Authors: Jessica Zack, MD (EM Chief Resident at SAUSHEC, USAF) and Brit Long, MD (@long_brit, EM Attending Physician at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
A 64-year-old male presents with sudden onset subjective fever/chills, dyspnea, weakness, and mild hemoptysis that began 2 hours prior to arrival. His VS include HR 104, BP 103/62, RR 24, O2 Sat 84% on RA, and T 99.6. On exam, you note bilateral rales R > L, a 4/6 diastolic murmur consistent with his known history of aortic regurgitation, and JVD without peripheral edema. His EKG is only significant for sinus tachycardia. You send labs that include a BNP and troponin and order a stat portable CXR which is pictured below. You subsequently order a CT scan of the chest and start him on NIPPV. You are initially considering PE, ACS, multi-lobar pneumonia, and acute heart failure syndrome … but is there something else you’re missing?

The prevalence of valvular heart disease in the United States is estimated to be about 2.5% and increases in prevalence with age.1 Though patients with clinically evident valvular heart disease have a 3.2-fold increase risk for stroke and 2.5-fold increase risk for death,2 most valvular heart disease encountered in the emergency department is chronic and does not require emergency stabilization.3 This is vastly different than the rare patient presenting with an acute valvular emergency. Symptoms of an acute valvular emergency may include dyspnea, tachycardia, pulmonary edema, and rapid development of cardiogenic shock. Many of these symptoms are seen with various other diagnoses, and the biggest pitfall clinicians may experience is leaving acute valvular emergency off the differential for patients presenting with acute dyspnea.
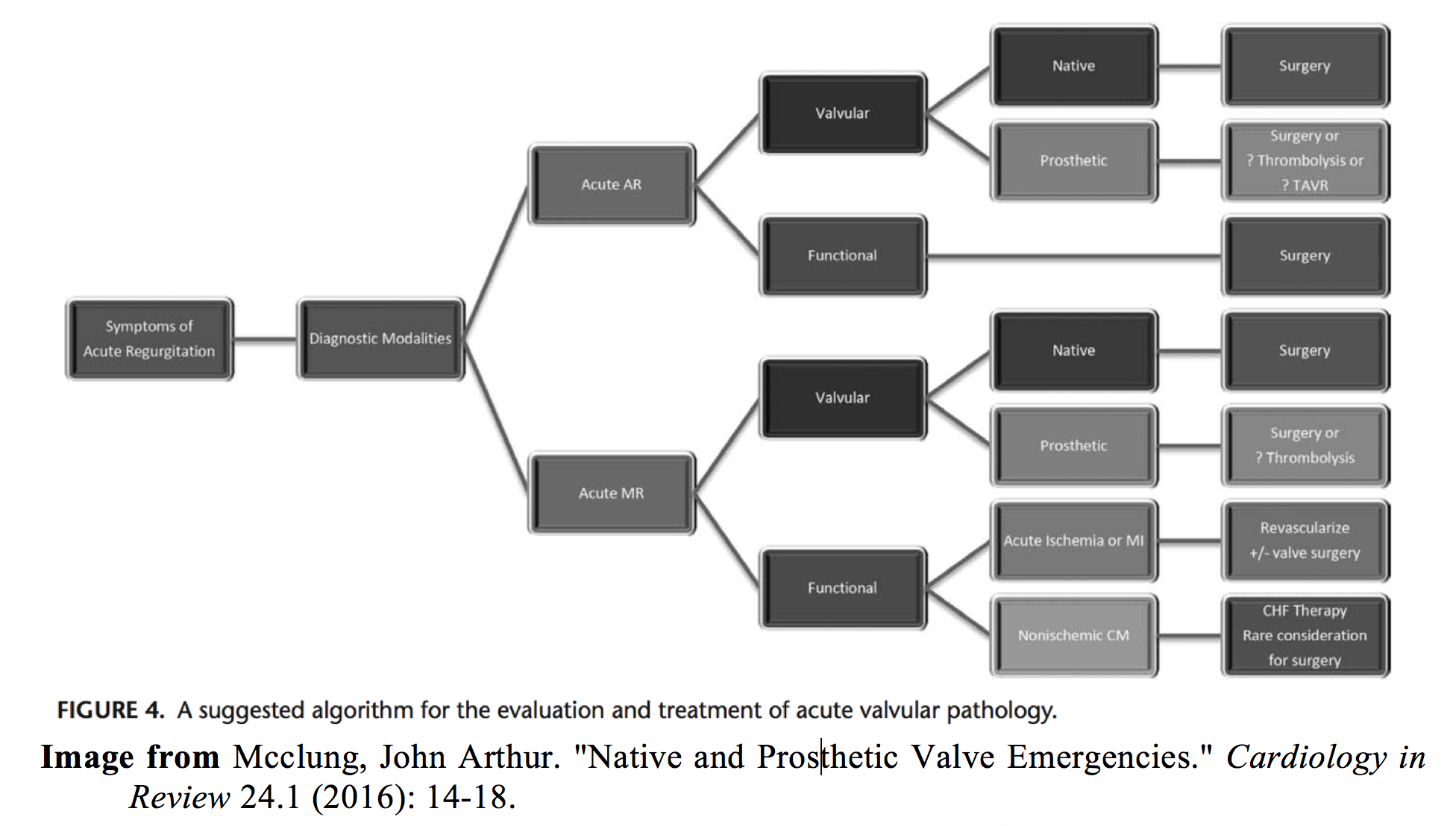
Valvular emergencies can be broken down by type of valve: native or prosthetic. Native valve emergencies are almost always the result of regurgitation, while acute prosthetic valve dysfunction may be the result of either regurgitation or stenosis.4
Valvular Structure and Function:
The heart is composed of four valves: the mitral and tricuspid valves (atrioventricular valves) and the pulmonic and aortic valves (semilunar valves). These valves all open and close passively in response to changes in pressure and volume. The right side of the heart functions similarly to left except that these valves experience much lower pressures. Since most native valve emergencies involve the mitral and aortic valves, we will focus our discussion here. In a normally functioning heart, the aortic valve is open during ventricular systole. This allows blood to flow from the left ventricle into systemic circulation. Once