Authors: Matthew Nemero, DO (Resident Physician, SAUSHEC) and Joshua Oliver, MD (EM Attending Physician, SAUSHEC) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 15-year-old male patient presents to your emergency department with his family complaining of a fever for 3 days and a rash that started on his face and chest that has been spreading for 3 days. Past medical history is significant for 3 ED visits in the past 90 days and a new diagnosis of epilepsy for which he recently started seeing a neurologist and was placed on phenytoin 3 weeks ago.
Vitals: HR 84, BP 122/74, RR 12, T 38.8 (101.8F), SpO2 99% RA
- On physical exam, you palpate enlarged and tender cervical and axillary lymph nodes.
- You note the generalized rash shown below. It does not involve the oral mucosa.

Introduction
Drug reaction with eosinophilia and systemic symptoms (DRESS) can pose a bit of a conundrum for emergency physicians – patients can present with diffuse, nonspecific symptoms that occur weeks after the inciting event, which is most commonly a new anticonvulsant medication. A prolonged treatment course with frequent relapses, along with frequent reactivation of latent herpesvirus infection, complicates the disease process. With 10% of cases becoming fatal due to organ failure, it is important to identify and treat DRESS syndrome in a timely manner.
Background
DRESS syndrome, which is sometimes referred to as anticonvulsant hypersensitivity disorder (AHS), is characterized as a class IV hypersensitivity reaction. It leads to T-cell activation, which is the main component of the disease. Along with the latent T-cell activation, there has been a strong correlation with reactivation of latent EBV, CMV, or herpesviruses.1-3
Its frequency is estimated between 1/1,000 to 1/10,000 drug reactions, with 10% of those being fatal.4, 5 Being highly associated with aromatic anticonvulsants (those that contain an amine aromatic structure), it is more likely encountered in patients who take these medications daily, with a 12-year study showing that up-to 25% of all case reports were from new-onset administration of carbamazepine.6 Of note, incidence may be as high as 1% in patients taking lamotrigine.7 However, DRESS syndrome has also been reported with other drugs such as antibiotics, allopurinol, and ibuprofen. While there is a slight predilection towards females versus males (male/female ratio of 0.80), there is an increased incidence in children versus adults.8
Pathophysiology
While the pathophysiology is still being investigated, the current theory is that as the patient continues to take their new medication, drug metabolites build up in the liver leading to a systemic inflammatory state. This inflammatory cascade induces T-cell activation, possibly activating drug-specific T-cells in some individuals.8 Specifically, CD4+ cells release Type 2 cytokines that lead to the activation of eosinophils which causes the eosinophilia and leads to the clinical presentation of DRESS syndrome (rash, fever, eosinophilia).
There is also an association with the reactivation of latent viruses: herpesvirus (with HHV-6 being the most common), Epstein-Barr, and Cytomegalovirus. This reactivation is suspected to occur in two different pathways. In the first pathway the offending agent, while simultaneously causing the DRESS reaction, also directly induces reactivation of the virus; e.g. amoxicillin inducing HHV-6 replication.9 The second pathway is caused by the release of pro-inflammatory cytokines and chemokines, which cause a “cytokine storm,” leading to HHV-6 reactivation.10 The proliferation of defective CD4 and CD8 T-cells in the blood may also be a contributing factor that leads to virus re-activation.11
It must be pointed out that while viral reactivation was found in up to 80% of patients who are included in this report, viral reactivation is not a required component for DRESS syndrome and should not be used as criteria to diagnose DRESS syndrome.4
Clinical Features
The typical prodrome of DRESS syndrome (fever, pruritus, and tender lymphadenopathy) will follow the initiation of a new medication by 2-8 weeks.12 However, if a patient is re-exposed (as may be the case in a patient who took vancomycin, had subclinical DRESS syndrome, and then restarted vancomycin due to another recurrence), DRESS syndrome can occur in a matter of hours.13
The most common symptom noted in DRESS syndrome is fever (temp >100.4F), occurring in 90% of cases. Fever may present up to 1 week prior to the rash and can wax/wane. Symmetric and persistent facial edema is also a common finding in 75% of patients. Lymphadenopathy (>1cm) occurs in 75% of cases, most commonly in the cranial, cervical, axillary, or groin. Extensive cervical node involvement may add to the facial edema, and in some cases, may contribute to angioedema.14
The rash usually starts on the face or chest and spreads to the extremities. The rash is morbilliform and usually does not progress to erosions or bullae. Frequently, greater than 50% of body surface area (BSA) is involved, with involvement of >90% being strongly indicative of DRESS. The rash is usually pruritic, and patients may state that they were itchy days before the rash appeared. While mucosa involvement is common (56% of cases) it is usually limited to the mouth, throat, or lips. One defining characteristic is that mucosal lesions are usually only at a single site and do not progress to erosion as they would with SJS/TEN.
