Author: Josh Poles, DO (Attending Physician, John Peter Smith Health Network, Fort Worth, Texas and Methodist Charlton Medical Center, Dallas, Texas) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Manpreet Singh, MD (@MPrizzleER)
Featured on the LITFL Review #173 – Thanks to Mat Goebel and the LITFL Review group for the shout out!
Cases:
- 39 year old female, hx of bipolar, presents with 2 weeks of worsening GI cramps, mild tremor, and ataxia.
- 35 year old male, no past medical history, presents with acute onset of “feeling off balance,” described as “falling to my left when I walk.”
- 65 year old male, history of hypertension, diabetes, hyperlipidemia and obesity presents with 1 week of worsening difficulty walking, standing, and states “it’s hard to talk.”
Introduction
Ataxia: Incoordination of volitional movement. It represents a wide range of overlapping symptoms. The differential diagnosis is wide and includes benign as well as life-threatening diseases.
- The effects of cerebellar disease involve
- Loss of acceleration and deceleration movements
- Clumsiness managing the rate, range, and force of movement (2).
Pearls
- Complaints of dizziness, vertigo, weakness, nausea, vomiting, and falling are common.
- Ataxia is different than pure alterations in gait and must be understood.
- Central causes of ataxia are most concerning and include multiple sclerosis, vertebrobasilar insufficiency, acoustic neuromas, infections, and intoxications.
- Posterior circulation strokes can be particularly debilitating and carry a mortality rate of 7-20% even despite intervention (1, p 440).
- The misdiagnosis of posterior fossa infarcts in the Emergency Department is frequent.
- Non-cerebellar, supratentorial lesions are capable of causing isolated motor ataxia (2,4).
What does the cerebellum control?
- The coordination of movements, especially skilled voluntary ones.
- The control of posture and gait, and the regulation of muscular tone.
- The coordination and fluid movements of the limbs and trunk (permits an ongoing and almost instantaneous comparison between desired and actual movements while the movements are being carried out).
Two Types of Ataxia:
- Motor Ataxia (cerebellar ataxia) – sensory receptors and afferent pathways remain functional, but integration of proprioceptive information is lacking. A lesion within the lateral cerebellum may cause:
- Ipsilateral limb ataxia.
- Axial muscle incoordination, manifested by inability to sit upright or maintain a standing position. These findings may be compromised by a midline lesion of the cerebellum.
- Midline cerebellar lesions may also present with a wide-based, uncoordinated gait (the drunken sailor gait).
- Sensory ataxias are caused by disrupted proprioception and position sense signals to the CNS.
- Sensory ataxias may be compensated for by visual input. Removal of visual information, for example closing the eyes or poor lighting, may often worsen sensory ataxia.
- Caused by disrupted peripheral nerves or input tracts of spinal cord lesions
- Despite intact cerebellar function and motor systems, uncoordinated motor function will be present.
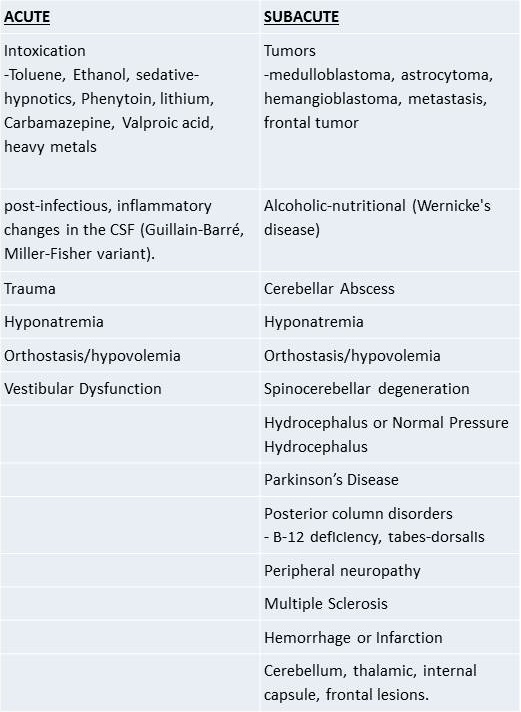
Causes to Consider:
How to Test for Ataxia:
- Rapid alternating movements (RAM) – supination and pronation of forearms
- Finger-to-nose, and heel-to-shin
- Romberg testing
- NIH Stroke Scale
- Gait testing
- Deep tendon reflexes
- Dysdiadochokinesis – Defects in alternation or rapid change in direction of movement such as pronation
- How To Test: Evaluate rapid supination of the forearm or successive touching of each fingertip to the thumb.
- Abnormal Results: Inability to perform rapid alternating movements. Movements become more irregular with increased speed.
- Dysmetria – Overshooting or undershooting a target during volitional movement. There will be irregularity and slowing of movement during both acceleration and deceleration.
- How to Test: (Ask the patient to make movements quickly and accurately)
- Finger-to-nose and toe-to-finger movement
- Running the heel down the opposite shin
- Tracing a square in the air with a hand or foot.
- Abnormal Results: Inability to move the limb to the target accurately and rapidly. (These abnormalities are particularly prominent as the finger or toe approaches its target). With regards to the NIHSS, in case of visual neglect test within functional visual field. Ataxia is scored if it is present out of proportion to weakness. Ataxia is considered absent in patients who cannot understand or are paralyzed. In blind patient, have them touch their nose from extended arm position.
