
Authors: Simon Sarkisian, DO (EM Attending, Cooper University Hospital/US Army, Camden, NJ) and Zachary Sletten, MD (EM Attending, Brooke Army Medical Center) // Reviewed by: Alexander Y. Sheng MD MHPE (@TheShenger); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
A 32-year-old female presents after a high-speed motor vehicle accident in which she was the restrained driver of a car that rear ended another vehicle. The patient arrives in a c-collar complaining only of neck pain. Physical exam is remarkable for an abrasion to the left side of the neck with tenderness to palpation and swelling. What is the imaging modality of choice? What criteria might be useful to determine the next step in imaging?
What is Blunt Cerebrovascular Injury?
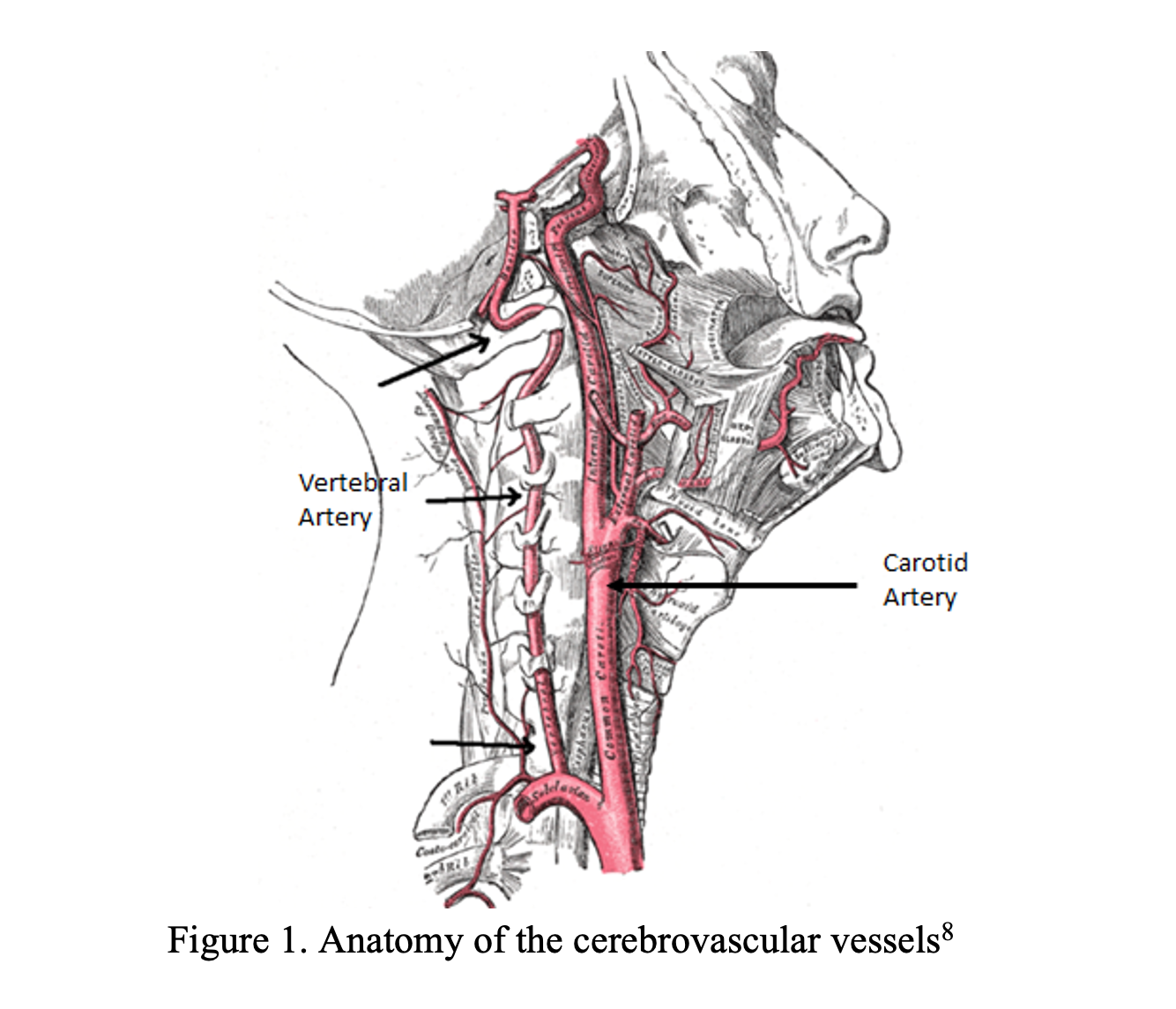
Blunt neck trauma with damage to the carotid and vertebral artery injuries are commonly referred to as blunt cerebrovascular injuries (BCVIs).
