Authors: Jeremiah T. Phelps, MD, PhD (EM Resident Physician, University of Kentucky, Department of Emergency Medicine) and Christopher I. Doty, MD (Program Director and Vice Chair of Education, University of Kentucky, Department of Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
Case
A 63-year-old man presents to your emergency department on a busy Friday afternoon with a triage complaint of “numb… Rx refill” on the triage board. You’ve got a quick minute between higher acuity patients, and you pick up his chart. From triage, his vitals are BP 140/85, HR  99, Temp 37.0, RR 16, and SpO2 of 99% room air. You proceed to the fast-track area to investigate. The patient states he’s been out of his gabapentin for several weeks and continues to have numbness and tingling in both legs. He’s a poorly controlled type 2 diabetic and doesn’t recall his last A1C. He just wants his gabapentin and a quick discharge home. He has no additional complaints. On exam, he appears well. Being the excellent EM DOC that you are, you asking him to take off his shoes and socks to better examine his areas of numbness. On inspection, you find hairless, smooth pre-tibial surfaces bilaterally and an erythematous ulceration on the planter surface of his left foot. When asked how long he’s had this ulcer, he remarks, “What ulcer?” It seems your quick med refill just got more complicated. Now what do you do?
99, Temp 37.0, RR 16, and SpO2 of 99% room air. You proceed to the fast-track area to investigate. The patient states he’s been out of his gabapentin for several weeks and continues to have numbness and tingling in both legs. He’s a poorly controlled type 2 diabetic and doesn’t recall his last A1C. He just wants his gabapentin and a quick discharge home. He has no additional complaints. On exam, he appears well. Being the excellent EM DOC that you are, you asking him to take off his shoes and socks to better examine his areas of numbness. On inspection, you find hairless, smooth pre-tibial surfaces bilaterally and an erythematous ulceration on the planter surface of his left foot. When asked how long he’s had this ulcer, he remarks, “What ulcer?” It seems your quick med refill just got more complicated. Now what do you do?
Introduction
Diabetic foot infections (DFI) are a common problem for patients with poor blood glucose control. The lifetime risk of developing a diabetic foot infection is as high as 25% with estimates of yearly risk reaching 4%[1, 2]. Presentation of a DFI can range from simple cellulitis to osteomyelitis with the most common presentation being a foot ulceration. Major risk factors for the development of foot ulcerations include peripheral neuropathy and peripheral vascular disease [2]. Early recognition and treatment of DFI is essential, not only to reduce risk of developing life-threatening sepsis, but also to decrease incident of lower extremity amputation, the treatment of last resort associated with a poor quality of life and a very high 5-year mortality rate [3]. Vigilance for these infections in the emergency department may indeed save both life and limb in the diabetic patient. The astute clinician realizes that most DFI cases are like icebergs, and what you see on the surface often does not give the full picture of what lies beneath.
Pathophysiology
Long-standing, poorly controlled blood glucose leads to neurovascular damage beginning in the microcirculation and eventually involving more regional circulation. Damage in the lower extremities leads to development of peripheral neuropathy and peripheral vascular insufficiency, which can manifest as tingling, burning, prickling, and abnormal hot/cold sensations in the feet [2]. However, many patients are asymptomatic. As a consequence of this peripheral neuropathy, these patients will inadvertently bump into objects causing undiscovered local trauma and ulceration [2, 3]. Once local trauma is introduced, poor circulation and impaired immune system associated with diabetes provides a perfect environment for bacterial growth, and a diabetic foot infection is born. Most DFI are polymicrobial. The most common causative source is staphylococcus (S. aureus), though streptococci and enterobacteriaceae are also likely pathogens. In ischemic and necrotic wounds, aerobic gram-negative rods and anaerobes are often also present[3]. It is important to note that not all ulcers are infectious. Therefore, careful examination and classification of the ulcer should guide treatment[3].
