
Author: Henry DeYoung MD (Flight Surgeon, NAS Norfolk, LT MC USN), Eric Sulava MD (EM Resident, NMCP, LT MC USN) // Edited by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 52-year-old male, with a past medical history of hypertension, hyperlipidemia, and tobacco abuse presents to the ED with the chief complaint of chest pain. He describes the pain as being different from his angina in the past. It is left sided, sharp, and worse at night when he is resting flat in bed. This pain has been occurring intermittently for the past week and unfortunately has not improved with Tylenol use. He has no other complaints and has been doing well since his hospitalization last month.
Initial Vital Signs: HR 101, BP 134/85, RR 18, SpO2 96% (on RA), Temp 38.6⁰C.
Exam: An age-appropriate male is sitting comfortably, leaning forward with his hands on his knees. Auscultation shows an elevated rate, but regular rhythm. Murmurs, rubs, and gallops are not heard, noting the ambient noise in the ED. He is clear to auscultation bilaterally on pulmonary exam, with no abdominal tenderness.
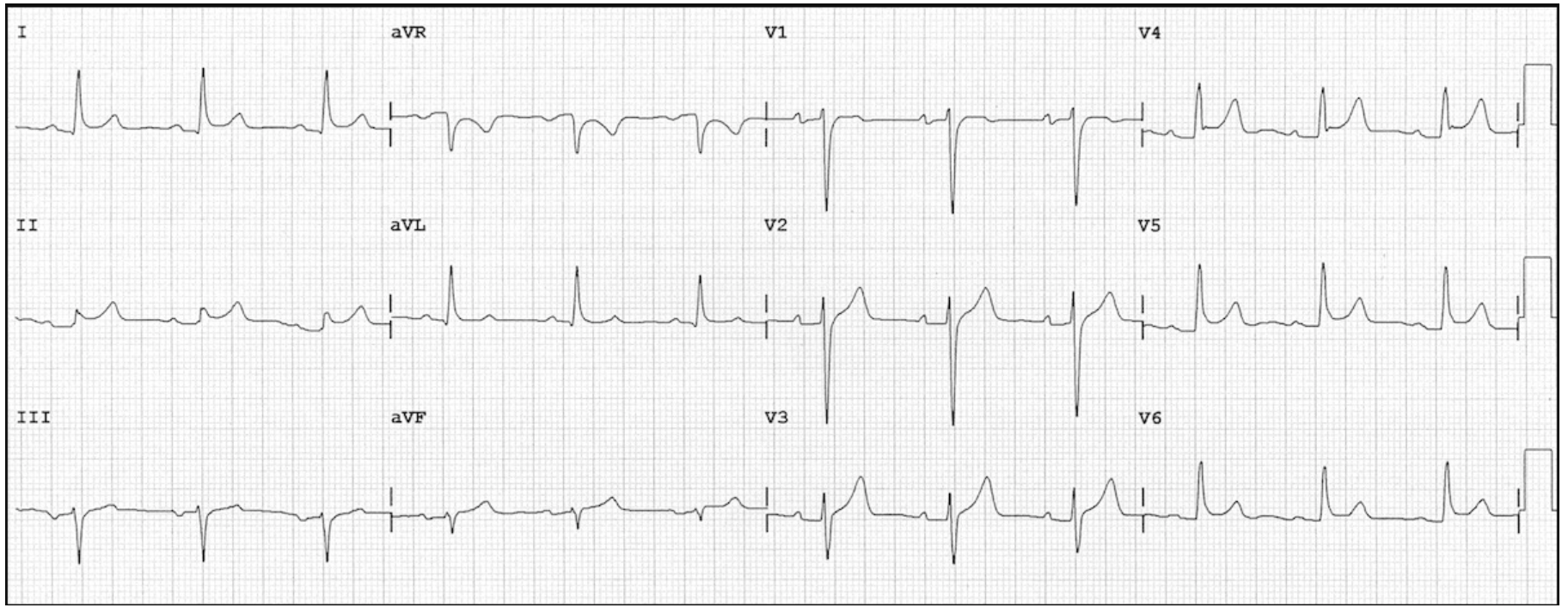
EKG:
What do you suspect as the diagnosis? What are your next steps?
Answer:
- The patient’s presentation suggests pericarditis.
- As with any high risk chest pain, an EKG should be done as soon as possible.