BCVI includes:
- intimal tears
- thrombosis
- dissection (commonly referred to as cervical artery dissections1)
- pseudoaneurysm2
Blunt cerebrovascular injury can result from a wide variety of causes to include major trauma along with incidents that are decidedly minor such as sneezing, coughing, sports, or chiropractic manipulation3.
BCVI results in complications after
- An intimal tear exposes subendothelial collagen and leads to either thrombus formation with arterial stenosis/occlusion or distal thromboembolism4.
- As blood dissects within the intimal walls, occlusion of the vessel may also occur.
Stroke is ultimately the most feared complication, occurring in up to 20% of BCVI patients5. Early recognition of BCVI is the key so treatment with anticoagulation or antiplatelets can be initiated to reduce the risk of stroke, long-term morbidity, and mortality6,7.
Presentation and Workup
In adults, BCVIs are rare affecting 0.8-3% of all blunt trauma patients4,9-12. In children, BCVIs are even rarer, occurring in 0.4% of blunt trauma. Reported incidence, or diagnosis, of BCVI is partly dependent on the predetermined screening criteria, such as the Denver Criteria (Table 3) and the Memphis Criteria (Table 4), which take into consideration the mechanism and associated injuries that trigger screening. Introduction of screening criteria along with advancements in imaging have improved early detection of BCVI13.
Classically BCVI occurs as a result of forced hyperextension and lateral rotation of the neck which effectively puts tension on the cervical vessels2.
- There are four types of BCVI based on mechanism (Table 1)
- The most commonly cited cause is motor vehicle collisions (MVCs)2,9,14.
- Other causes are myriad and include blunt neck trauma, intraoral trauma, basilar skull fractures, chiropractic neck manipulation, strangulation, and fractures of the spinal column.
- As noted earlier, even minor trauma can lead to BCVI, and patients may present well after the inciting event3.
Among the elderly, ground level falls account for 33% of the cases of BCVI which may argue for more vigilance in searching for the diagnosis in this scenario. The high incidence related to falls, however, is likely partially attributable to the frequency of falls for elderly patients, as only 0.15% of elderly patients who experience a ground level fall are found to have BCVI15.

Approximately 50% of patients with BCVI can be asymptomatic (no neurological deficits) at presentation, with some studies demonstrating rates as high as 76% of patients2,4,9.
- The interval from injury to neurological deficit onset typically has a latency period of 10-72 hours.
- One retrospective study of 171 patients demonstrated an average presentation time of 28 hours9.
- Another retrospective study of 492 patients with BCVI related stroke showed 63% of patients presented without neurologic deficits, with about 50% going on to be diagnosed with BCVI incidentally (on imaging) and the other 50% being diagnosed after symptom onset. About 40% of the patients did not manifest neurological symptoms until after 72 hours17.
- This latency period highlights the importance of screening for the diagnosis in patients even in the absence of neurological deficits.