- How to Test: (Ask the patient to make movements quickly and accurately)
- Dysarthria – Incoordination of the muscles of articulation
- How to Test: use NIH Stroke Scale. Have the patient repeat the words “Mama, tip-top, fifty-fifty, thanks, huckleberry, baseball player.”
- Abnormal Results: Words should be crisp and clear with no slurred speech. Also look for variations in voice intensity.
- Check Reflex (Rebound Phenomenon) – An intact check reflex will allow the patient to activate the opposing muscles to slow and stop forced impending motion of a limb.
- How to Test: Have the patient flex their elbows isometrically against resistance.
- Abnormal Result: When the resistance is suddenly removed without warning, the patients’ arms may swing up uncontrollably and even hit themselves.
https://www.youtube.com/watch?v=CbPFuVrGKmU
- Gait – During normal gait the body is erect, the head is straight, arms hang relaxed by the sides, each movement is rhythmic. There should be coordinated flexion of the hip and knee, dorsiflexion of the foot and the foot should just barely clear the ground. The heel normally strikes the ground first.
- How To Test:
- Observe the patient sit upright on the stretcher.
- Have the patient rise, stand, walk, turn around and sit back down.
- Have the patient walk heel-to-toe.
- Abnormal Results
- Inability to hold themselves up in a seated position.
- Wide base gait.
- Truncal or ambulatory unsteadiness.
- Irregularity of steps
- Lateral veering
- Inability to walk heel-to-toe
- Unsteadiness when rising from a chair, turning suddenly or when abruptly asked to stop walking.
- How To Test:
- Romberg – It is primarily a test of sensation, vibratory sense, and posterior columns. If positive, may distinguish sensory from motor ataxia.
- How to Test: While standing with arms outstretched, feet narrowly spaced and the eyes open, the patient is observed for signs of unsteadiness. The patient is then asked to close their eyes.
- Abnormal Result: If the ataxia worsens with this loss of visual input, then the Romberg sign is present or positive, suggesting sensory ataxia with a problem of proprioceptive input (posterior column, vestibular dysfunction), or a peripheral neuropathy.
- In patients who are unsteady with eyes open and show little or no change in their unsteadiness with eye closure (Romberg test–negative), a motor ataxia is suggested with possible localization of that problem to the cerebellum.
- Position sense – tests the dorsal spinal columns.
- Testing- With the patient’s eyes closed, grasp the side of each great toe individually and move the toe inferiorly and superiorly.
- Abnormal Result: Inability to sense the appropriate position of movement.
Case Discussion:
- 39 year old female, hx of bipolar, presents with 2 weeks of worsening GI cramps, mild tremor, and ataxia.
- Consider acute intoxication or lithium toxicity. This patient needs lithium level, CBC, chemistry, toxicology labs, and EKG.
- 35 year old male, no past medical history, presents with acute onset of “feeling off balance,” after heavy work out 2 days ago. Symptoms are described as “falling to my left when i walk.”
- In a young person, consider vertebral artery dissection. This patient needs CT head/neck w/ contrast, CBC, Chemistry panel, neurology consultation, and warrants admission for further workup.
- 65 year old male, history of hypertension, diabetes, hyperlipidemia and obesity presents with 1 week of worsening difficulty walking, standing, and states “it’s hard to talk.”
- This is an elderly patient presenting with the classic symptoms of posterior stroke (ataxia and dysarthria). This patient needs CBC, Chemistry, EKG, CT head likely followed by MRI/MRA head/neck – stroke protocol, neurology consultation, and warrants admission for further workup.
References // Further Reading:
– Mattu A, Chanmugam S, Swadron S, et al. Avoiding Common Errors in the Emergency Department. Philadelphia: Lippincott Williams & Wilkins, p. 440. Print.
– Ropper, Allan H., et al. “Chapter 5. Ataxia and Disorders of Cerebellar Function.” “Chapter 7. Disorders of Stance and Gait.” Adams & Victor’s Principles of Neurology, 10e. Eds. Allan H. Ropper, et al. New York, NY: McGraw-Hill, 2014. n. pag. AccessMedicine. Web. 28 Jan. 2015. <http://accessmedicine.mhmedical.com/content.aspx?bookid=690&Sectionid=45424414>.
– Martin-Schild S, Alright KC, Tanksley J, et al. Zero on the NIHSS Does Not Equal Zero. Ann Emerg Med. 2011 Jan;57(1):42-5. doi: 10.1016/j.annemergmed.2010.06.564. Epub 2010 Sep
– Huff, J. Stephen. “Ataxia and Gait Disturbances.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. Eds. Judith E. Tintinalli, et al. New York, NY: McGraw-Hill, 2011. n. pag. AccessEmergency Medicine. Web. 28 Jan. 2015. <http://accessemergencymedicine.mhmedical.com/content.aspx?bookid=693&Sectionid=45915507>.








2 thoughts on “Acute Ataxia in the ED Highlights”
Pingback: LITFL Review 173 - LITFL
Pingback: LITFL Review 173 • LITFL Medical Blog • FOAMed Review