While lymphocytic infiltration of organs is a common finding in DRESS, patients do not usually present with symptoms of end-organ failure or injury. While the liver is the most commonly involved organ (>75%), patients do not frequently present with hepatomegaly or jaundice. Asymptomatic hepatitis is usually diagnosed by elevations in liver function tests (LFT) on admission or during routine screening.12 The RegiSCAR society defines liver involvement as an elevation of alanine aminotransferase (AST) greater than twice the upper limit of normal and/or an alkaline phosphatase greater than 1.5 times the upper limit of normal.
While liver involvement is usually mild, it is worth noting that most deaths from DRESS are associated with severe hepatitis. Presentations with markedly elevated LFTs, jaundice, and hepatic encephalopathy are the most likely to lead to death.
Renal involvement occurs in 40% of patients, most commonly manifesting as acute interstitial nephritis. DRESS with renal involvement has a much stronger association with allopurinol (67%) than other agents.8, 12 Patients with renal involvement typically present with proteinuria >1g/d or have an elevation greater than 1.5 times their baseline creatinine level.
Lung involvement is the third most-likely end-organ affected by DRESS (33%). Any evidence of interstitial involvement on x-ray, CT scan, or abnormal blood gases in an individual without a history of previous pulmonary injury would be considered a positive finding. Minocycline is the most common offending agent associated with lung involvement.13 There have also been reports of cardiac, pancreatic, gastrointestinal, and splenic involvement.11, 14
Diagnosis
Clinicians should be suspicious of DRESS in anyone who presents with a fever, rash, and a medication change within the past 2 months, especially with high-risk medications, or if the patient also has elevated eosinophils and liver enzymes.
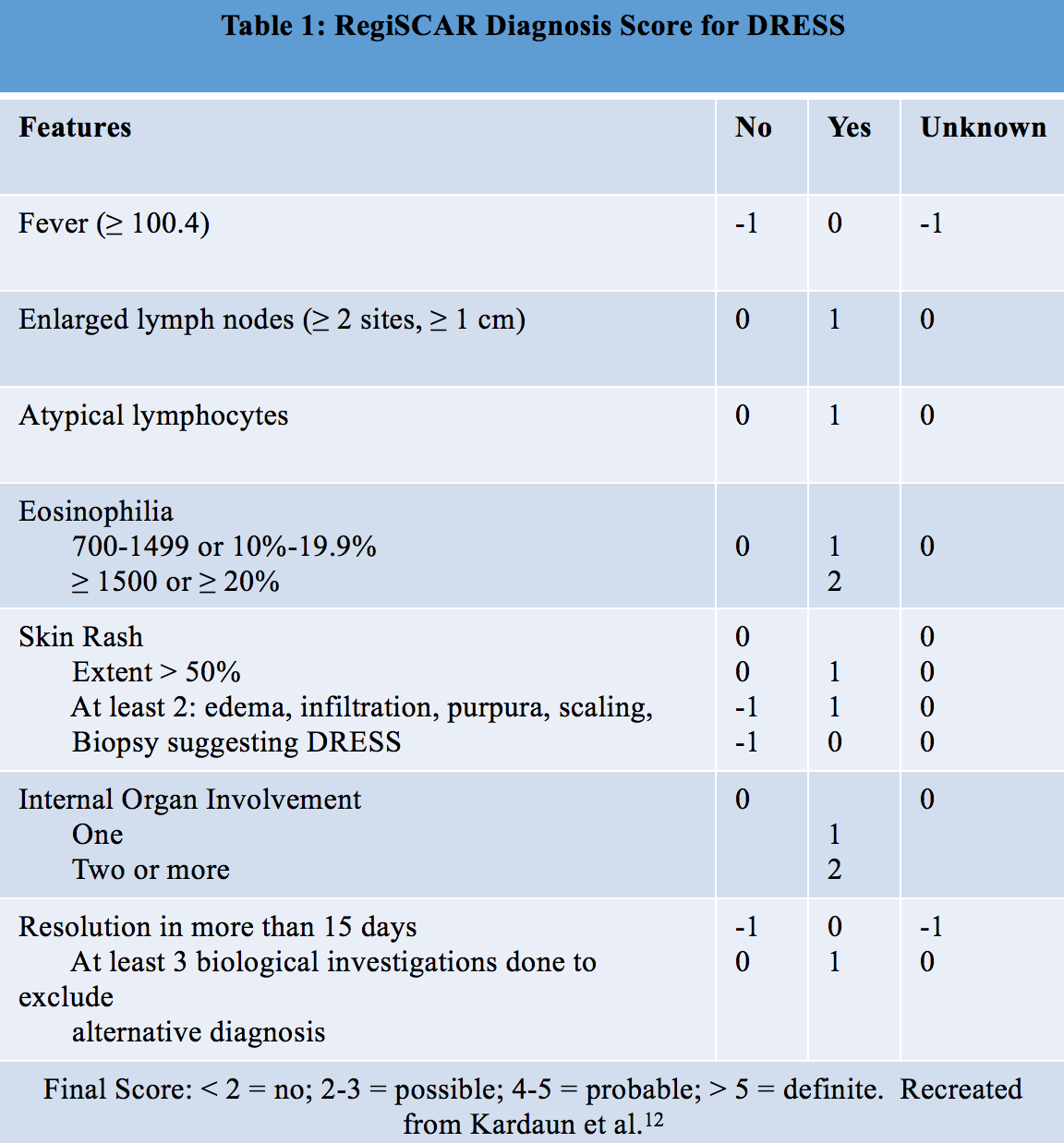