the aortic root pressure supersedes that of the left ventricle, the three cusps of the aortic valve fold in, and valve closure occurs. This marks the beginning of ventricular diastole. During this phase of the cardiac cycle, the mitral valve opens allowing flow from the left atrium to the left ventricle. Filling of the left ventricle is completed after the atrial “kick” which provides 10-40 % of the left ventricular end-diastolic volume.5 This is followed by closure of the mitral valve, and the cycle begins again with ventricular contraction. The anterior and posterior leaflets of the mitral valve are supported by the papillary muscles and chordae tendinae during ventricular contraction and aid in the prevention of reverse flow in the left atrium.6
a normally functioning heart, the aortic valve is open during ventricular systole. This allows blood to flow from the left ventricle into systemic circulation. Once the aortic root pressure supersedes that of the left ventricle, the three cusps of the aortic valve fold in, and valve closure occurs. This marks the beginning of ventricular diastole. During this phase of the cardiac cycle, the mitral valve opens allowing flow from the left atrium to the left ventricle. Filling of the left ventricle is completed after the atrial “kick” which provides 10-40 % of the left ventricular end-diastolic volume.5 This is followed by closure of the mitral valve, and the cycle begins again with ventricular contraction. The anterior and posterior leaflets of the mitral valve are supported by the papillary muscles and chordae tendinae during ventricular contraction and aid in the prevention of reverse flow in the left atrium.6
Acute Aortic Regurgitation
Pathophysiology: Acute aortic insufficiency is typically the result of either acute aortic dissection or endocarditis.7 It has also been reported in the case of blunt chest trauma.8 In acute aortic regurgitation (AR), the left ventricle (LV) pathologically fills during ventricular diastole preventing forward flow from the left atrium (LA). This greatly reduces stroke volume and causes a compensatory tachycardia to maintain cardiac output. In the acute setting, this regurgitation is met by a relatively stiff LV and causes increased LV pressure. The increased pressure in the LV stifles flow from the left atrium (LA) and may cause pulmonary congestion. In severe AR, increased LV pressure may cause early closure of the mitral valve prior to atrial systole and exacerbate pulmonary congestion as the atria contracts against a closed valve.9,10 When AR is severe enough, the decreased cardiac output leads to progressive hypotension, peripheral vasoconstriction, and cardiogenic shock.
