Authors: Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) // Edited by: Jennifer Robertson, MD
Background
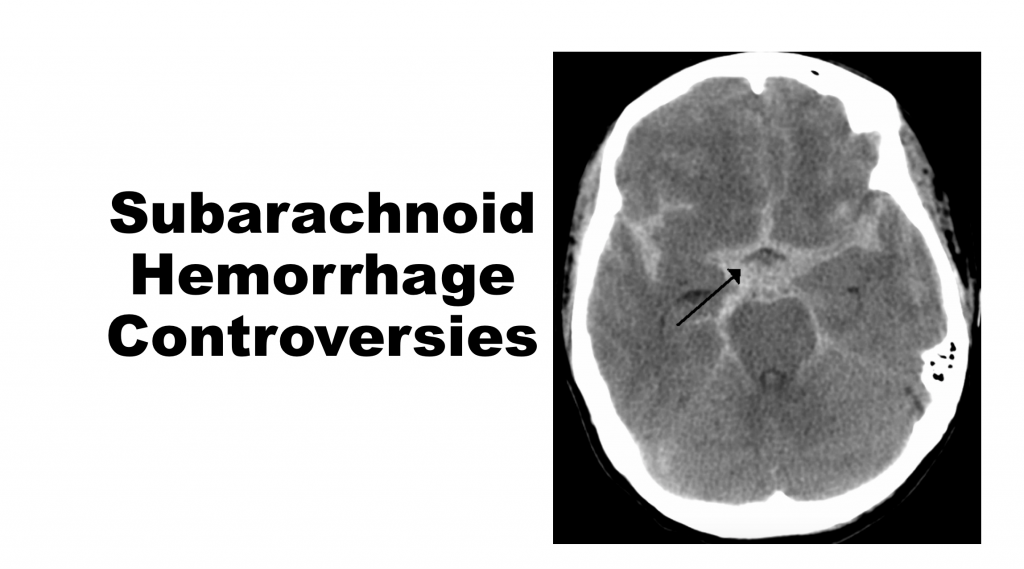
The challenge of emergency medicine is to determine if a patient has a serious and/or deadly condition, even when he or she presents with a common chief complaint. Headache is a chief complaint that accounts for 2% of emergency department (ED) visits. Subarachnoid hemorrhage (SAH) is one condition that emergency physicians must diagnose, as it is serious and potentially deadly. Accounting for 1% of headaches, SAH is most commonly due to arterial aneurysm rupture1-3. The classic presentation of SAH is a sudden, severe headache. This warning sign occurs in up to 97% of cases. Close to 85% of subarachnoid hemorrhages are non-traumatic. Approximately 80% of non-traumatic SAH are due to aneurysm rupture, while 10% are due to peri-mesencephalic hemorrhage.4-7 Risk factors for rupture include size and aneurysm location.11 One third to half of patients will experience a sentinel headache that precedes the subarachnoid hemorrhage. With 25% mortality within 2 hours of initial bleeding and 40% mortality at one week, missing this diagnosis can be deadly.16-19
How is this condition missed? 1) Failure to appreciate the clinical spectrum of SAH 2) Failure to obtain initial non-contrast head computed tomography (CT) or understand limitations in diagnosis, and 3) Failure to perform LP (lumbar puncture) and interpret results properly.20
The neurologically intact patient who presents to the ED with a headache presents several challenges. Traditionally, it has been recommended that SAH workup include a non-contrast head CT followed by LP if the initial CT is negative. 4,6,8 This recommendation has been questioned with novel imaging technology and recent literature. Multiple studies have evaluated different diagnostic strategies for subarachnoid hemorrhage including clinical decision rules (CDR), non-contrast head CT alone, combination head CT and LP, and non-contrast head CT with CT angiography (CTA).
