Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Written by Ashley Miller, MD and Edited by Anand Swaminathan, MD
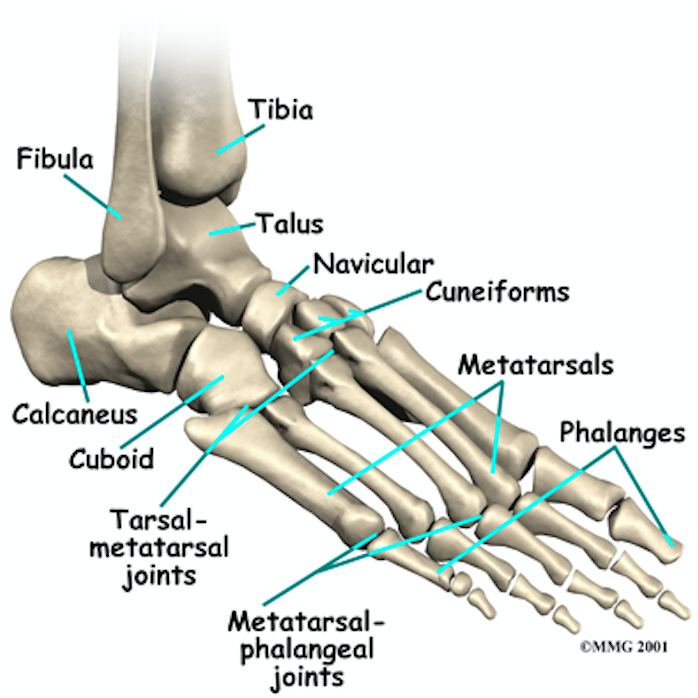
Definition: A rare ankle injury that occurs with disruption of the talo-navicular and talocalcaneal joints. Not to be confused with “ankle” (tibio-talar) dislocation
Role of Subtalar Joint
- Provides shock absorption
- Permits foot to adjust to uneven ground (such as walking on sand)
Mechanism:
- High energy trauma
- Fall from height
- Motor vehicle accident
- Plantar flexed-foot (foot lands on ground while inverted or everted)

Subtalar Dislocation (orthobullets.com)
Classification/Physical Exam
- Open (up to 25%) vs. Closed
- Medial: ~60-80% (Weatherford, Yoder 2011)
- Inversion injury
- Foot locked in plantar flexion and supinated (Menkes 2000)
- Sometimes referred to as “basketball foot”as it is seen when basketball players land after jumping) (Yoder 2011)
- Head of talus prominent dorsolaterally
- Lateral
- Eversion injury
- Foot locked in pronation
- Because of surrounding anatomical structures, lateral dislocation requires more force; thus, more frequently open and/or associated with other injuries (Yoder 2011)
- Calcaneus is displaced lateral to talus
- Anterior (from hyperextension) /Posterior (from hyperflexion)
- Much less common (< 5% of all dislocations) (DeLee 1982)

Medial Subtalar Dislocation (West JEM)
Diagnostic Imaging
- Dislocations will be clear on plain radiographs
- X-ray
- Obtain AP and lateral views of foot and ankle
- Medial Dislocation: talar head superior to navicular on lateral image
- Lateral Dislocation: talar head colinear or inferior to navicular bone on lateral image, non-distinguishable subtalar joint
- Complete a primary and secondary trauma survey looking for additional injuries
- Assess neurovascular status and perform skin exam
- Provide analgesia
- Consider early consultation with orthopedics
- These dislocations are often much more difficult to reduce than standard ankle dislocations (tibio-talar dislocations)
- Up to 32% of subtalar dislocations require open reduction (Bibbo 2003)
- Medial reduction can be blocked by capsule of talonavicular joint and extensor digitorum brevis, deep peroneal neurovascular bundle, talar head can “buttonhole” through the extensor digitorum brevis, or impaction can occur on navicular
- Lateral reduction can be blocked by posterior tibial tendon (most common), impaction fractures, or other tendons
- Reduction Approach
- Standard ankle reduction techniques can lead to further injury and morbidity
- Flex the patient’s knee (90 degrees) and hip to reduce tension on the gastrocnemius and hold counter-traction (you may require an assistant for this)
- Place the ankle in plantar flexion
- For MEDIAL dislocations, grasp calcaneus with dominant hand, dorsum of foot with opposite hand, for LATERAL dislocations, do the same but also place non-dominant thumb over navicular
- Distract the hindfoot and apply direct pressure to talar head while inverting vs. everting to exaggerate the deformity
- If patient is inverted (medial dislocation), hyper-invert
- If patient is inverted everted (lateral dislocation), hyper-evert
- Subsequently reverse the direction of dislocation (Thompson 2011)
- Post-Reduction
- Post-reduction X-rays
- Confirm proper alignment
- Evaluate for osteochondral lesions (injuries and/or small fractures of cartilage surface of talus), compression fractures, and other injuries of ankle/foot
- Consider post-reduction CT scan (Yoder 2011, Bibbo 2003)
- Concomitant foot/ankle injuries are common (88-100%)
- These injuries may be missed on plain radiographs
- CT findings may change management and may affect outcomes
- Optimal time to obtain CT scan (ED vs as outpatient) is unknown
- Short leg cast, non-weight bearing for 3-6 weeks (may consider short leg posterior/AO splint in ED after reduction for presumed swelling with close ortho follow up to transition to cast) (DeLee JC 1982)
- Post-reduction X-rays
Complications
-
- Post-Traumatic Arthritis
- Small number of subtalar fusions
- Lateral dislocations typically fare worse (as above, higher-energy mechanism, more frequent concomitant injuries)
- Infection with open wounds
Take Home Points:
- Subtalar dislocations are a rare injury, but are much more likely to require operative reduction than tibio-talar (standard ankle) dislocations
- Consider early orthopedic consultation as the success rate of closed reduction is relatively low
- Consider post-reduction CTs to evaluate for other injuries as the incidence of these are relatively high
Read More
Menkes, J: Injuries to Bones, Joints, and Soft Tissues. In J.E. Tintinalli, G. Kelen, & J.S. Stapcyznski (Eds.), Emergency Medicine ed. 5. McGraw-Hill 2000
OrthoBullets: Subtalar Dislocation Video
Radiopaedia: Peritalar Dislocation
Physiopedia: Subtalar Dislocation
References:
Weatherford, B. (2017, August 27). Subtalar Dislocations.[Orthobullets]. Link
Yoder et al. Talocalcaneal Navicular Dislocations: a Review. Chapter 11. 49-55. Link
DeLee JC. Subtalar dislocation of the foot. J Bone Joint Surg A. 1982; 64(3):433-437. PMID: 7061560
Bibbo et al. Injury characteristics and the clinical outcome of subtalar dislocations: a clinical and radiographic analysis of 25 cases. Foot Ankle Int. 2003. 24(2):158-63. PMID 12627624
Thompson S, Zlotolow D. Handbook of Splinting and Casting. Elsevier Health Sciences. 2011. 111-114.






1 thought on “CORE EM: Subtalar Dislocation”
Interesting post. In France we consider reduction extremely time sensitive in this case and don’t recommend xrays before reduction. If reduction is delayed, skin will be damaged and could postpone surgery by several days. Any comments?