History/Exam: These patients will typically present with sudden onset of dyspnea. Other significant historical features may include those associated with the underlying cause of their AR such as tearing chest pain in aortic dissection or fevers in the setting of endocarditis. Physical exam may reveal evidence of pulmonary edema and cardiogenic shock such as rales, JVD, hypotension, pallor, and diaphoresis.3,13 Don’t be fooled by the absence of the typical blowing diastolic murmur in this patient. Murmurs are created by the velocity of blood flow over the valve. This velocity is largely determined by pressure gradients. In the acute AR versus chronic AR, the LV is less compliant which lends to equalization of end diastolic pressure in the aorta and LV.10 With a decreased pressure gradient, your murmur will likely be softer and shorter. Throw in a noisy ED, tachycardia, tachypnea, and rales, and your murmur may be completely inaudible.
Treatment: Definitive treatment for severe acute AR is immediate surgical intervention. Mortality for acute type A aortic dissection is as high as 1-2% per hour for the first several hours.11 So, how do we keep them alive until the OR?
-Intubate if necessary
-Nitroprusside: Yes, their blood pressure is probably already low. Stay with me. Nitroprusside causes afterload reduction, decreased LV preload, and results in reduced regurgitant volume.12 If your patient is going downhill, consider simultaneously starting dobutamine.
-Dobutamine: This ionotropic agent helps to increase contractility and stroke volume. In combination with nitroprusside, you may be able to achieve increased forward flow and temporize the patient.4,13
-Don’t forget antibiotics in the setting of suspected endocarditis.
Treatment Pitfalls:
-Beta blockers: I know, they’re tempting. Especially if your patient is dissecting. Beta blockers are relatively contraindicated in the case of acute AR.4 Beta blockers will decrease reflex tachycardia, but that tachycardia is currently maintaining their cardiac output. Additionally, that decrease in heart rate will increase the time spent in diastole and cause more aortic regurgitation.4
-Aortic Balloon Counterpulsation: This is absolutely contraindicated.4,13 Remember, the balloon pump will inflate during diastole and definitively make the problem worse.
Acute Mitral Regurgitation
Pathophysiology: The most common cause of acute mitral regurgitation (MR) is rupture of chordae tendinae or papillary muscles from ischemia and is typically seen within the first week following a myocardial infarction.13 However, other causes include leaflet perforation from infective endocarditis, blunt chest trauma, and leaflet tethering in acute cardiomyopathies.3,4,14 In acute MR, blood flows back across the mitral valve during ventricular systole. This causes a precipitous decrease in cardiac output. Additionally, blood is flowing into an atrium with normal compliance. This often results in rapid onset of pulmonary edema. In some cases, unilateral pulmonary edema may be seen. Most commonly, this unilateral edema is isolated to the right side or right upper lobe due to the regurgitant jet, particularly from a posterior flail leaflet, being directed towards the right pulmonary vein.15,16
History/Exam: Like acute AR, acute MR frequently leads to overt cardiogenic shock. One key historical difference is that these patients typically present 2-7 days after acute MI.13 Patients with acute MR present with sudden onset of dyspnea from rapidly amassing pulmonary edema, as well as tachycardia.13 Since the atria has not had time to develop additional compliance like in chronic mitral regurgitation, expect left atrial pressures to be high. Again, without a significant pressure gradient across the valve, don’t be surprised if the typical high-pitched holosystolic murmur is absent. This is particularly true if your regurgitant jet is aimed posteriorly and you are auscultating anteriorly.
Treatment: In addition to treating any underlying ischemia if present, definitive treatment is operative management.
Similar temporizing measures as used in acute AR may be useful here, with a few differences.
-Positive pressure for respiratory failure.3
-Nitroprusside or nitrates for afterload reduction.3,4,13 Often other afterload reducing agents, such as nicardipine, are more readily available in the ED. There is little data available directly evaluating whether other afterload reducing agents have similar clinical effects as nitroprusside.
-Dobutamine for inotropic effects.3,13
-Aortic Balloon Counterpulsation: A balloon pump may provide some benefit here if surgical intervention is not readily available.4,13 This will increase forward flow, increase mean arterial pressure, decrease regurgitant volume, and decrease left ventricular filling pressures.3
-Antibiotics if endocarditis is suspected.