Current Guidelines
The American College of Emergency Physicians (ACEP) Clinical Policy on acute headache retains a Level B Recommendation that “lumbar puncture is the criterion standard for diagnosing subarachnoid hemorrhage because it may detect small amounts of xanthochromia or blood in the CSF that can be missed by CT.”23 The American Heart Association has a Level B Recommendation that states “acute diagnostic workup should include a non-contrast head CT, which, if non-diagnostic, should be followed by lumbar puncture.” Level C Recommendation is given for CTA consideration in the workup of SAH.24,25
Where does this leave emergency physicians, and what patient warrants evaluation for subarachnoid hemorrhage?
Clinical Decision Rules (CDR)
Clinical decision rules are often developed to decrease testing, but CDR’s can be challenging in rare diseases, as they require sensitivities approaching 100%. Three important SAH rules include the following rules below. Each rule had 100% sensitivities in their derivative studies.2
Rule 1
Investigate if ≥ 1 high-risk finding present:
- Age ≥ 40 years
- Neck pain or stiffness
- Witnessed loss of consciousness
- Onset during exertion
Rule 2
Investigate if ≥ 1 high-risk finding present:
- Age ≥ 45 years
- Arrival by ambulance
- Vomiting (≥ 1 episodes)
- Diastolic blood pressure ≥ 100 mmHg
Rule 3
Investigate if ≥ 1 high-risk finding present:
- Age 45-55 years
- Neck pain or stiffness
- Arrival by ambulance
- Systolic blood pressure ≥ 160 mm Hg
Recently, a retrospective external validation study used each rule to measure their sensitivities.26,27 This retrospective study looked at patients with atraumatic headache and normal Glasgow Coma Scores (GCS). Sensitivities were 96% for Rule 1, 100% for Rule 2, and 89% for Rule 3. If vomiting was added, all were 100% sensitive.26,27 The original investigator completed an external validation and found sensitivities of 95-98%, and in order to increase sensitivity, the addition of thunderclap headache and limited neck flexion completed the Ottawa Subarachnoid Hemorrhage clinical decision rule, shown in Figure 1.26-28
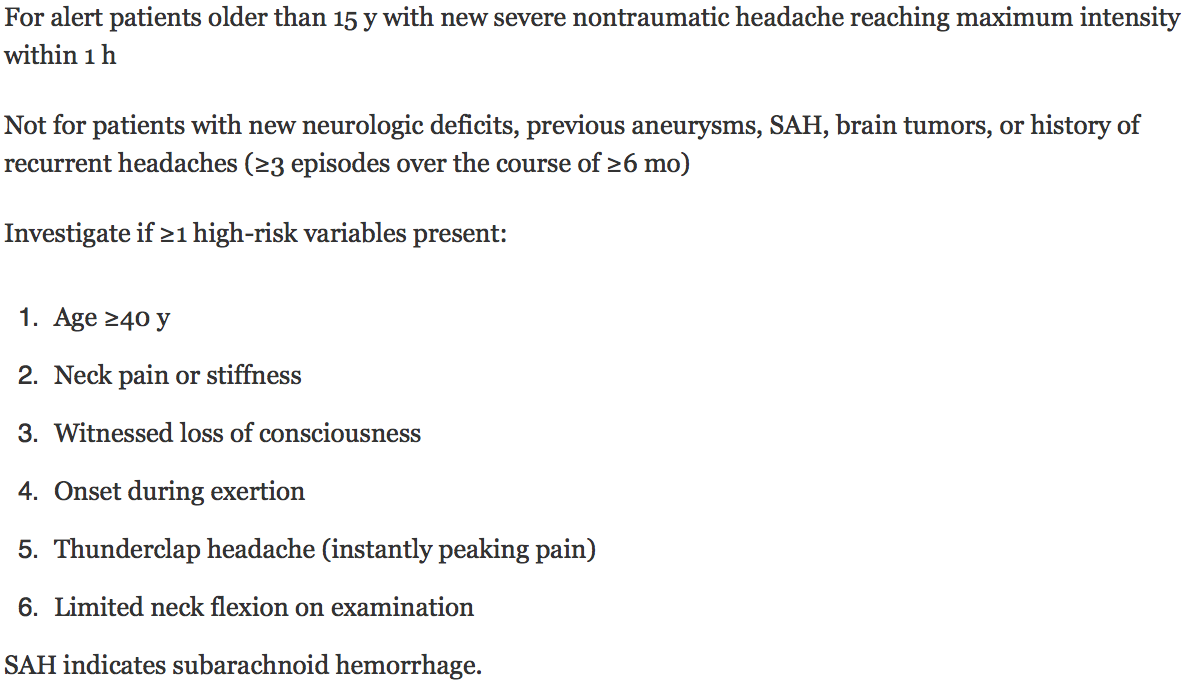
Figure 1 – Ottawa Subarachnoid Hemorrhage clinical decision ruleThe Ottawa Subarachnoid Hemorrhage (OSH) clinical decision rule demonstrated a sensitivity of 100% (with lower CI 97.2%) and 15.3% specificity. However, the OSH rule’s specificity and applicability to ED headache patients, as well as interobserver reliability, have been questioned. A second study found the rule would increase head CT/LP utilization.30 At this point, further external validation is needed but these rules do provide helpful red flags that clinicians can use when evaluating patients with headache.
Non-contrast Head CT
Much of the evaluation for SAH focuses on the non-contrast head CT, which has demonstrated increasing accuracy due to improved technology. Fifth generation scanners have sensitivities ranging from 93% to 100% depending on time from headache onset.31-35
The diagnostic accuracy of head CT is limited in several scenarios. CT scanner quality, the interpreter, and image artifacts may limit the study. Patients with hematocrit < 30% may have blood that appears isodense. Patients with normal exams and smaller hemorrhages may not demonstrate visible bleeding on the non-contrast CT. 36-38