Given the variable presentation of DRESS and the non-specific findings, the RegiSCAR society developed the criteria in Table 1 to help identify cases of DRESS.12 The emergency physician should note that these criteria are not intended for use in the diagnosis of DRESS, as one of the hallmarks is a rash lasting >15 days. Instead, they are presented to help the emergency physician consider DRESS syndrome when the findings from Table 1 are present.
Laboratory testing is an important component of diagnosing DRESS. Leukocytosis is part of the diagnostic criteria, with eosinophilia and atypical lymphocytosis being the most common hematological markers. The most common markers of end-organ involvement are elevated LFTs which suggest hepatic involvement, whereas an increase in creatinine or proteinuria with eosinophils suggest renal involvement.
A viral panel should be ordered to look for acute viral hepatitis as a cause for elevated LFTs. While a herpesvirus infection is not indicative of DRESS, a concurrent viral reactivation may be prognostic for a longer and more complicated course as well as an indication for considering antiretroviral medications.
One important consideration of assessing end-organ involvement is that metabolic abnormalities (elevated LFTs or creatinine) are not present prior to eruption of the rash in 93% of cases.12-14
Distinguishing DRESS from Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis
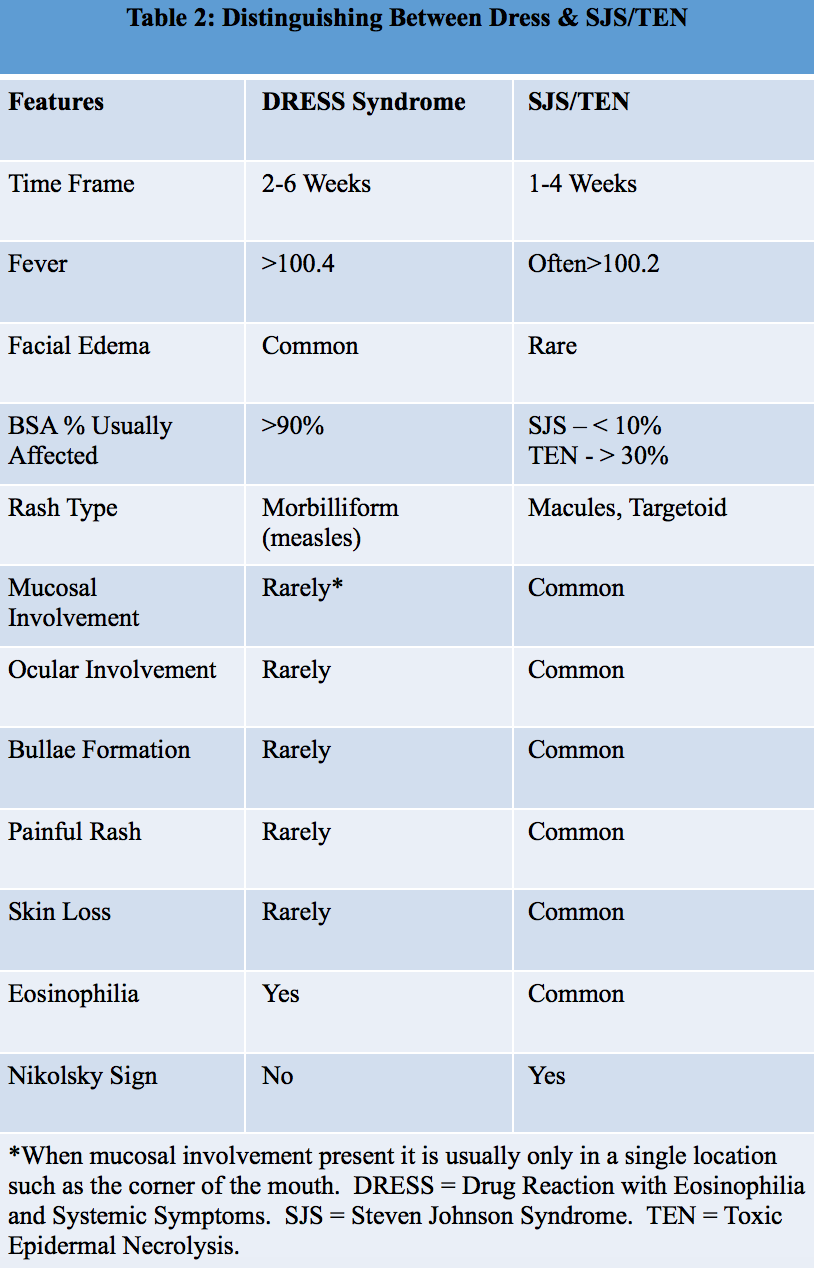
Since DRESS syndrome can have such a varied presentation, one important differentiation that should be made is between DRESS and Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis (SJS/TEN). SJS/TEN is a more acute and life-threatening dermatological emergency, so it is important diagnose early. Table 2 below lists some defining features to aid in diagnosis.1
Treatment
