Author: Diana Kay Coleman, MD (EM Resident Physician, UTSW / Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician at SAUSHEC)
An elderly patient presents to your emergency department with his adult son who is concerned that his father is acting more and more confused. This is not a new behavior for the patient; the son has noticed it over the past several years. He will repeat questions and not remember significant events from the past few days. Over the past several months he has even become “stubborn” according to the son, often yelling when his family members try to correct him. The only other symptom the patient’s son has noticed is that for the past several months, the patient moves around much more slowly, often needing assistance to walk to the bathroom. He has had many accidents of urinating on himself when he doesn’t get to the bathroom in time. The patient has never been to your hospital before – in fact he moved to the U.S. with his son from Africa 1 year ago, so you have no past medical history, and the patient has not seen a physician in years. The son asks you why his father is acting in this manner and how you can fix it, as he doesn’t think he can take care of his father like this anymore.
Dementia versus Delirium
Differentiating dementia and delirium can be a difficult but important distinction to make in the emergency department, and the best tool to help differentiate the two disease processes is the history. The catch is that both dementia and delirium make for poor patient historians. You will need to rely on family or friends, nursing home staff or home health aids who may have been assisting the patient, and any prior records.
Symptoms of delirium can overlap the symptoms of dementia, but there are some clues that lead more towards a diagnosis of delirium. Patients with delirium will have disturbances in consciousness, memory, cognition, and perception. These patients may develop hallucinations or delusions. Their presentation can vary from hyperactive and agitated to hypoactive and lethargic, or a category of mixed delirium which includes characteristics of both. Studies show that up to 60% of critically ill patients with delirium will present with hypoactive symptoms[i].
In contrast, patients suffering from dementia are more likely to have predominantly impairments in memory and cognitive function, as opposed to alterations in consciousness and perception. For patients with delirium, their symptoms present much more acutely, over days to weeks, as opposed to the symptoms of dementia, which occur over months and years. Patients with delirium are also much more likely to have a fluctuating course, with symptoms changing abruptly over the course of days, or even hours.
Using laboratory tests and imaging as adjuncts can help delineate between these two disease processes. Delirium will usually be accompanied by some lab or imaging abnormality indicating the cause, such as an electrolyte disturbance, a source of infection, or an intoxicant. Identifying if your patients’ symptoms are caused by dementia or delirium is important because most causes of delirium are reversible. There are many mnemonics to help remember the common causes of delirium. Two different mnemonics are[ii][iii]:

Reversible Causes of Dementia
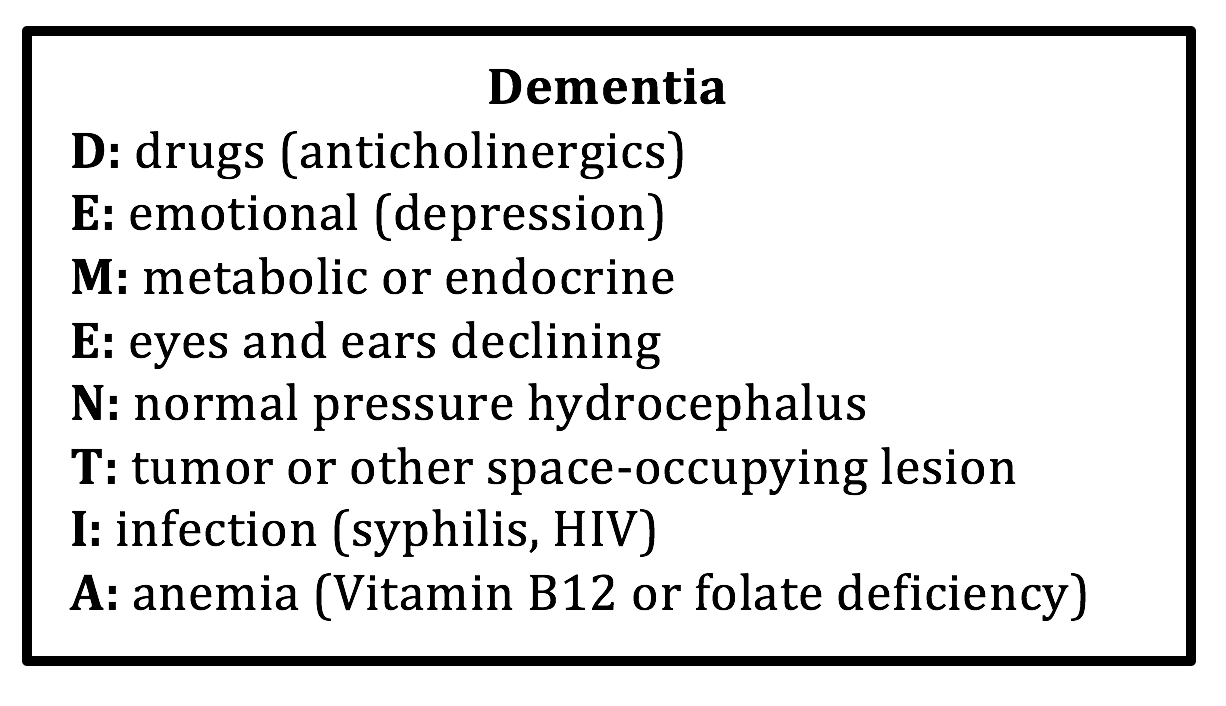
After your initial history has pointed you in the direction of dementia as a cause of your patient’s symptoms, the next step is to determine if your patient has a reversible cause of dementia. The frequency of dementia due to a potentially reversible cause is varied, with reports of anywhere between 0 to 23% of cases being attributed to a reversible cause. The most common reversible causes are alcohol and medication related dementia, depression induced cognitive impairment, surgical brain lesions (normal pressure hydrocephalus, tumors, chronic subdural hematomas), metabolic disorders, vitamin deficiencies, and CNS infections such as neurosyphilis and HIV[iv]. It is important to note that some of those causes, such as drug reactions, metabolic abnormalities, or endocrine derangements can cause either an acute delirium or a gradual progressive dementia[v]. Below is a helpful mnemonic to remember the reversible causes of dementia:
When evaluating a patient with symptoms of dementia, keep in mind that not all reversible forms of dementia can be diagnosed in the emergency department, let alone treated in the emergency department. For example, a patient in whom you suspect decline in hearing as a cause for dementia will likely require a formal outpatient audiology evaluation. Depending on your facility, an HIV test or RPR or VDRL test to evaluate for syphilis might not result that same day, so the diagnosis might be delayed until the patient has left your emergency department. However, there are some basic labs and imaging that you can order to rule out the common reversible causes of dementia, and you can add other adjunct based on the relevant information from your history and physical exam.
Evaluation of a Patient with Symptoms of Dementia
A focused history in these patients may be all that is needed to point in the direction of a particular etiology of dementia, such as a patient reporting a long history of alcohol abuse prior to symptom onset, or a patient with multiple prior strokes who can be diagnosed with vascular dementia. However, not all cases are straight forward. A thorough history should be obtained regarding the cognitive symptoms, including symptom onset, severity of decline, association with potential emotional stressors, and any other physical complaints that have developed since the symptom onset. Be sure to include a thorough past medical history, including family history of similar symptoms, social history including prior drug or alcohol use, and a complete list of medications, including over-the-counter drugs or vitamins. Asking about prior history of depression or recent changes in mood may provide helpful clues to assess for pseudodementia secondary to depression.
Dementia due to drug toxicity can be a difficult entity to diagnose as well as to treat – particularly in elderly patients – for many reasons. These patients often have multiple prescribed drugs, and it is hard to determine which drug might be the offender. It is rare that dementia is caused solely by a single drug side effect or drug toxicity, but rather many drugs can exacerbate the symptoms of dementia. Many patients require psychoactive drugs to treat the behavioral aspect of dementia, and it is difficult to determine if these drugs are exacerbating the cognitive decline, or if that is just a natural continuation of the disease process. The drugs that are most commonly associated with exacerbating cognitive impairment are psychoactive drugs including anticholinergics, opioids, benzodiazepines, antipsychotics, antidepressants, antiparkinsonian drugs, and anticonvulsants. However, physicians need to be aware that even non-psychoactive drugs can exacerbate symptoms of dementia or even lead to delirium, including histamine antagonists, cardiac drugs – particularly digoxin and other antiarrhythmics – corticosteroids, NSAIDS, and antibiotics.[vi] Therefore, it is important to discuss all medications, either prescription or over-the-counter medications, with the patient or their family members or care-givers during your history.
Your physical exam should focus on a complete neurologic exam as well as a mental status evaluation. There are many different scoring tools to assess mental status, including the Mini Mental Status Examination, or the Six-Item Cognitive Impairment Test, which can be used quickly in the emergency department. The validity for these tests have been best studied in the primary care outpatient setting; however, these tests can be performed quickly and provide a baseline status that will be useful when the patient follows up as an outpatient[vii]. Patients with pseudodementia may present with a chief complaint of memory loss. However, cognitive testing will be less likely to reveal clinical signs of dementia, and instead patients will have poor concentration and impaired motivation and energy when responding to questions[viii].
The neurologic exam could also point towards certain reversible causes of dementia. For example, a patient presenting with cognitive dysfunction and seen to have ataxia on neurologic exam may be suffering from normal pressure hydrocephalus, especially if the history also includes symptoms of urinary incontinence. Alternatively, patients with more focal neurologic findings such as isolated limb weakness or cranial nerve deficits may be suffering from a space-occupying lesion.