New literature has evaluated the non-contrast head CT scan alone in evaluating for SAH within 6 hours of headache first occurrence. One prospective study evaluated 3000 patients and the sensitivity of non-contrast CT within the first 6 hours of symptoms.34,35 This study included patients with their worst ever atraumatic headache and the use of at least third generation CT scanners. Final diagnoses were all made by neuro-radiologists.
The results of this study showed non-contrast head CT to have a sensitivity and specificity of 100% for acute SAH within 6 hours of headache onset. However, after 6 hours of onset of symptoms, the sensitivity of non-contrast CT fell to 85.7%. Similarly, a 2012 study found an initial non-contrast head CT within 6 hours of headache onset to have a sensitivity of 98.5% but excluding an atypical patient, the sensitivity of non-contrast head CT was 100%. 35 Thus, this study recommends that patients with atypical presentations and presentations later than 6 hours should still receive a lumbar puncture if initial head CT is negative, as non-contrast head CT has only a sensitivity of 90% in these situations.35
In conclusion, in a patient with a sudden, severe headache with a normal neurologic exam and symptoms occurring within the prior 6 hours, the literature does support eliminating the LP if the non-contrast head CT, read by a qualified neurologist, is negative. This places patients at less than 1% risk for SAH.
Lumbar Puncture and Cerebrospinal Fluid (CSF)
Many patients present after 6 hours of headache onset, where CT sensitivity decreases to 85.7%.34 LP after a non-diagnostic CT is recommended as per ACEP clinical policy. LP can also add useful clinical data and assist in differentiating among other diagnoses.23-25 Classic LP findings in SAH include an elevated opening pressure and elevated red blood cell (RBC) count that does not diminish from tube one to four with xanthochromia.40 There are, however, limitations in the interpretation of CSF results. First, is the question of CSF RBC clearing from tube 1 to tube 4. Traumatic LP can occur in approximately 15% of studies and a clearance of zero RBC’s from tube 1 to tube 4 definitively diagnoses traumatic LP, but this is rare. Interpretation is often not as clear.41 Classically, there has been no absolute threshold for RBC cutoff or clearing in the diagnosis of SAH. One study found no patients with SAH with RBCs under 100 in tube 4. The study also found a 63% reduction in RBC from tube 1 to 4 to be the optimal threshold for clearance, but this has not been externally validated.42
LP does have several limitations, including inability to diagnosis pituitary apoplexy, cerebral venous sinus thrombosis, arterial dissection, and unruptured aneurysm. Traumatic lumbar puncture is, of course, a concern. The procedure is invasive, can be uncomfortable, and has known complications such as headache. The procedure can also be time-consuming and technically difficult in uncooperative and/or obese patients whose landmarks are difficult to find.