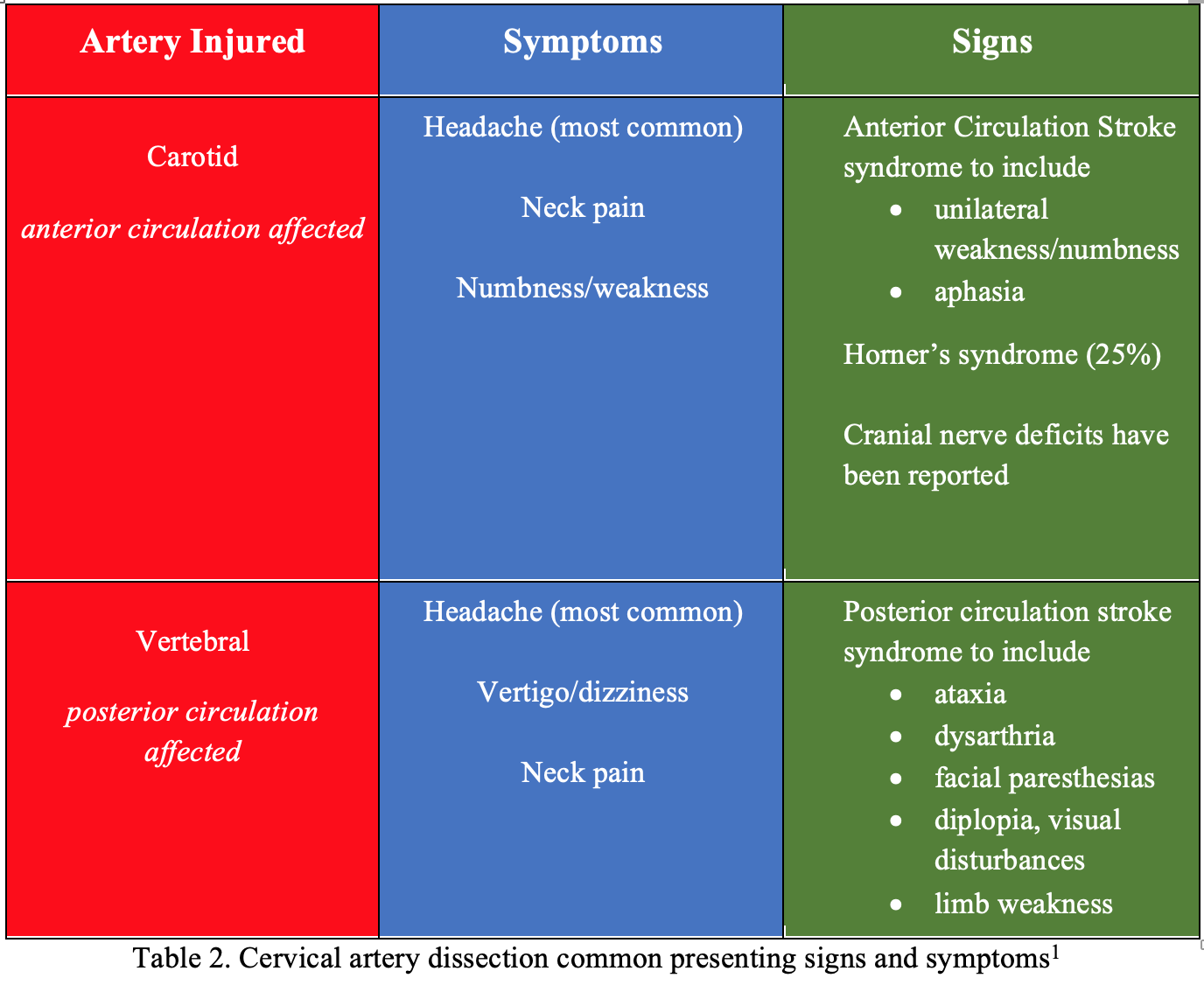
Increased detection of BCVI in asymptomatic patients in the studies performed by Biffl and his colleagues led to the development of the Denver criteria4,9,13,18. Table 2 highlights the common signs and symptoms amongst patients with dissections of either the carotid or basilar artery1 and tables 3 and 4 outline the Denver and Memphis BCVI screening criteria5.