The basic labs that you should consider ordering on patients presenting to the emergency department that you suspect have undiagnosed dementia include a complete blood count with peripheral blood smear to assess for anemia, a complete metabolic profile (to evaluate electrolytes, liver function, and renal function), TSH, and urinalysis. If you have clinical suspicion for tertiary syphilis as a cause of the patient’s symptoms, consider adding a VDRL and serum fluorescent treponemal antibody assay. These patients should also undergo CT scan of the head to rule out space-occupying lesions or hydrocephalus. There are additional studies that can be performed as an outpatient, including serum vitamin levels, inflammatory markers, urine corticosteroid levels, and urine screens for drugs or heavy metals. These tests are difficult to run in most emergency departments and may not result for several days, when your patient hopefully is not in your department anymore.
Treatment and Disposition
Treatment for dementia will of course be determined by the cause of dementia. Any space-occupying lesion will require consultation with neurosurgery to determine any possible surgical options. Diagnosis of normal pressure hydrocephalus based on symptoms and CT imaging should prompt a neurology evaluation, as these patients can undergo further evaluation and testing on either an inpatient or outpatient basis, depending on the protocols of your institution.
Disposition can be tricky to manage in patients with dementia, regardless of whether the symptoms are chronic or relatively new. Patients who are not able to ambulate independently or perform their activities of daily living may be safe to discharge home if they have family members who understand the responsibilities of care and are physically able to assist the patient with those activities. Otherwise, the patient may need placement in nursing home or other institution. In rare situations, the patient may be able to get placement from the emergency department, but that depends on the patient’s insurance, their medical conditions, and the available resources of your community. If your emergency department has available social workers, they can help determine what options are available to your patient. If there is not an option for nursing home placement and your patient is not safe for discharge by themselves or with their family, they will require admission for physical therapy and/or occupational therapy evaluation to help better determine eventual disposition.
Case
Your patient from the case turns out to be a very nice gentleman who responds with only one-word answers. Cardiac, pulmonary, and abdominal exam are all normal. The patient has equal weakness in all extremities when tested while supine. When you ask him to walk, he takes a few steps with a wide-based gait, and then requires assistance from his son to make it back to the bed. Labs are all within normal limits, but CT Head shows brain atrophy with dilated ventricles. Neurology is consulted and they agree to take the patient and confirm the diagnosis of normal pressure hydrocephalus with lumbar puncture and begin the discussion with the patient and son about options for possible shunt placement.
Pearls
- Delirium is more acute in onset, fluctuates more frequently and drastically, and includes alterations in consciousness and perception; dementia induces a more gradual and steady decline and symptoms are predominantly impairments in memory and cognitive function.
- Common reversible causes of dementia include drugs (either overdose or poly-pharmacy), depression, metabolic or endocrine disorders, hydrocephalus, space-occupying lesions, decline in hearing or vision, infections, or anemia.
- Patients presenting with symptoms of dementia should be evaluated with CBC, chemistry, LFTs, TSH, and CT head to help identify reversible causes; not all reversible causes will be identified in the emergency department because they require further outpatient evaluation for diagnosis (such as depression or decline in hearing).
- Any patient who cannot ambulate or perform their activities of daily living and who does not have family able to care for them at home will require placement in a nursing home or institution; contact your social workers to see if this can be arranged from the emergency department.
References / Further Reading
[i] Pandharipande P, Cotton BA, et al. Motoric subtypes of delirium in mechanically ventilated surgical and trauma intensive care unit patients. Intensive Care Med. 2007 Oct; 33:726-1731.
[ii] St. Louis University Geriatric Evaluation Mnemonics and Screening Tools. Saint Louis University School of Medicine Division of Geriatric Medicine and the Geriatric Research, Education, and Clinical Center at the St. Louis VA Medical Center. http://aging.slu.edu/uploads/pdf/Saint-Louis-University-Geriatric-Evaluation_2013.pdf
[iii] Smith, JP, Seirafi J: Delirium and Dementia. Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 104: p 1398-1408.
[iv] Tripathi M, Vibha D. Reversible Dementias. Indian J Psychiatry 2009; 51: 52-55
[v] Smith, JP, Seirafi J: Delirium and Dementia. Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 104: p 1398-1408.
[vi] Moore A, O’Keeffe. Drug-Induced Cognitive Impairment in the Elderly. Drugs and Aging 1999; 15: 15-28.
[vii] Upadhyaya A, Rajagopal M, Gale T. The Six Item Cognitive Impairment Test (6-CIT) as a screening test for dementia: comparison with Mini-Mental Status Examination (MMSE). Curr Aging Sci 2010; 3: 138-42.
[viii] Haggerty JJ, Golden RN, et al. Differential diagnosis of pseudodementia in the elderly. Geriatrics 1988; 43: 61-69.





4 thoughts on ““Dementia” in the emergency department: can you do anything about it?”
Pingback: Länkar v37 | Internmedicin
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Delirium - emDOCs.net - Emergency Medicine Education
Pingback: March 18th Didactics – Lakeland Health EM Blog
Pingback: June ’20 Asynchronous Learning – Lakeland Health EM Blog