Xanthochromia
Xanthochromia is produced by hemoglobin product breakdown, resulting in a yellow tinge/color of the CSF. The presence of xanthochromia in the setting of SAH greatly reduces the chance of traumatic LP. Xanthochromia lasts for at least two weeks, but can take 2 to 12 hours to develop.43,44 Up to 20% of SAH patients who receive an LP within 6 hours of headache onset will have positive xanthochromia, but 100% will have its presence after 12 hours of headache occurrence.45,46
Xanthochromia is assessed by visual inspection (comparing the vial of CSF with a vial of water against a white background) or spectrophotometry. Studies have demonstrated wide variation in sensitivity of visual inspection, from 43% to 100%.41,45 Multi-wavelength spectrophotometry has recently been suggested as a superior means to detecting xanthrochromia.48 Despite the reported 100% sensitivity, it has poor specificity (29 to 75%).49,50 Additionally, less than 1% of laboratories in the U.S. contain a spectrophotometer, bringing into question this test’s applicability.44
Combination of CSF RBC and Xanthochromia
A recent study demonstrated that a combination of no xanthochromia with less than 2000 RBCs rules out SAH. This prospective cohort study enrolled patients with acute headache, and 3.5% of the cohort had SAH. Of the 1,739 patients who underwent LP (4141 total enrolled), 37% had blood or xanthochromia on LP. The vast majority were traumatic taps, as only 15 of 641 patients were actually diagnosed with SAH. The majority of false positives (74.3%) were with RBC counts of less than 100, with another 14.8% with counts between 100-1000 RBCs. A cutoff of 2000 RBCs had a sensitivity of 93%, but sensitivity was 100% with the addition of no xanthochromia. However, this threshold was retrospectively derived from the studied cohort and this should be kept in mind when considering study results.51 Additionally, the sensitivity of xanthochromia alone was 47%, consistent with prior studies.
Computed tomography angiography (CTA)
CTA is an emerging noninvasive technology. The American Heart Association (AHA) clinical policy provides a Level C Recommendation for CTA to follow a non-diagnostic head CT.24 CTA can identify, localize, and characterize a culprit aneurysm, as well as diagnose other causes of headache. One other advantage of this strategy is the ability to perform the test directly after a non-contrast head CT.
However, the sensitivities of CTA range from 77% to 100% with specificities of 87% to 100%.52-58 A decrease in sensitivity occurs with aneurysms less than 4 mm.59,60 Proponents of using CTA following non-diagnostic initial non-contrast head CT cite improved patient comfort and improved sensitivity and specificity with the combination of non-contrast head CT and CTA. Negative non-contrast head CT and a negative CTA are likely indicative of a benign clinical course. However, opponents cite a rate of 2% to 5% of the population with asymptomatic aneurysms, leading to concerns of increased neurosurgical intervention if an aneurysm is discovered.11
The current diagnostic data on CTA comes from small cohort trials. These trials compare CTA to digital subtraction angiography (DSA) in patients already diagnosed with SAH. In these studies, sensitivities range from 81% to 99%. Even the gold standard DSA can be negative in the setting of arteriospasm. Additionally, these studies do not provide data on the use of CTA for diagnosing SAH in the ED patient.