Critical Aortic Stenosis
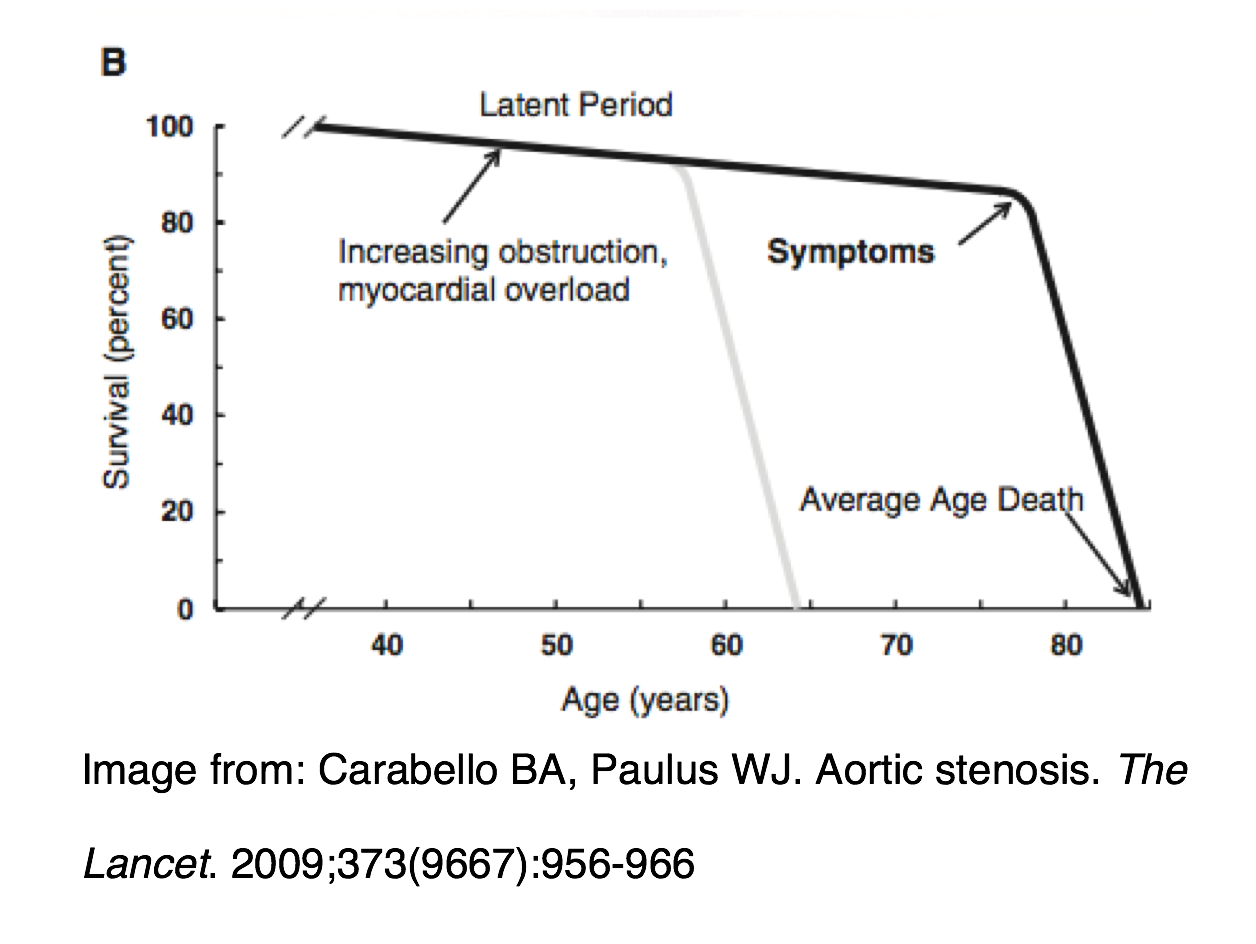
Background: Aortic stenosis (AS) is most commonly caused by age-related calcific changes of a normal valve, calcification of a bicuspid aortic valve, or rheumatic heart disease.17 The difference between AS and the other native valve emergencies discussed in this article is that aortic stenosis develops over many years prior to symptoms onset.18 Even patients with severe aortic stenosis may never develop symptoms, and their estimated risk of sudden cardiac death is still 0.5%-1.0% per year.18 However, once symptom onset does occur, mortality rate rapidly increases. Seventy-five percent of patients will die within 3 years of symptom onset.19
 Pathophysiology: Severe AS is characterized by a fixed outflow obstruction, and cardiac output is preload dependent. Since severity increases over time, LV hypertrophy develops as a compensatory mechanism to maintain ejection fraction. Patients will often maintain a normal ejection fraction, but this is commonly associated with an overall decreased cardiac output due to decreased end diastolic volumes in the hypertrophied LV.18 LV hypertrophy itself reduces diastolic function and impairs coronary perfusion contributing to angina,19 one of the most common symptoms of AS. Another common presenting symptom of AS is syncope during exercise. Though not completely understood, it is theorized that the high resistance across the aortic valve prevents the increase in cardiac output required to maintain normotension during exercise when peripheral vasodilation occurs.18 When the AS becomes severe enough, it can lead to severe LV dysfunction and acute heart failure.