Assessment and Treatment of the diabetic foot infection
The Infectious Disease Society of America (IDSA) created guidelines in 2012 for management of DFI [3]. The manuscript is comprehensive, as it describes evidence-based guidelines for both assessment and treatment of DFI. The IDSA recommendations support early recognition and risk stratification, as classification of DFI severity ultimately guides treatment. In terms of risk assessment, the IDSA proposes DFI evaluation across three categories: 1.) the whole person, 2.) the affected foot/limb, and 3.) the wound itself. The summary below adapts the IDSA approach with particular focus on what is possible in the setting of the fast-paced emergency department:
Assessment of the whole person
- Does the person look ill?
- Look for diaphoresis, pallor, delirium, altered mentation.
- Are there vital sign abnormalities?
- Look for fever, tachycardia, hypotension.
- Are there laboratory markers suggestive of systemic illness?
- BMP, CBC, ESR, CRP, procalcitonin to evaluate for electrolyte derangements, renal dysfunction, leukocytosis, and markers of systemic inflammation.
- According to the IDSA, CRP and procalcitonin may be used to distinguish uninfected ulcers from mild to moderate DFI [3]. Procalcitonin levels may be a more useful marker when following trends and response to therapy rather than to screen for infection.
Assessment of the lower extremity
- Are there signs of proximal infection spread?
- Look for lymphatic involvement.
- Any evidence of vascular insufficiency?
- Evaluate for pulse deficits, but most importantly always document an Ankle-Brachial Index (ABI)!
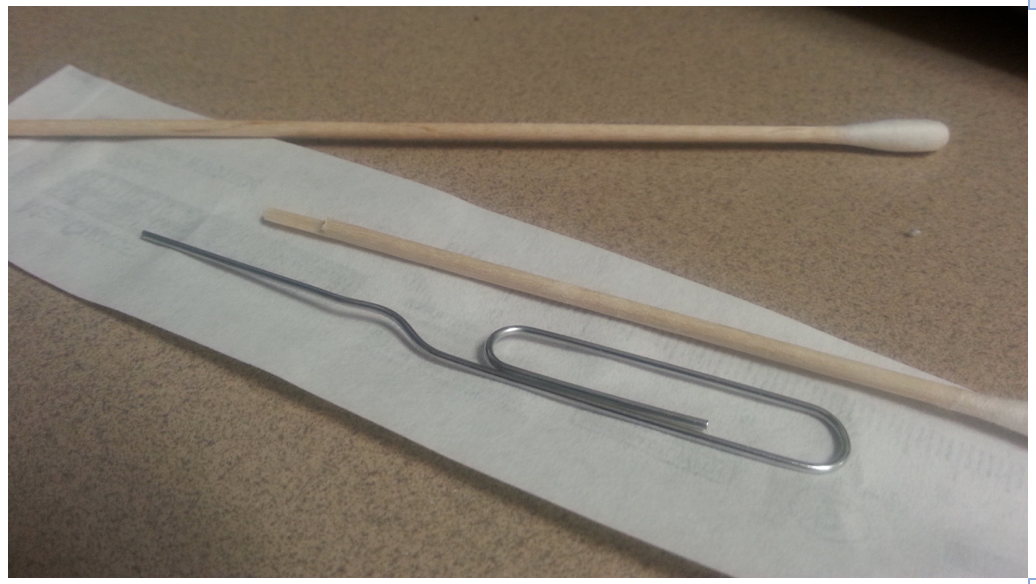
- Is there evidence of sensation loss?
- Evaluate for sensation loss with a monofilament.
- If a monofilament is not available in the ED, consider using the sharp end of a sterile, wooden cotton applicator or paper clip. Be careful not to embed shards of wood into the patient’s foot!
Assessment of the wound
- Are there any signs of local infection?
- Look for redness, swelling, induration, pain, purulence. Assess the plantar arch for fullness and tenderness which may occur with deep plantar space abscess.
- Better yet, grab an ultrasound to look for fluid collections
- Look for redness, swelling, induration, pain, purulence. Assess the plantar arch for fullness and tenderness which may occur with deep plantar space abscess.
- What is the wound size and depth?
- Explore the wound with a blunt metal probe. If you hit bone, consider osteomyelitis as part of your differential diagnosis.