Assuming a 15% population prevalence of SAH, a recent mathematical analysis calculated the post-test probability of SAH following both negative non-contrast head CT and CTA. Ultimately, the study found a negative predictive value for CT/CTA of 99.4%. The model confidently states this is acceptable based on the number needed to complete a study comparing CT/CTA and CT/LP, where greater than 3,000 patients would be required. However, there are several negative factors with CTA. First, a negative head CT within 6 hours will more than likely be followed with a negative CTA. Second, CTA is an anatomic test that detects aneurysm, but it does not definitively state the cause of the headache. Finally, CTA also requires intravenous contrast, potentially causing allergic reaction or renal injury.61
Though the sensitivities of combination CT/CTA vary based on current data, this strategy can assist in several situations. CTA is beneficial in patients with high likelihood of SAH, obese patients, or patients where LP is not feasible (due to mental status, inability to cooperate, or patients who decline LP). CTA will consistently reveal aneurysms larger than 3mm. A negative predictive value of 99.4% is useful in a clinical setting where LP may be difficult to complete, or the patient declines LP.
The Importance of Test threshold
One important aspect of medical care is test threshold, or what is an acceptable threshold for testing and potentially missing SAH? Explained in a different manner, at what threshold does further testing do more harm than good?62,63 A miss rate of 1% in many diseases is deemed acceptable. Once this threshold of 1% is crossed, further testing may cause harm to the patient rather than providing a benefit.62,63 For a patient with headache and concern for SAH, this means that if the initial test places the risk of missing SAH at less than 1%, LP will not assist the provider and patient but may cause further harm to the patient.
A sample calculation may help provide the probability of SAH with a negative head CT.62,64 With cerebral hemorrhage accounting for 6%-7% of headaches, and an assumed non-contrast head CT sensitivity of 90%, a negative head CT provides a 0.5% chance of missed SAH. This calculation is based on high-risk patient cohorts, where approximately 4/5 patients suffered worst-ever headache, 1/3 vomiting, and 5% had loss of consciousness. If a pretest probability of 50% is used for a high risk patient, then a negative head CT with 90% sensitivity provides a post-test probability of 10%. A low risk patient with a 1% pretest probability has a 0.1% post-test probability of missed bleed with a negative non-contrast head CT. Rapid onset of headache, worst of life headache, exertional headache, syncope with headache, vomiting, and neck stiffness are red flags associated with a higher pretest probability of SAH.64
Risk and the Shared Decision Making Model
This leads to the importance of risk stratification and using a shared decision model. Many EM physicians advocate that a physician does not rule out disease, but rather, risk stratifies. Thus, a negative head CT in a patient with headache within six hours does not rule out SAH, but risk stratifies the patient to less than 1% of having SAH. The patient and physician must work as a team, with the physician presenting the information and discussing the risks/benefits of further testing if the initial CT is negative. A negative LP and CT can rule out SAH, but LP is associated with patient pain, consumption of valuable time in the ED, and potential difficulty obtaining CSF results if the patient has poor body habitus and/or cooperation.61
Using a test threshold of less than 1% and head CT within 6 hours has literature support to be used in a shared decision model. For higher risk patients with red flags on history/exam or the patient presenting after 6 hours, discussion should be done with the patient regarding further testing.
What about current ACEP Clinical Policy? Dr. Edlow, one of the editors for the official policy, states that the EM practice should change in that the neurologically intact patient with a sudden, severe headache who undergoes a non-contrast head CT within 6 hours of headache onset no longer requires LP.65
Summary
Subarachnoid hemorrhage is a deadly disease and can present in a variety of ways, most commonly sudden, severe headache. Multiple diagnostic regimens exist, including non-contrast CT only, CT/LP, and CT/CTA. Many of these pathways have significant controversy. Within 6 hours of headache onset, a CT only approach does have literature support for risk stratifying patients to less than 1% risk of SAH. However, after 6 hours, the sensitivity of non-contrast head CT decreases. A test threshold of 1% does seem acceptable currently. Ultimately, a shared decision making model should be followed.