Interestingly, a meta-analysis of nine screening criteria (most of which appear in the Denver and Memphis criteria) found that only cervical and thoracic spine injuries had a statistically significant association with BCVI19. Many injuries were lumped into generic terms (i.e. all LeFort fractures were listed under “facial fracture”). Of note, no significant associations with BCVI were observed for head injury, basilar skull fracture, cervical abrasion, neurological deficits, facial fracture, abdominal injury, and GCS < 8. Since publication of that meta-analysis, a study published in 2016 introduced five more distinct screening criteria (complex skull fractures, upper rib fractures, mandible fractures, scalp degloving, great vessel injury) which led to increased detection of BCVI and resulted in the expanded Denver Criteria (Table 3)10. To the authors’ knowledge, no studies are available comparing the Memphis Criteria to the Denver Criteria.
The EAST Guidelines recommend the use of either screening criteria (Denver or Memphis) for the detection of BCVI in adult patients with blunt polytrauma. Once the patient is determined to be high risk for BCVI by screening positive for any one of the criteria in Table 3 or Table 4:
- CTA of the neck is performed next.
- If the pre-test probability for BCVI is high and the CTA is negative, then conventional arteriography [digital subtraction angiography (DSA)], which is the gold standard, can be considered.
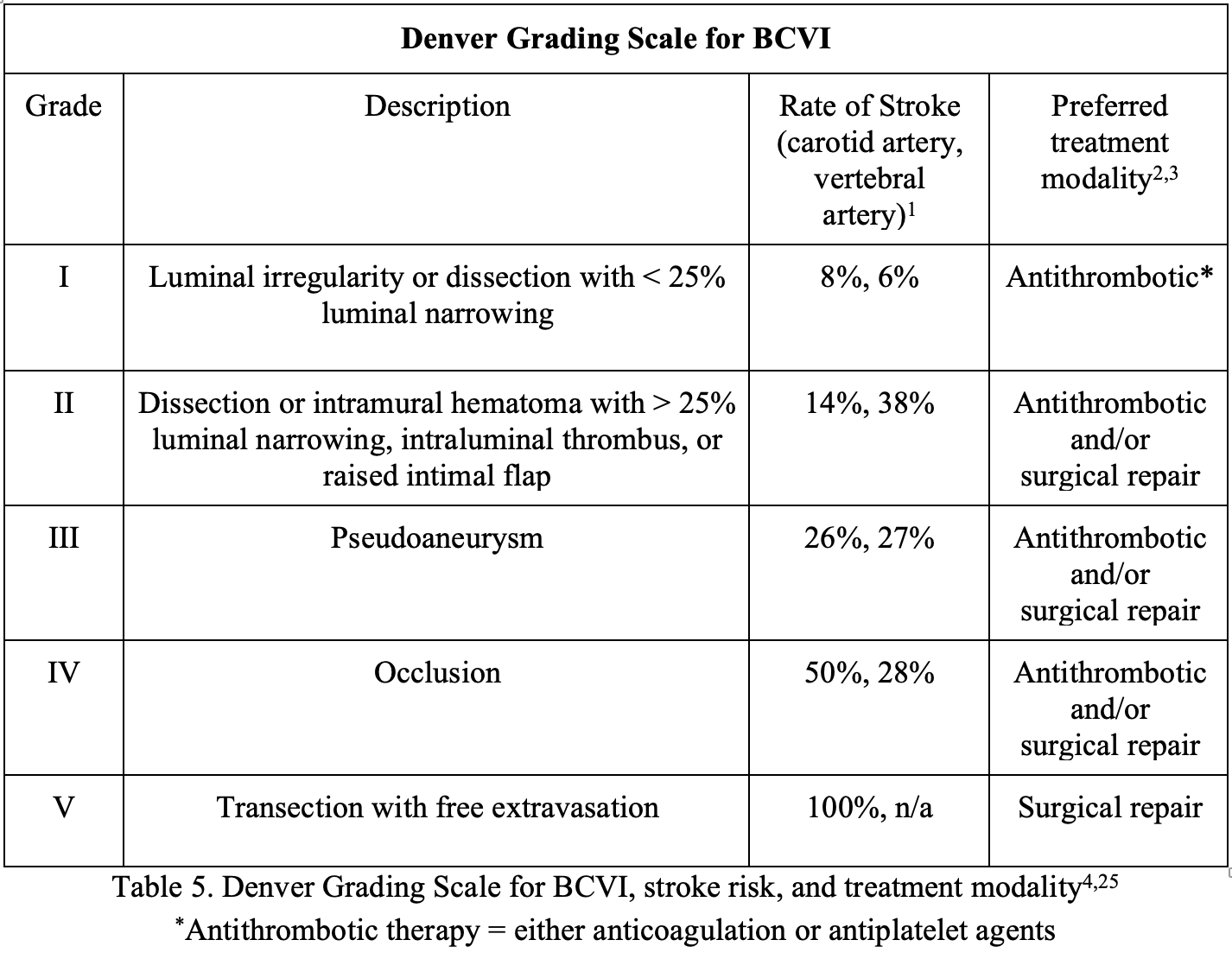
One study reported that CTA has a sensitivity of 98% and specificity of 100% for BCVI20, but a meta-analysis of over 1400 patients found that CTA has pooled sensitivity and specificity of 67% and 97% respectively compared to DSA. The reason for such a wide discrepancy remains unclear. What is known is that the DSA is invasive, often unavailable at hospitals, and can be associated with access site complications21. On the other hand, DSA can be helpful in clarifying clinically