
Authors: Allison Moyes, MD (EM Resident Physician, University of Washington / Harborview Medical Center, Seattle, WA) and Amy E. Betz, MD (Clinical Assistant Professor, Harborview Medical Center, University of Washington Division of Emergency Medicine, Seattle, WA) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) & Justin Bright, MD (@JBright2021)
The Institute of Medicine’s 1999 report “To Err is Human: Building a Safer Health System” drew attention to medical errors and the need for improving quality and safety in medicine.1 Since then, a body of literature has emerged suggesting that transparency around adverse events and medical errors benefits both providers and patients. However, the actual rate of disclosing medical errors has lagged behind popular support for the concept.2-5
Benefits of error disclosure
- Provides support for patients and enhances patient-provider communication.2, 6-8
- Improves institutional awareness of errors which might otherwise go unreported. Analyses of why errors occur can lead to system-wide improvements in quality and safety.5
- Open disclosure of medical errors may make lawsuits less likely.2-3,6
- In 2001, the University of Michigan adopted a program of full disclosure, which also offers compensation to patients for medical errors. Retrospective reviews have demonstrated a reduction in claims and liability costs since the program began.9
- Disclosure policies in other isolated institutions and insurance networks have yielded inconsistent results.10
- Nondisclosure of errors has been shown to decrease patient satisfaction and increase the likelihood of seeking legal advice.8
- The cumulative effect of error disclosure on legal claims remains difficult to determine and largely unclear.
The disclosure gap
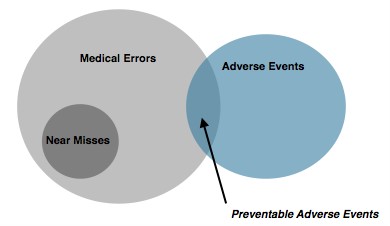
Patients and providers agree that errors resulting in otherwise preventable adverse events should be disclosed; however, actual rates of disclosure remain variable.2-6
- Patient surveys often indicate a desire for disclosure of errors wherein minimal or no harm occurs as well.7
- Whether to disclose these “near misses” appears to be more controversial among physicians and may account for a portion of nondisclosure cases.7
Uncertainty over which errors need to be disclosed, and how much information to share, may negatively impact rates of error disclosure.2,4,5,7
- Mixed messaging within institutions can compound provider uncertainty. Surveys of risk managers, for instance, demonstrate strong support for the disclosure of errors but less support for apologizing for errors.9
- Reducing conflict over error disclosure within institutions, through broad institutional support and policies, appears to improve disclosure rates.5,7
Concern exists over the possible legal repercussions of disclosure.
- Some states have adopted “apology laws” which prevent portions of disclosure from being used in lawsuits.2
- The protection provided by those laws varies significantly between states, however, and many states remain without any legal protection.
- The net effect of error disclosure on legal claims remains unclear.
Steps for the disclosure process
- Plan for the conversation
- Attempt to determine whether an error occurred and whether the error had an adverse impact on the patient. It can be difficult to say whether an error resulted in an otherwise preventable adverse event immediately. Do your best to assemble the facts through discussion with all of the involved personnel, and acknowledge ambiguity if it exists.
- Consult risk management at your institution before disclosing an error. Consider talking with your department’s quality improvement team as well.
- Plan your wording carefully. Be careful not to speculate or place blame. An admission of regret can be distinct from an admission of liability.
- Be aware of your own emotions and how they may impact communication. Patients often perceive rationalizations or defensiveness negatively. Aim for accountability and empathy.
- Set up for optimal communication
- Choose a quiet location with minimal distractions.
- Silence your pager and phone.
- Sit down.
- Arrange for an interpreter, if needed.
- Have the appropriate personnel present.
- Essential physicians – don’t overcrowd the meeting.
- Include a nurse manager or pharmacist if involved in the incident.
- Essential components of disclosure
Based on patient preference studies, disclosing an error should include the following core components.2-4,6-7
- An apology.
- An explicit statement that an error occurred.
- A factual description of what the error was, why it occurred, and its clinical implications.