Pathophysiology: Severe AS is characterized by a fixed outflow obstruction, and cardiac output is preload dependent. Since severity increases over time, LV hypertrophy develops as a compensatory mechanism to maintain ejection fraction. Patients will often maintain a normal ejection fraction, but this is commonly associated with an overall decreased cardiac output due to decreased end diastolic volumes in the hypertrophied LV.18 LV hypertrophy itself reduces diastolic function and impairs coronary perfusion contributing to angina,19 one of the most common symptoms of AS. Another common presenting symptom of AS is syncope during exercise. Though not completely understood, it is theorized that the high resistance across the aortic valve prevents the increase in cardiac output required to maintain normotension during exercise when peripheral vasodilation occurs.18 When the AS becomes severe enough, it can lead to severe LV dysfunction and acute heart failure.
History/Exam: The most common symptoms of severe AS are angina, syncope, and dyspnea.17,18 Since severe AS is a disease process that happens over time, you are more likely to appreciate the crescendo-decrescendo systolic ejection murmur. However, it may be absent in the critically ill patient.17 This murmur often radiates into the carotids. Additionally, you may see evidence of LV hypertrophy on EKG and cardiomegaly on CXR. Occasionally, patients with severe AS will present with acute left ventricular dysfunction and signs and symptoms of acute heart failure such as dyspnea, pulmonary edema, JVD, and even cardiogenic shock.
Treatment: There are two types of AS patients generally encountered in the ED: patients who have the potential to be sick at any time and patients who are currently really sick.
Patients with symptomatic AS (potential to be sick):
-IV Fluids: overall, AS is preload dependent, and these patients may require IVF resuscitation to maintain cardiac output.17
-Inpatient admission for echocardiography and evaluation for surgical aortic valve replacement.17,20
Patients with severe AS and failing LV (currently really sick AS), consider the following:
-Nitroprusside:17,19 There is limited data supporting the use of nitroprusside infusion in patients with severe AS and MAP > 60mm Hg.21 In this subset of patients, there is some evidence to suggest nitroprusside will decrease afterload, improve systolic and diastolic function, and reduce myocardial ischemia.22 This newer data goes against traditional teaching that nitrates will cause decreased blood pressure and decreased coronary perfusion.21 This should be considered in patients who can be closely monitored in an ICU setting and in conjunction with cardiology and/or an intensivist.
-Ionotropic agents such as dobutamine.17
-Early consultation with cardiology: in some cases percutaneous balloon dilation may be performed as a temporizing measure in patients too ill to immediately receive aortic valve replacement.20
Prosthetic Valve Emergencies
Acute Valve Thrombosis: During the first three months following surgery, both mechanical and bioprosthetic valves are at the greatest risk for thrombosis and thromboembolic complications.23 However, this risk has a lifelong persistence for patients with a mechanical valve. Thrombosis of a mechanical valve can lead to acute regurgitation, acute stenosis, or both.4 In severe cases, patients will present with acute dyspnea, weakness, and cardiogenic shock. The preferred treatment for patients with acute valve thrombosis is surgery. However, there is some evidence to support the use of intravenous thrombolytics.24 This decision should be made in conjunction with a cardiologist and cardiothoracic surgeon.