indeterminate cases, unexplained neurological findings, those planned for potential intervention, or confirming positive findings on CTA22. Although there is a study that show CTA may miss up to nearly 80% of lesions grade 2 or higher23, there are several other studies demonstrating that CTA does not miss clinically significant BCVI13. MR angiography (MRA) has been discussed as another viable diagnostic tool, but the problem is that compared to DSA, MRA has a sensitivity ranging from 50-75% and a specificity of only 67%12,18,24. Refer to Table 5 for the Denver Grading Scale for BCVI as well as the preferred treatment modality.
Complications and Management
Once a BCVI is identified the mortality can be as high as 60%, with 48-58% of survivors suffering permanent severe neurologic deficits9. One of the most feared complications occurs after a thrombus develops at the site of injury resulting in a stroke. In a study by Cothren et al, the average time to stroke of 76% of the patients with BCVI not treated with antithrombotic therapy was 75 hours. Therefore, if a BCVI is identified, then treatment choices include immediate antithrombotics and/or surgery26.
Thrombolysis within 4.5 hours with tissue plasminogen therapy (tPA) remains an important aspect of the treatment of acute ischemic stroke. However, a stroke caused by BCVI presents a few dilemmas. Namely, these types of traumatic patients present with concomitant intracranial hemorrhage, intracranial dissection, or aortic dissection which should not be treated with tPA.
Good outcomes have been reported with mechanical thrombectomy in patients with carotid artery dissection and intracranial occlusion, with or without stenting27,28. Although the recent DAWN and DEFUSE-3 trials did not specifically address large vessel occlusion due to a traumatic dissection, endovascular intervention should be considered for select patients within 24 hours of last known normal29,30. Consider neuro-interventional consultation in these cases.
