflow
|
Ineffective at high IOP |
| Topical Steroids | Prednisolone 1% | Decrease inflammation and synechiae formation | Use in conjunction with ophthalmology |
| Desiccating Agents/Hyperosmotic Agents | Mannitol 1-2g/kg IV | Draw fluid out of the vitreous humor by osmotic pressure | Caution with use in patients with intravascular volume depletion |
*Because aqueous humor production is stimulated by β receptors, β blockers are effective in decreasing further production of aqueous humor. Timolol functions in this way.
*Alpha 2 receptors in the eye (as elsewhere in the body) inhibit sympathetic stimulation. Alpha 2 agonism functions to decrease aqueous humor production by reducing sympathetic outflow and thereby decreasing the β mediated aqueous humor production. Alpha 2 agonism also decreases the mydriatic effect of sympathetic stimulation on the iris through alpha 1 receptors. Brimonidine functions in this manner.
*Carbonic anhydrase is an enzyme that is used in erythrocytes and in the renal tubule for bicarbonate/CO2 titration and/or buffering effects. In the eye it is used for aqueous humor production. Inhibition of this enzyme minimizes production through this pathway. Acetazolamide functions in this way.
*Prostaglandin analogs are thought to increase aqueous humor outflow without affecting its production. One proposed mechanism suggests that they work by altering the production of matrix metalloproteinases. These are thought to cause changes in the extracellular matrix of the iris and widening of connective tissue filled spaces. (4)
*Muscarinic agonists cause miosis. This may help pull the posterior iris from the lens, thereby helping to increases aqueous humor outflow through the pupil. Pilocarpine works by this mechanism. Unfortunately, under high intraocular pressure settings, pilocarpine is less effective. This is because during these conditions, pressure induced ischemic paralysis of the iris decreases its effectiveness. There is also concern that by constricting the ciliary muscles, pilocarpine may increase the axial thickness of the lens and cause anterior displacement, which may reduce the depth of the anterior chamber effectively worsening outflow of aqueous humor. Pilocarpine should be given after other eye drops.
*Topical steroids decrease the overall inflammatory response and scar tissue/synechiae formation.
*Mannitol works by drawing water out of the vitreous humor by osmotic means, thereby decreasing the overall fluid in the eye, dropping the pressure.
*It’s important to give adequate pain control with opioids such as morphine or fentanyl. Antiemetics should be given for nausea and vomiting.
Start with a topical β blocker and alpha 2 agonist +/- diamox. Diamox can be given by mouth if IOP is not excessively elevated (i.e. less than 40). If highly elevated, IV Diamox is preferred. Topical pilocarpine can be considered but should be used with caution 1-2 hours after IOP is reduced for the reasons stated earlier. If IOP is not significantly reduced by 25% at 30-60 minutes, an osmotic agent should be strongly considered. The goal IOP should be 35 or less (3).
If IOP is not effectively reduced in a timely manner, corneal indentation (CI) can be considered (9). This is performed by indenting the cornea with a soft instrument (i.e. cotton tipped applicator) after administration of a topical anesthetic. By indenting the cornea, aqueous humor is displaced peripherally, opening the angle and increasing aqueous outflow temporarily.
Definitive therapy is performed by ophthalmology by means of Laser Peripheral Iridotomy (LPI). Ideally, this is performed within 24 to 48 hours. However, LPI must be performed under circumstances in which visibility is optimal. In many cases of AACG, corneal haziness impairs visibility. Once IOP is reduced, water is drawn out of the cornea and visibility improves, thus allowing LPI to be performed. LPI may need to be performed on the consensual eye in order to prevent AACG in that eye as well.
Disposition
Disposition should be made in conjunction with ophthalmology. There should be a low threshold for admission, especially for those who receive osmotic diuretics, as they may require further electrolyte monitoring. For those who will follow up as outpatients, patients must be able to reliably follow up in an ophthalmology clinic within the next 24-48 hours. In addition, they should be discharged with topical IOP lowering agents, as definitive therapy (LPI) will not have been performed yet.
Summary
- Consider AACG in all patients presenting with headache and visual changes, especially if associated with nausea and vomiting.
- AACG occurs more frequently in females and those of Asian descent.
- Early and effective therapy is vital in reducing optic nerve ischemia and vision loss. Time is optic nerve.
- Be aware of the patient’s comorbidities and allergies before treating (i.e. be aware of the risks of topical β blockers in COPD/asthma, sulfa allergy with acetazolamide use)
- Consider corneal indentation as a temporizing maneuver if IOP is not satisfactorily lowered in a reasonable amount of time.
- There is no emergent treatment that an ophthalmologist can offer that an emergency physician cannot. Definitive treatment is with LPI, however this is frequently delayed until corneal clearing occurs. Thus topical and IV agents are paramount in early treatment of AACG.
References / Further Reading
- He M, Foster PJ, Ge J, Huang W, Zheng Y, Friedman DS. Prevalence and clinical characteristics of glaucoma in adult Chinese: a population-based study in Liwan District, Guangzhou. Invest Ophthalmol Vis Sci. 2006 Jul. 47(7):2782-8.
- Ang LP, Ang LP. Current understanding of the treatment and outcome of acute primary angle-closure glaucoma: an Asian perspective. Ann Acad Med Singapore. 2008 Mar. 37(3):210-5.
- Singer MS, Salim S. Bilateral acute angle-closure glaucoma as a complication of facedown spine surgery. Spine J. 2010 Sep. 10(9):e7-9.
- Toris CB, Gabelt BT, Kaufman PL. Update on the mechanism of action of topical prostaglandins for intraocular pressure reduction. Surv Ophthalmol. 2008 Nov;53 Suppl1:S107-20.
- Coleman AL. Glaucoma. The Lancet; Nov 20, 1999; 354, 9192
- Tarongoy P, Lin C, Walton D. “Angle-closure Glaucoma: The Role of the Lens in the Pathogenesis, Prevention, and Treatment”. Survey of Ophthalmology, Volume 54 Number 2 2009.
- Choong YF, Irfan S, Menage M. Acute angle closure glaucoma: an evaluation of a protocol for acute treatment. Eye (1999) 13, 613-616.
- Emanuel ME et al. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol 2014, 25:89–92.
- Masselos K, Bank A, Francis IC, Stapleton F. Corneal indentation in the early management of acute angle closure. Ophthalmology. 2009 Jan. 116(1):25-9.
- Weizer J. Angle-Closure Glaucoma. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on August 5 2016.)
- Khondkaryan Ani, Francis Brian A. Angle Closure Glaucoma. American Academy of Ophthalmology. https://www.aao.org/munnerlyn-laser-surgery-center/angleclosure-glaucoma-19. Dec18, 2013.