Other complications: While acute thrombosis is typically seen with mechanical valves, other complications such as paravalvular regurgitation from suture failure or dehiscence from endocarditis is seen in both mechanical and bioprosthetic valves.4 Up to 6% of prosthetic valves will be complicated by endocarditis within 5 years.3 This finding is associated with an overall poor prognosis, as approximately one third of patients diagnosed with prosthetic valve endocarditis will die within one year of diagnosis.25 If there is suspicion for prosthetic valve endocarditis, blood cultures should be drawn, antibiotics started, and echocardiography and consult with cardiology should be obtained.
Case Resolution:
The patient was admitted to the MICU and was later intubated for worsening respiratory distress. He had an echo performed and was found to have new severe mitral regurgitation with a flail posterior leaflet, in addition to his known chronic aortic regurgitation. After his echo, he was immediately taken to the operating room and underwent uncomplicated valve replacement of both mitral and aortic valves. He recovered uneventfully and was subsequently discharged home.
Key Takeaways:
-In patients presenting with sudden onset dyspnea, always keep a valvular emergency on the differential.
-Murmurs may not be audible in the acute setting.
-Definitive management is surgery more often than not, so get consultants on board early.
-If you have a sick patient with a native valve emergency consider nitroprusside +/- dobutamine.
-If present, don’t forget to treat the underlying cause of aortic regurgitation (aortic dissection, endocarditis), mitral regurgitation (ischemia, endocarditis), or prosthetic valve emergency (endocarditis, thrombosis).
References/Further Reading
- Nkomo, Vuyisile T., Julius M. Gardin, Thomas N. Skelton, John S. Gottdiener, Christopher G. Scott, and Maurice Enriquez-Sarano. “Burden of Valvular Heart Diseases: A Population-based Study.” The Lancet9540 (2006): 1005-011.
- Petty, G. W., B. K. Khandheria, J. P. Whisnant, J. D. Sicks, W. M. O’Fallon, and D. O. Wiebers. “Predictors of Cerebrovascular Events and Death among Patients with Valvular Heart Disease: A Population-Based Study.” Stroke11 (2000): 2628-635.
- Alley, William D., and Simon A. Mahler. “Chapter 54: Valvular Emergencies.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 8th ed. N.p.: McGraw Hill, 2015.
- Mcclung, John Arthur. “Native and Prosthetic Valve Emergencies.” Cardiology in Review1 (2016): 14-18.
- Alhogbani, Tariq, Oliver Strohm, and Matthias G. Friedrich. “Evaluation of Left Atrial Contraction Contribution to Left Ventricular Filling Using Cardiovascular Magnetic Resonance.” Journal of Magnetic Resonance Imaging4 (2012): 860-64.
- Perpetua, Elizabeth M., Dmitry B. Levin, and Mark Reisman. “Anatomy and Function of the Normal and Diseased Mitral Apparatus.” Interventional Cardiology Clinics1 (2016): 1-16.
- Roberts, W. C., J. M. Ko, T. R. Moore, and W. H. Jones. “Causes of Pure Aortic Regurgitation in Patients Having Isolated Aortic Valve Replacement at a Single US Tertiary Hospital (1993 to 2005).” Circulation5 (2006): 422-29.
- Baek, J. H., J. H. Lee, and D. H. Lee. “Acute Aortic Valve Insufficiency following Blunt Chest Trauma.” European Journal of Trauma and Emergency Surgery5 (2010): 499-501.
- Eusebio, Jose, Eric K. Louie, Lonnie C. Edwards, Henry S. Loeb, and Patrick J. Scanlon. “Alterations in Transmitral Flow Dynamics in Patients with Early Mitral Valve Closure and Aortic Regurgitation.” American Heart Journal5 (1994): 941-47.
- Rees, J. R., E. J. Epstein, J. M. Criley, and R. S. Ross. “HAEMODYNAMIC EFFECTS OF SEVERE AORTIC REGURGITATION.” Heart3 (1964): 412-21.