The mainstay of treatment in DRESS syndrome is stopping the offending agent. In patients with polypharmacy, this may mean stopping as many medications as the patient can safely tolerate while avoiding adding new medications. Patients may be treated on an outpatient basis, but admission should be strongly considered. Severe cutaneous reactions or multiple organ involvement requires hospitalization. Dermatology consultation is required. If the suspected offending agent is an anticonvulsant, valproic acid is often the recommended replacement agent.
For patients with mild cases of DRESS, the current recommendation is high or super high potency topical steroids in consultation with dermatology, as higher rates of infection, septicemia, and intensive care are more likely in patients who receive systemic corticosteroids.
For patients requiring hospitalization, most are commonly treated with systemic corticosteroids. While they do not appear to be detrimental in treatment, they also do not appear to directly improve mortality, as the risk of death is related to the amount of organ involvement and not cutaneous symptoms.15-17
As an example, extensive liver involvement will not directly benefit from systemic corticosteroids. However, some research has shown that treatment with n-acetylcysteine has led to improved outcomes.15
If systemic corticosteroids are used, the recommended dose is 1mg/kg/day, max 1g/day. They are maintained until symptoms begin to recede and are tapered over a course of 8 to 12 weeks to avoid flare ups of DRESS. An alternative option is to begin with pulse doses of 30mg/kg (max 1g/day) for 3 days and then continuing 1mg/kg/day (max 1g/day) regimen.15-17
In life-threatening cases, IVIG may be used at 2g/kg over 5 days. However, the evidence on IVIG use is inconclusive and should be made on a case-by-case basis. Antiretroviral agents may be used in cases where patients have positive confirmation of viral reactivation with severe viral symptoms such as encephalitis.
Key Points
-DRESS syndrome should be suspected whenever a patient presents with a fever, morbilliform rash, and lymphadenopathy following a medication change.