- Acknowledge that the outcome of an error may be ambiguous at the time of disclosure.
- Discuss the possible repercussions and how the medical team will monitor for and manage adverse effects, and plan for subsequent conversations.
- An opportunity for the patient to relate his/her experience.
- A description of steps being taken to prevent recurrence of similar errors.
Summary
Benefits of error disclosure include enhanced patient-provider communication, opportunity for system-wide improvements in quality and safety, and possibly fewer lawsuits. Patients and providers agree that errors resulting in otherwise preventable adverse events should be disclosed; however, actual rates of disclosure remain variable. Approach the disclosure process with a few key steps in mind: 1. Plan for the conversation by assembling the facts and consulting with risk management ahead of time, 2. Set up for optimal communication, and 3. Include each of the core components in the discussion (see above).
References / Further Reading:
- Kohn LT, Corrigan J, Donaldson MS. To Err Is Human: Building a Safer Health System. Washington, D.C.: National Academy Press; 2000.
- Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289(8):1001-7.
- Gallagher, TH, Studdert D, Levinson W. Disclosing harmful medical errors to patients. New England Journal of Medicine 2007; 356(26): 2713-2719.
- Chamberlain CJ, Koniaris LG, Wu AW, Pawlik TM. Disclosure of “Nonharmful” Medical Errors and Other Events: Duty to Disclose. Arch Surg. 2012;147(3):282-286.
- King ES, Moyer DV, Couturie MJ, Gaughan JP, Shulkin DJ. Getting Doctors to Report Medical Errors: Project DISCLOSE. The Joint Commission Journal on Quality and Patient Safety, Volume 32, Number 7, July 2006, pp. 382-392(11).
- “Teaching Module: Talking about harmful medical errors with patients”. Tough talk: a toolbox for medical https://depts.washington.edu/toolbox/errors.html. Accessed: 06 March 2016.
- Fein S, Hilborne L, Kagawa-Singer M, et al. A Conceptual Model for Disclosure of Medical Errors. In: Henriksen K, Battles JB, Marks ES, et al., editors. Advances in Patient Safety: From Research to Implementation (Volume 2: Concepts and Methodology). Rockville (MD): Agency for Healthcare Research and Quality (US); 2005 Feb. Available from: http://www.ncbi.nlm.nih.gov/books/NBK20500/
- Mazor KM, Reed GW, Yood RA, Fischer MA, Baril J, Gurwitz JH. Disclosure of Medical Errors: What Factors Influence How Patients Respond? Journal of General Internal Medicine. 2006;21(7):704-710. doi:10.1111/j.1525-1497.2006.00465.
- Kachalia A, Kaufman SR, Boothman R, Anderson S, Welch K, Saint S, et al. Liability Claims and Costs Before and After Implementation of a Medical Error Disclosure Program. Ann Intern Med. 2010;153:213-221.
- Kachalia A, Shojania KG, Hofer TP, Piotrowski M, Saint S. Does full disclosure of medical errors affect malpractice liability? The jury is still out. Jt Comm J Qual Saf. 2003;29:503-11.
- Loren DJ, Garbutt J, Dunagan WC, Bommarito KM, Ebers AG, Levinson W, Waterman AD, Fraser VJ, Summy EA, Gallagher TH. Risk managers, physicians, and disclosure of harmful medical errors. Jt Comm J Qual Patient Saf. 2010 Mar;36(3):101-8.





2 thoughts on “Disclosure of Adverse Events and Medical Errors”
A big part of the reason why the U Michigan model works is because they protect their docs from data bank entry, see http://jama.jamanetwork.com/article.aspx?articleid=186745. The key quote “Settlement, if made, generally occurs in the system’s name, which is common practice at many hospitals with employed medical staffs”. The docs are less likely to keep things hidden and mistakes can be revealed early with timely resolution. They offer no reference to the statement that this is “common practice” with employed physicians, doubt it is widespread.
Pingback: Global Intensive Care | Disclosure of Adverse Events and Medical Errors