- Hamirani, Y. S., C. A. Dietl, W. Voyles, M. Peralta, D. Begay, and V. Raizada. “Acute Aortic Regurgitation.” Circulation9 (2012): 1121-126.
- Miller, Richard R., Louis A. Vismara, Anthony N. Demaria, Antone F. Salel, and Dean T. Mason. “Afterload Reduction Therapy with Nitroprusside in Severe Aortic Regurgitation: Improved Cardiac Performance and Reduced Regurgitant Volume.” The American Journal of Cardiology5 (1976): 564-67.
- Lefebvre, Cedric, James C. O’Neill, and David Cline. Atlas of Cardiovascular Emergencies. New York: McGraw-Hill Education, 2015.
- Smedira, Nicholas G., Magued Zikri, James D. Thomas, Michael S. Lauer, John J. Kelleman, and Patrick M. Mccarthy. “Blunt Traumatic Rupture of a Mitral Papillary Muscle Head.” The Annals of Thoracic Surgery5 (1996): 1526-528.
- Shin, Jeong Hun, Seok Hwan Kim, Jinkyu Park, Young-Hyo Lim, Hwan-Cheol Park, Sung Il Choi, Jinho Shin, Kyung-Soo Kim, Soon-Gil Kim, Mun K. Hong, and Jae Ung Lee. “Unilateral Pulmonary Edema: A Rare Initial Presentation of Cardiogenic Shock Due to Acute Myocardial Infarction.” Journal of Korean Medical Science2 (2012): 211.
- Young, Andrew L., Charles S. Langston, Robert L. Schiffman, and Michael J. Shortsleeve. “Mitral Valve Regurgitation Causing Right Upper Love Pulmonary Edema.” Texas Heart Institute Journal1 (2001): 53-56.
- Chen RS, Bivens MJ, Grossman SA. Diagnosis and Management of Valvular Heart Disease in Emergency Medicine. Emergency Medicine Clinics of North America. 2011;29(4):801-810. doi:10.1016/j.emc.2011.08.001.
- Carabello BA. Introduction to Aortic Stenosis. Circulation Research. 2013;113(2):179-185. doi:10.1161/circresaha.113.300156
- Carabello BA, Paulus WJ. Aortic stenosis. The Lancet. 2009;373(9667):956-966. doi:10.1016/s0140-6736(09)60211-7.
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(23):2440-2492. doi:10.1161/cir.0000000000000029.
- Khot UN, Novaro GM, Popović ZB, et al. Nitroprusside in Critically Ill Patients with Left Ventricular Dysfunction and Aortic Stenosis. New England Journal of Medicine. 2003;348(18):1756-1763. doi:10.1056/nejmoa022021.
- Popovic ZB. Effects of sodium nitroprusside in aortic stenosis associated with severe heart failure: pressure-volume loop analysis using a numerical model. AJP: Heart and Circulatory Physiology. 2004;288(1):H416-H423. doi:10.1152/ajpheart.00615.2004.
- Carnicelli, Anthony. “Anticoagulation for Valvular Heart Disease.” American College of Cardiology. N.p., 18 May 2015. Web. 05 Dec. 2016.
- Özkan, Mehmet, Cihangir Kaymaz, Cevat Kirma, Kenan Sönmez, Nihal Özdemir, Mehmet Balkanay, Cevat Yakut, and Ubeydullah Deligönül. “Intravenous Thrombolytic Treatment of Mechanical Prosthetic Valve Thrombosis: A Study Using Serial Transesophageal Echocardiography.” Journal of the American College of Cardiology7 (2000): 1881-889.
- Lalani, Tahaniyat. “In-Hospital and 1-Year Mortality in Patients Undergoing Early Surgery for Prosthetic Valve Endocarditis.” JAMA Internal Medicine16 (2013): 1495-503.





3 thoughts on “Acute Valvular Emergencies: Pearls and Pitfalls”
Pingback: August 2017 Asynchronous Learning – Lakeland Health EM Blog
Pingback: emDOCs.net – Emergency Medicine EducationThe EM Educator Series: The Aortic Stenosis Patient - emDOCs.net - Emergency Medicine Education
Pingback: Aortastenos – Akut översikt – Mind palace of an ER doc