–Liver failure is the leading cause of mortality in DRESS syndrome
-Frequently co-exists with herpesvirus, CMV, or EBV reactivation
-The mainstay of treatment is stopping the offending agent
-DRESS without severe organ involvement is treated outpatient with topical steroids
-DRESS with severe organ involvement warrants hospitalization and the use of systemic corticosteroids
References/Further Reading
- Kano Y, Shiohara T. The variable clinical picture of drug-induced hypersensitivity syndrome/drug rash with eosinophilia and systemic symptoms in relation to the eliciting drug. Immunology and allergy clinics of North America. 2009;29:481-501.
- Kocaoglu C, Cilasun C, Solak ES, Kurtipek GS, Arslan S. Successful Treatment of Antiepileptic Drug-Induced DRESS Syndrome with Pulse Methylprednisolone. Case reports in pediatrics. 2013;2013:928910.
- Picard D, Janela B, Descamps V, et al. Drug reaction with eosinophilia and systemic symptoms (DRESS): a multiorgan antiviral T cell response. Science translational medicine. 2010;2:46ra62.
- Cacoub P, Musette P, Descamps V, et al. The DRESS syndrome: a literature review. The American journal of medicine. 2011;124:588-597.
- Chiou CC, Yang LC, Hung SI, et al. Clinicopathological features and prognosis of drug rash with eosinophilia and systemic symptoms: a study of 30 cases in Taiwan. Journal of the European Academy of Dermatology and Venereology : JEADV. 2008;22:1044-1049.
- Camous X, Calbo S, Picard D, Musette P. Drug Reaction with Eosinophilia and Systemic Symptoms: an update on pathogenesis. Current opinion in immunology. 2012;24:730-735.
- Guberman AH, Besag FM, Brodie MJ, et al. Lamotrigine-associated rash: risk/benefit considerations in adults and children. Epilepsia. 1999;40:985-991.
- Cho YT, Yang CW, Chu CY. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): An Interplay among Drugs, Viruses, and Immune System. International journal of molecular sciences. 2017;18.
- Mardivirin L, Valeyrie-Allanore L, Branlant-Redon E, et al. Amoxicillin-induced flare in patients with DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms): report of seven cases and demonstration of a direct effect of amoxicillin on Human Herpesvirus 6 replication in vitro. European journal of dermatology : EJD. 2010;20:68-73.
- Chen YC, Chiang HH, Cho YT, et al. Human herpes virus reactivations and dynamic cytokine profiles in patients with cutaneous adverse drug reactions –a prospective comparative study. Allergy. 2015;70:568-575.
- Takahashi R, Kano Y, Yamazaki Y, Kimishima M, Mizukawa Y, Shiohara T. Defective regulatory T cells in patients with severe drug eruptions: timing of the dysfunction is associated with the pathological phenotype and outcome. Journal of immunology (Baltimore, Md. : 1950). 2009;182:8071-8079.
- Kardaun SH, Sekula P, Valeyrie-Allanore L, et al. Drug reaction with eosinophilia and systemic symptoms (DRESS): an original multisystem adverse drug reaction. Results from the prospective RegiSCAR study. The British journal of dermatology. 2013;169:1071-1080.
- Kano Y, Hiraharas K, Sakuma K, Shiohara T. Several herpesviruses can reactivate in a severe drug-induced multiorgan reaction in the same sequential order as in graft-versus-host disease. The British journal of dermatology. 2006;155:301-306.
- Corneli HM. DRESS Syndrome: Drug Reaction With Eosinophilia and Systemic Symptoms. Pediatric emergency care. 2017;33:499-502.
- Moling O, Tappeiner L, Piccin A, et al. Treatment of DIHS/DRESS syndrome with combined N-acetylcysteine, prednisone and valganciclovir–a hypothesis. Medical science monitor : international medical journal of experimental and clinical research. 2012;18:Cs57-62.
- Redondo P, de Felipe I, de la Pena A, Aramendia JM, Vanaclocha V. Drug-induced hypersensitivity syndrome and toxic epidermal necrolysis. Treatment with N-acetylcysteine. The British journal of dermatology. 1997;136:645-646.
- Velez A, Moreno JC. Toxic epidermal necrolysis treated with N-acetylcysteine. Journal of the American Academy of Dermatology. 2002;46:469-470.





2 thoughts on “DRESS: What does the emergency physician need to know?”
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) - emDOCs.net - Emergency Medicine Education
Pingback: Länkar v41-42 | Internmedicin