Currently there are no prospective randomized studies comparing treatment strategies for BCVI. Management of BCVI is based on retrospective studies that are managed by institutional protocols. Although the quality of evidence is low, the EAST Guidelines and several retrospective studies recommend the initiation of antithrombotic therapy in the setting of BCVI in order to decrease the incidence of stroke as well as mortality5,31. The recommendations are not specific in regards to choosing between systemic anticoagulation (e.g. heparin, LMWH) or antiplatelet (e.g. aspirin, clopidogrel) agents, and there does not seem to be a difference in outcomes between these two classes of agents26,32,33. In a ten year study by Edwards et al, there was no significant difference in outcomes between BCVI patients treated with unfractionated heparin with an aPTT goal of 40 to 50 seconds and patients treated with aspirin 325 mg daily and clopidogrel 75 mg daily34. In another study at Denver Health Medical Center, patients were anticoagulated with either systemic heparin (15 U/kg per hour, without a loading dose, to achieve an aPTT between 40 and 50 seconds) or, if a contraindication to heparin existed, then aspirin 325 mg daily and clopidogrel 75 mg daily, or subcutaneous heparin (5000 U of unfractionated heparin sodium twice daily or 5000 U of dalteparin sodium daily). None of the patients in these groups ended up having a stroke35. Unfractionated heparin has the benefit of ease of reversibility and short half-life for trauma patients who may require surgical intervention22.
The benefits of anticoagulation/antiplatelet therapy need to be weighed against the risk of bleeding complications and progression of hemorrhage. What if the patient has a concomitant traumatic brain injury (TBI)? Should one continue to give anticoagulation or antiplatelet therapy? In a study of 77 patients with BCVI as well as TBI, the use of unfractionated heparin or aspirin resulted in lower stroke rates than no therapy. There was no difference in risk of hemorrhagic deterioration of traumatic brain injury based on pharmacologic treatment versus no treatment (5% vs 6% p= 0.6)36. Therefore, the decision to start antithrombotic therapy in the setting of TBI, or other hemorrhagic injuries (ie. solid organ injuries) should be made in consultation with appropriate specialists and the admitting team. A repeat CT scan in 7-10 days is often used to determine (based on resolution of injury) if antithrombotic can be discontinued or maintained for a longer period.
Surgical options include ligation, resection, thrombectomy, endovascular stent placement, or transarterial embolization. These options are limited by injury locations that are less accessible such as the carotid canals or vertebral foramen. Endovascular stents have questionable benefits with possible complications such as post-procedural stroke, stent occlusion, or procedural complications37,38. Due to poor quality of evidence as well as studies showing increased incidence of complications after stenting, the EAST Guidelines recommend against the use of routine stenting as an adjunct to antithrombotic treatment in adult patients with Grade II or III BCVIs to reduce the risk of stroke5. Ultimately, when treated appropriately either medically or surgically, strokes can be reduced from 25.8% to 3.9%39.
*Note:*
A recently released retrospective observational study including 4659 patients, of which 126 had BCVI, found screening criteria to miss a significant number of injuries40. Close to 20% of injuries were missed with screening criteria, including American College of Surgeons Trauma Quality Improvement Program Best Practices Guidelines and Denver Criteria.
Case Resolution
You correctly identify the “seat belt sign” on the patient’s neck and use the Denver criteria to determine that this patient needs a CTA of her neck to evaluate for BCVI. The CTA shows a grade I injury. Neurosurgery was consulted and recommended starting an unfractionated heparin drip. The patient was admitted and a repeat CTA in 7 days showed resolution of the injury. The patient was discharged without any adverse events.
Take Home Messages
- BCVI can occur from minor trauma and can present without neurologic deficits and/or in a delayed fashion. Consider in any patients presenting after a mechanism involving hyperextension and lateral rotation.
- There are well established clinical tools such as the Denver or Memphis criteria that assist in determining the need for a CTA of the neck in the setting of trauma.
- The major complication of BCVI is stroke from thromboembolism and treatment is generally focused on anticoagulation or antiplatelet therapy with endovascular therapy and surgery as options in select cases.
References/Further Reading
- Tintinalli JE, Ma OJ, Yealy DM, et al. Tintinalli’s emergency medicine: a comprehensive study guide. 2020.
- Walls RM, Hockberger RS, Gausche-Hill M. Rosen’s emergency medicine: concepts and clinical practice2018.
- Engelter ST, Grond-Ginsbach C, Metso TM, et al. Cervical artery dissection: trauma and other potential mechanical trigger events. Neurology 2013;80:1950-7.
