Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan, Dr. Jacob Avila, and CORE EM on twitter at @EMSwami , @UltrasoundMD and @Core_EM
Written by Anand Swaminathan, MD and Edited by Jacob Avila, MD
Definition:
- Delivery of a local anesthetic agent to a peripheral nerve in the forearm with the goal of achieving anesthesia to facilitate performance of a procedure.
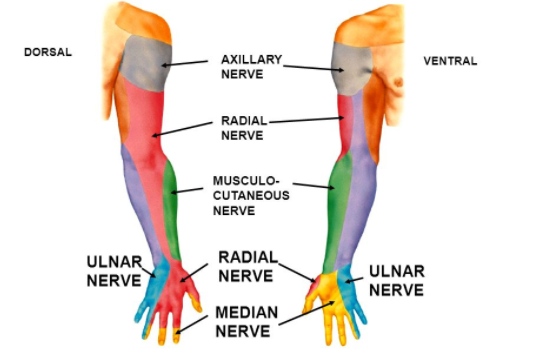
Upper Extremity Neurovascular Anatomy
Risk + Benefits
Benefits
- Potential to achieve complete anesthesia of the hand
- Doesn’t require local infiltration of wound
- Absence of systemic side effects if performed properly
- Can be rapidly performed using direct visualization with ultrasound
Risks/Limitations
- Does not provide analgesia to the wrist and distal forearm
- Potential to inadvertently injure anatomically related vascular structures
- Systemic toxicity of anesthetic agent possible if injected into vein or artery
Complications
- Vascular puncture and intravascular drug delivery
- Neural trauma
- Intraneural injection (pain or parasthesia during injection)
- Infection
- Hematoma
Common Indications
- Lacerations
- Abscess I+D
- Metacarpal and phalangeal fractures and dislocations (ulnar nerve block is particularly good for 5th metacarpal fractures but the radian and median nerve blocks give variable bony anesthesia limiting their utility)
Note: Forearm nerve blocks do not provide anesthesia to the volar surface of the forearm and wrist due to innervation of these regions by cutaneous nerves (i.e. musculocutaneous nerve)
Common Local Anesthetics
|
Agent |
Duration of Action (minutes) |
Max Dose |
|
Lidocaine |
30 – 60 |
4.5 mg/kg (max 300 mg) |
|
Lidocaine with Epinephrine |
120 – 360 |
7 mg/kg (max 500 mg) |
|
Bupivacaine |
120 – 240 |
2 mg/kg (max 175 mg) |
|
Bupivacaine with Epinephrine |
180 – 420 |
3 mg/kg (max 225 mg) |
Radial Nerve Block
- Relevant Anatomy
- Course of radial nerve is radial to the radial artery
- Further up the forearm, there is increased separation between the radial nerve and artery
- Of the three forearm blocks, this one is the most difficult as the nerve is the smallest of the three
- Sensory Distribution: Dorsum of the hand and wrist
- Radial aspect of the dosrum of the hand
- Dorsum of the thumb, index finger, long finger and 1/2 of the ring finger proximal to the distal interphalangeal (DIP) joint
- Block Technique Basics
- Use standard sterile preparation
- Ideal location for block
- Mid to upper forearm
- Radial artery and nerve separate making block technically easier
- Approach to block at the wrist may not be effective
- At wrist, superficial radial nerve splits into multiple sensory branches
- If block delivered distal to division, may not fully anesthetize region
- “Blind” technique
- Palpate radial artery
- Inject local anesthetic radial to where artery palpated
- Disadvantages
- Unable to directly confirm delivery of anesthetic agent
- Difficult to perform block above wrist (difficult to palpate artery above this area)
- US Guided Block
- Superior to “blind” technique as offers direct visualization of nerve and needle
- Perform block using “in-plane” orientation to allow best visualization of nerve and needle
Ulnar Nerve Block
- Relevant Anatomy
- Course of ulnar nerve is ulnar to the ulnar artery
- Further up the forearm, there is increased separation between the ulnar nerve and artery
- Sensory distribution
- Ulnar portion of the dorsum of hand, 5th digit and ulnar aspect of the ring finger
- Hypothenar eminence
- Block Technique Basics
- Use standard sterile preparation
- Ideal location for block
- Mid to upper forearm
- Ulnar artery and nerve separate making block technically easier
- “Blind” technique
- Palpate the ulnar artery
- Inject local anesthetic ulnar to where artery palpated
- Disadvantages
- Unable to directly confirm delivery of anesthetic agent
- Ulnar artery often difficult to palpate
- US Guided Block
- Superior to “blind” technique as offers direct visualization of nerve and needle
- Perform block using “in-plane” orientation to allow best visualization of nerve and needle
Median Nerve Block
- Relevant Anatomy
- Runs through middle of volar surface of forearm and deep to the carpal tunnel at the wrist
- Does not traverse arm alongside a major artery unlike the radial and ulnar nerves
- Sensory distribution
- Volar surface of the palm and thumb, index finger, long finger and 1/2 of the ring finger
- Dorsal surface of the thumb, index finger, long finger and 1/2 of the ring finger distal to the DIP joint
- Block Technique Basics
- Use standard sterile preparation
- Ideal location for block dependent on technique used
- “Blind” technique
- Locate the palmaris longus (PL) and the flexor carpi radialis (FCR) tendons at the wrist
- The median nerve runs in between these the PL and FCR tendons
- Insert needle to a depth of 3-5 mm and inject local anesthetic
- US Guided Block
- Superior to “blind” technique as offers direct visualization of nerve and needle
- Locate nerve at wrist and track proximally to mid to upper forearm
- Perform block using “out-of-plane” orientation
- Easiest to identify needle “in-plane”
- Most direct route to reach nerve via anterior approach which must be done “out-of-plane”
Take Home Points
- Forearm nerve blocks are relatively easy to perform and deliver excellent regional anesthesia to the hand without systemic side effects
- Successful utilization of nerve blocks requires an intimate understanding of anatomical relationships and motor/sensory supply. Nerve blocks are made easier by employing ultrasound
- There are a host of indications for forearm nerve blocks including lacerations, fractures and need for incision and drainage
Read More
5 Minute Sono: Radial Nerve Block
5 Minute Sono: Median Nerve Block
5 Minute Sono: Ulnar Nerve Block
Ultrasound Podcast: Upper Extremity Nerve Block Mastery with Mike Stone