References/Further Reading:
1. Ingall T, Asplund K, Mahonen M, et al. A multinational comparison of subarachnoid hemorrhage epidemiology in the WHO MONICA stroke study. Stroke 2000;31(5):1054-1061.
2. Kozak N, Hayashi M. Trends in the incidence of subarachnoid hemorrhage in Akita Prefecture, Japan. J Neurosurg 2007;106(2):234-238.
3. King JT, Jr. Epidemiology of aneurysmal subarachnoid hemorrhage. Neuroimaging Clin N Am 1997;7(4):659-668.
4. Edlow JA, Malek AM, Ogilvy CS. Aneurysmal subarachnoid hemorrhage: update for emergency physicians. J Emerg Med 2008;34(3):237-251.
5. Fukuda T, Hasue M, Ito H. Does traumatic subarachnoid hemorrhage caused by diffuse brain injury cause delayed ischemic brain damage? Comparison with subarachnoid hemorrhage caused by ruptured intracranial aneurysms. Neurosurgery 1998;43(5):1040-1049.
6. Suarez JI, Tarr RW, Selman WR. Aneurysmal subarachnoid hemorrhage. N Engl J Med 2006;354(4):387-396.
7. Watanabe A, Hirano K, Kamada M, et al. Perimesencephalic nonaneurysmal subarachnoid haemorrhage and variations in the veins. Neuroradiology 2002;44(4):319-325.
8. van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet 2007;369(9558):306-318.
9. Heiskanen O. Ruptured intracranial arterial aneurysms of children and adolescents. Surgical and total management results. Childs Nerv Syst 1989;5(2):66-70.
10. Stehbens WE. Etiology of intracranial berry aneurysms. J Neurosurg 1989;70(6):823-831.
11. Rinkel GJ, Djibuti M, Algra A, et al. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke 1998;29(1):251-256.
12. Linn FH, Wijdicks EF, van der Graaf Y, et al. Prospective study of sentinel headache in aneurysmal subarachnoid haemorrhage. Lancet 1994;344(8922):590-593.
13. Landtblom AM, Fridriksson S, Boivie J, et al. Sudden-onset headache: a prospective study of features, incidence and causes. Cephalalgia 2002;22(5):354-360.
14. Morgenstern LB, Luna-Gonzales H, Huber JC Jr, et al. Worst headache and subarachnoid hemorrhage: prospective, modern computed tomography and spinal fluid analysis. Ann Emerg Med 1998;32(3 Pt 1):297-304.
15. Gorelick PB, Hier DB, Caplan LR, Langenberg P. Headache in acute cerebrovascular disease. Neurology 1986;36:1445.
16. Hop JW, Rinkel GJ, Algra A, et al. Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke 1997;28(3):660-664.
17. Neil-Dwyer G, Lang D. ‘Brain attack’–aneurysmal subarachnoid haemorrhage: death due to delayed diagnosis. J R Coll Physicians Lond 1997;31(1):49-52.
18. Broderick JP, Brott TG, Duldner JE, et al. Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke 1994;25(7):1342-1347.
19. Feigin VL, Lawes CM, Bennett DA, et al. Stroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol 2003;2(1):43-53.
20. Edlow JA, Caplan LR. Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. N Engl J Med 2000;342:29.
21. Harling DW, Peatfield RC, Van Hille PT, et al. Thunderclap headache: is it migraine? Cephalalgia 1989;9(2):87-90.
22. Linn FH, Rinkel GJ, Algra A, et al. Headache characteristics in subarachnoid haemorrhage and benign thunderclap headache. J Neurol Neurosurg Psychiatry 1998;65(5):791-793.
23. Edlow JA, Panagos PD, Godwin SA, et al. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with acute headache. Ann Emerg Med 2008;52(4):407-436.
24. Connolly ES, Jr., Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012;43(6):1711-1737.
25. Bederson JB, Connolly ES, Jr., Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 2009;40(3):994-1025.
26. Perry JJ, et al. Clinical decision rules to rule out subarachnoid hemorrhage for acute headache. JAMA 2013 Sep 25;310(12):1248-55.