- Biffl WL, Ray CE, Jr., Moore EE, et al. Treatment-related outcomes from blunt cerebrovascular injuries: importance of routine follow-up arteriography. Ann Surg 2002;235:699-706; discussion -7.
- Kim DY, Biffl W, Bokhari F, et al. Evaluation and management of blunt cerebrovascular injury: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2020;88:875-87.
- Cothren CC, Moore EE, Ray CE, Jr., et al. Screening for blunt cerebrovascular injuries is cost-effective. Am J Surg 2005;190:845-9.
- Shahan CP, Croce MA, Fabian TC, Magnotti LJ. Impact of Continuous Evaluation of Technology and Therapy: 30 Years of Research Reduces Stroke and Mortality from Blunt Cerebrovascular Injury. J Am Coll Surg 2017;224:595-9.
- Cervical Artery Dissection. 2020. (Accessed 6 SEP, 2020, at https://en.wikipedia.org/wiki/Cervical_artery_dissection.)
- Biffl WL, Moore EE, Ryu RK, et al. The unrecognized epidemic of blunt carotid arterial injuries: early diagnosis improves neurologic outcome. Ann Surg 1998;228:462-70.
- Geddes AE, Burlew CC, Wagenaar AE, et al. Expanded screening criteria for blunt cerebrovascular injury: a bigger impact than anticipated. Am J Surg 2016;212:1167-74.
- Kerwin AJ, Bynoe RP, Murray J, et al. Liberalized screening for blunt carotid and vertebral artery injuries is justified. J Trauma 2001;51:308-14.
- Miller PR, Fabian TC, Croce MA, et al. Prospective screening for blunt cerebrovascular injuries: analysis of diagnostic modalities and outcomes. Ann Surg 2002;236:386-93; discussion 93-5.
- Brommeland T, Helseth E, Aarhus M, et al. Best practice guidelines for blunt cerebrovascular injury (BCVI). Scand J Trauma Resusc Emerg Med 2018;26:90.
- Cogbill TH, Moore EE, Meissner M, et al. The spectrum of blunt injury to the carotid artery: a multicenter perspective. J Trauma 1994;37:473-9.
- Anto VP, Brown JB, Peitzman AB, et al. Blunt cerebrovascular injury in elderly fall patients: are we screening enough? World J Emerg Surg 2018;13:30.
- Blunt cerebrovascular injury: Mechanisms, screening, and diagnostic evaluation. 2020. (Accessed 6 SEP, 2020, at https://www.uptodate.com/contents/blunt-cerebrovascular-injury-mechanisms-screening-and-diagnostic-evaluation?search=blunt%20cerebrovascular%20injury&source=search_result&selectedTitle=2~11&usage_type=default&display_rank=2.)
- Burlew CC, Sumislawski JJ, Behnfield CD, et al. Time to stroke: A Western Trauma Association multicenter study of blunt cerebrovascular injuries. J Trauma Acute Care Surg 2018;85:858-66.
- Biffl WL, Ray CE, Jr., Moore EE, Mestek M, Johnson JL, Burch JM. Noninvasive diagnosis of blunt cerebrovascular injuries: a preliminary report. J Trauma 2002;53:850-6.
- Franz RW, Willette PA, Wood MJ, Wright ML, Hartman JF. A systematic review and meta-analysis of diagnostic screening criteria for blunt cerebrovascular injuries. J Am Coll Surg 2012;214:313-27.
- Eastman AL, Chason DP, Perez CL, McAnulty AL, Minei JP. Computed tomographic angiography for the diagnosis of blunt cervical vascular injury: is it ready for primetime? J Trauma 2006;60:925-9; discussion 9.
- Roberts DJ, Chaubey VP, Zygun DA, et al. Diagnostic accuracy of computed tomographic angiography for blunt cerebrovascular injury detection in trauma patients: a systematic review and meta-analysis. Ann Surg 2013;257:621-32.
- Stone DK, Viswanathan VT, Wilson CA. Management of Blunt Cerebrovascular Injury. Curr Neurol Neurosci Rep 2018;18:98.