This quick approach to the diabetic foot has been developed by the IDSA into a prospectively validated model for classifying DFI wounds that predicts need for hospitalization and risk for amputation [3]. According the model, wounds are classified as uninfected, mild infection, moderate infection, moderate infection, and severe infection. Each category carries a 0%, 4%, 52%, 89% risk for need of hospitalization, respectively; while risk for limb amputation is 3%, 3%, 46%, 70%, respectively [3]. The table below summarizes the classification scheme and risks for each class of infection severity as adapted from IDSA guidelines [3].

Infection present with at least 2 of the following:
- Local swelling induration
- Erythema
- Tenderness
- Warmth
- Purulent discharge
Treatment of the diabetic foot infection
Antibiotics
- If the wound is uninfected, DO NOT TREAT WITH ANTIBIOTICS.
- As with most infections, empiric treatment should be guided by local pathogen patterns and wound severity. Definitive therapy should be driven by wound tissue culture.
- While not the focus of this review, in addition to antibiotics, treatment of DFI wounds should include cleaning and debridement, either surgical or at bedside, to facilitate infection control and wound healing.
The IDSA guidelines propose empiric antibiotic treatment recommendations for DFI based on infection severity and causative pathogen. The table below represents a concise summary of the IDSA treatment guidelines. The IDSA recommends 1-2 weeks of antibiotics for mild infections, 1-3 weeks for moderate, and 2-4 weeks for severe infections [3]. Remember to check with your pharmacists and institutional policies before following these guidelines.

Wound culture
Wound culture is not recommended for uninfected DFI.
Infected wounds may be cultured from an appropriate tissue specimen. While culture collection may not occur in the ED, it is important to note that if cultures are obtained, tissue should only be collected from wounds only after they have been cleaned and debrided prior to starting antibiotics. Cultures from wound swabs and/or drainage is not recommended!
Wound off-loading
Reducing pressure on the ulceration is critical for wound healing [1, 2, 4]. While outside the scope of this review, options include stiff sole shoe, aircasts, Scotch-cast boot, or total contact casting.
Admission and Consultation
Patients with severe infections should be admitted for IV antibiotics. Patients with mild infection can be discharged with follow-up if reliable. Disposition for moderate infections may require more discernment; these patients may do well on oral antibiotics, but if they are unreliable or are likely to be lost to follow-up, admission for antibiotic therapy is reasonable [3].
Most importantly, IDSA recommends a multidisciplinary approach to diabetic foot care, as this approach has been shown to improve outcomes [3]. These patients will likely need evaluation by endocrinology, podiatry, surgery, and social work to encourage medical compliance and evaluate wound healing. IDSA recommends patients with peripheral vascular insufficiency and ulceration receive evaluation by a vascular surgeon. Additionally, patients with moderate and severe DFI should be seen by a surgeon to evaluate for debridement and need for further surgery. In those patients appropriate for discharge, it is critical they receive evaluation by a multidisciplinary team for management of their diabetes and diabetic sequelae. Coordination of this level of care will likely need to be performed by primary care physicians.
Key Pearls for treatment diabetic foot infection
– Inspect all diabetic patients for foot ulcers and infections.
– Do not culture uninfected diabetic ulcers.
– Swab and wound drainage cultures are not recommended.
– Choose antibiotic treatment based on wound severity.
– Diabetic care is complicated and requires multidisciplinary approach.
References / Further Reading:
- Uckay, I., et al., Diabetic foot infections: what have we learned in the last 30 years? Int J Infect Dis, 2015. 40: p. 81-91.
- Amin, N. and J. Doupis, Diabetic foot disease: From the evaluation of the “foot at risk” to the novel diabetic ulcer treatment modalities. World J Diabetes, 2016. 7(7): p. 153-64.
- Lipsky, B.A., et al., 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis, 2012. 54(12): p. e132-73.
- Park, T.H. and A. Anand, Management of diabetic foot: Brief synopsis for busy orthopedist. J Clin Orthop Trauma, 2015. 6(1): p. 24-9.