27. Kelly AM, et al. Sensitivity of proposed clinical decision rules for subarachnoid haemorrhage: An external validation study. Emerg Med Australas. 2014 Dec;26(6):556-60.
28. Perry JJ, Stiell IG, Sivilotti ML, et al. High-risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study. BMJ 2010 Oct 28;341:c5204.
29. Bellolio MF, Hess EP. External validation of the Ottawa subarachnoid hemorrhage clinical decision rule in patients with acute headache. Am J Emerg Med 2015 Feb;33(2):244-9.
30. Matloob SA, Roach J, Marcus HJ, et al. Evaluation of the impact of the Canadian subarachnoid haemorrhage clinical decision rules on British practice. Br J Neurosurg 2013;27(5):603- 606.
31. Sames TA, Storrow AB, Finkelstein JA, et al. Sensitivity of new-generation computed tomography in subarachnoid hemorrhage. Acad Emerg Med 1996;3(1):16-20.
32. Boesiger BM, Shiber JR. Subarachnoid hemorrhage diagnosis by computed tomography and lumbar puncture: are fifth generation CT scanners better at identifying subarachnoid hemorrhage? J Emerg Med 2005;29(1):23-27.
33. Byyny RL, Mower WR, Shum N, et al. Sensitivity of non-contrast cranial computed tomography for the emergency department diagnosis of subarachnoid hemorrhage. Ann Emerg Med 2008;51(6):697-703.
34. Perry JJ, Stiell IG, Sivilotti ML, et al. Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. BMJ 2011;343:d4277.
35. Backes D, Rinkel GJ, Kemperman H, et al. Time-dependent test characteristics of head computed tomography in patients suspected of nontraumatic subarachnoid hemorrhage. Stroke 2012;43(8):2115-2119.
36. van der Wee N, Rinkel GJ, Hasan D, et al. Detection of subarachnoid haemorrhage on early CT: is lumbar puncture still needed after a negative scan? J Neurol Neurosurg Psychiatry 1995;58(3):357-359.
37. Leblanc R. The minor leak preceding subarachnoid hemorrhage. J Neurosurg 1987;66(1):35-39.
38. Schriger DL, Kalafut M, Starkman S, et al. Cranial computed tomography interpretation in acute stroke: physician accuracy in determining eligibility for thrombolytic therapy. JAMA 1998;279(16):1293-1297.
39. Mark DG, Hung YY, Offerman SR, et al. Nontraumatic subarachnoid hemorrhage in the setting of negative cranial computed tomography results: external validation of a clinical and imaging prediction rule. Ann Emerg Med 2013;62(1):1-10.
40. Schievink WI, Wijdicks EF, Meyer FB, et al. Spontaneous intracranial hypotension mimicking aneurysmal subarachnoid hemorrhage. Neurosurgery 2001;48(3):513-516.
41. Dupont SA, Wijdicks EF, Manno EM, et al. Thunderclap headache and normal computed tomographic results: value of cerebrospinal fluid analysis. Mayo Clin Proc 2008;83(12):1326-1331.
42. Czuczman AD, Thomas LE, Boulanger AB, et al. Interpreting red blood cells in lumbar puncture: distinguishing true subarachnoid hemorrhage from traumatic tap. Acad Emerg Med 2013; 20:247.
43. Barrows LJ, Hunter FT, Banker BQ. The nature and clinical significance of pigments in the cerebrospinal fluid. Brain 1955;78(1):59-80.
44. Edlow JA, Bruner KS, Horowitz GL. Xanthochromia. Arch Pathol Lab Med 2002;126(4):413-415.
45. Vermeulen M, Hasan D, Blijenberg BG, et al. Xanthochromia after subarachnoid haemorrhage needs no revisitation. J Neurol Neurosurg Psychiatry 1989;52(7):826-828.