- DiCocco JM, Emmett KP, Fabian TC, Zarzaur BL, Williams JS, Croce MA. Blunt cerebrovascular injury screening with 32-channel multidetector computed tomography: more slices still don’t cut it. Ann Surg 2011;253:444-50.
- Lévy C, Laissy JP, Raveau V, et al. Carotid and vertebral artery dissections: three-dimensional time-of-flight MR angiography and MR imaging versus conventional angiography. Radiology 1994;190:97-103.
- Screening for and Treatment of Blunt Cerebrovascular Injuires Algorithm (Accessed 10 SEP, 2020, at https://westerntrauma.org/algorithms/ScreeningForAndTreatmentOfBluntCerebrovascularInjuries/NoteF.html.)
- Cothren CC, Biffl WL, Moore EE, Kashuk JL, Johnson JL. Treatment for blunt cerebrovascular injuries: equivalence of anticoagulation and antiplatelet agents. Arch Surg 2009;144:685-90.
- Fields JD, Lutsep HL, Rymer MR, et al. Endovascular mechanical thrombectomy for the treatment of acute ischemic stroke due to arterial dissection. Interv Neuroradiol 2012;18:74-9.
- Hoving JW, Marquering HA, Majoie C. Endovascular treatment in patients with carotid artery dissection and intracranial occlusion: a systematic review. Neuroradiology 2017;59:641-7.
- Albers GW, Marks MP, Kemp S, et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N Engl J Med 2018;378:708-18.
- Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med 2018;378:11-21.
- Fabian TC, Patton JH, Jr., Croce MA, Minard G, Kudsk KA, Pritchard FE. Blunt carotid injury. Importance of early diagnosis and anticoagulant therapy. Ann Surg 1996;223:513-22; discussion 22-5.
- Markus HS, Hayter E, Levi C, Feldman A, Venables G, Norris J. Antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): a randomised trial. Lancet Neurol 2015;14:361-7.
- Markus HS, Levi C, King A, Madigan J, Norris J. Antiplatelet Therapy vs Anticoagulation Therapy in Cervical Artery Dissection: The Cervical Artery Dissection in Stroke Study (CADISS) Randomized Clinical Trial Final Results. JAMA Neurol 2019;76:657-64.
- Edwards NM, Fabian TC, Claridge JA, Timmons SD, Fischer PE, Croce MA. Antithrombotic therapy and endovascular stents are effective treatment for blunt carotid injuries: results from longterm followup. J Am Coll Surg 2007;204:1007-13; discussion 14-5.
- Cothren CC, Moore EE, Biffl WL, et al. Anticoagulation is the gold standard therapy for blunt carotid injuries to reduce stroke rate. Arch Surg 2004;139:540-5; discussion 5-6.
- Callcut RA, Hanseman DJ, Solan PD, et al. Early treatment of blunt cerebrovascular injury with concomitant hemorrhagic neurologic injury is safe and effective. J Trauma Acute Care Surg 2012;72:338-45; discussion 45-6.
- Burlew CC, Biffl WL, Moore EE, et al. Endovascular stenting is rarely necessary for the management of blunt cerebrovascular injuries. J Am Coll Surg 2014;218:1012-7.
- DiCocco JM, Fabian TC, Emmett KP, et al. Optimal outcomes for patients with blunt cerebrovascular injury (BCVI): tailoring treatment to the lesion. J Am Coll Surg 2011;212:549-57; discussion 57-9.
- Stein DM, Boswell S, Sliker CW, Lui FY, Scalea TM. Blunt cerebrovascular injuries: does treatment always matter? J Trauma 2009;66:132-43; discussion 43-4.
- Leichtle SW, Banerjee D, Schrader R, Torres B, Jayaraman S, Rodas E, Broering B, Aboutanos MB. Blunt cerebrovascular injury: The case for universal screening. J Trauma Acute Care Surg. 2020 Nov;89(5):880-886. doi: 10.1097/TA.0000000000002824