46. Walton J. Subarachnoid Hemorrhage. Edinburgh, Scotland: E & S Livingstone Ltd; 1956.
47. Arora S, Swadron SP, Dissanayake V. Evaluating the sensitivity of visual xanthochromia in patients with subarachnoid hemorrhage. J EmergMed 2010;39:13–16.
48. Petzold A, Keir G, Sharpe TL. Why human color vision cannot reliably detect cerebrospinal fluid xanthochromia. Stroke 2005 Jun;36(6):1295-1297.
49. Wood MJ, Dimeski G, Nowitzke AM. CSF spectrophotometry in the diagnosis and exclusion of spontaneous subarachnoid haemorrhage. J Clin Neurosci 2005;12(2):142-146.
50.
Perry JJ, Sivilotti ML, Stiell IG, et al. Should spectrophotometry be used to identify xanthochromia in the cerebrospinal fluid of alert patients suspected of having subarachnoid hemorrhage? Stroke 2006;37(10):2467-2472.
51. Perry JJ, et al. Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study. BMJ 2015 Feb 18;350:h568.
52. Brisman JL, Song JK, Newell DW. Cerebral aneurysms. N Engl J Med 2006;355(9):928-939.
53. Agid R, Lee SK, Willinsky RA, et al. Acute subarachnoid hemorrhage: using 64-slice multidetector CT angiography to “triage” patients’ treatment. Neuroradiology 2006;48(11):787- 794.
54. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke 2000;31(11):2742-2750.
55. Dammert S, Krings T, Moller-Hartmann W, et al. Detection of intracranial aneurysms with multislice CT: comparison with conventional angiography. Neuroradiology 2004;46(6):427-434.
56. Uysal E, Yanbuloglu B, Erturk M, et al. Spiral CT angiography in diagnosis of cerebral aneurysms of cases with acute subarachnoid hemorrhage. Diagn Interv Radiol 2005;11(2):77- 82.
57. White PM, Teasdale EM, Wardlaw JM, et al. Intracranial aneurysms: CT angiography and MR angiography for detection prospective blinded comparison in a large patient cohort. Radiology 2001;219(3):739-749.
58. White PM, Wardlaw JM, Easton V. Can noninvasive imaging accurately depict intracranial aneurysms? A systematic review. Radiology 2000;217(2):361-370.
59. Dammert S, Krings T, Moller-Hartmann W, et al. Detection of intracranial aneurysms with multislice CT: comparison with conventional angiography. Neuroradiology 2004;46(6):427-434.
60. Anderson GB, Findlay JM, Steinke DE, et al. Experience with computed tomographic angiography for the detection of intracranial aneurysms in the setting of acute subarachnoid hemorrhage. Neurosurgery 1997;41(3):522-527.
61. McCormack RF, Hutson A. Can computed tomography angiography of the brain replace lumbar puncture in the evaluation of acute-onset headache after a negative noncontrast cranial computed tomography scan? Acad Emerg Med 2010;17(4):445-451.
62. David Newman, MD. LP for Subarachnoid Hemorrhage: The 700 Club. EP Monthly. December 4, 2012.
63. Perry JJ, Eagles D, Clement CM, et al. An international study of emergency physicians’ practice for acute headache management and the need for a clinical decision rule. CJEM 2009;11(6):516-522.
64. Newman D. Risk Assessment: High-Risk Headache in the Emergency Department. The NNT. September 21, 2010. http://www.thennt.com/risk/high-risk-headache-in-the-emergency-department/
65. Edlow JA, Fisher J. Diagnosis of subarachnoid hemorrhage: time to change the guidelines? Stroke 2012 Aug;43(8):2031-32.





3 thoughts on “Controversies in the Diagnosis of Subarachnoid Hemorrhage”
A brilliant review!!
Pingback: THUNDERCLAP HEADACHE – PEARLS AND PITFALLS – Luis Vargas MD.
Pingback: SAH: Should we CT, CTA or LP? – edhsredu