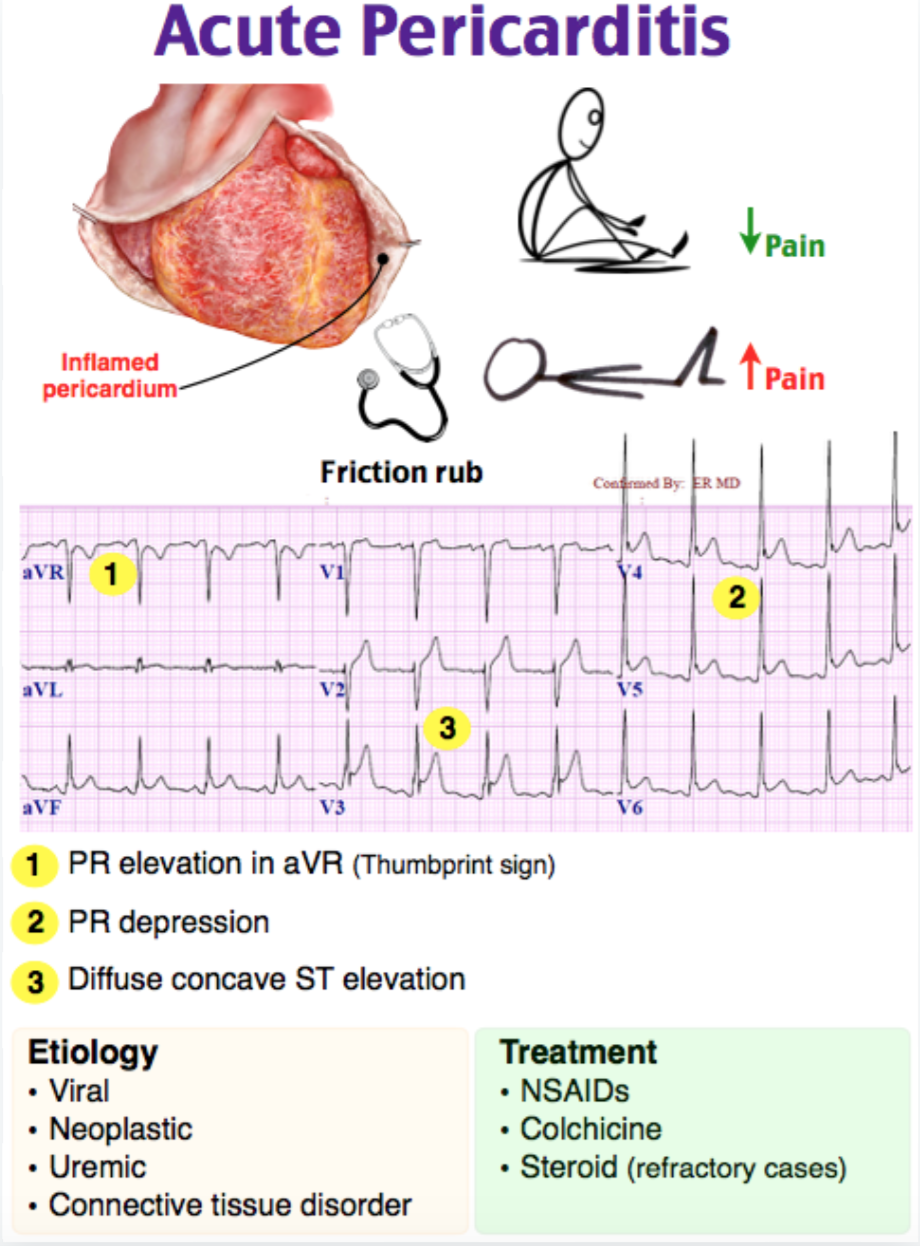
- EKG shows: Widespread ST-segment elevation, PR segment depression. ST elevations are all concave, elevation in lead II is > than lead III.
Anatomy:
- The pericardium is a double-walled sac that surrounds the heart.
- The outer (parietal) and inner (visceral) pericardial layers are separated by a potential space, called the pericardial cavity. Approximately 10-15 cc of pericardial fluid may be present at any time normally.
Definition:
- Pericarditis is an inflammatory syndrome leading to granulocytic or lymphocytic infiltration of the above mentioned layers.
Epidemiology:
- There are few published epidemiologic studies on the exact incidence and prevalence of acute pericarditis.
- Observational study form Finland (2014)
- Acute pericarditis is the cause of 0.2% of all cardiovascular admissions (1361 of 670,409).
- Associated in hospital mortality rate of 1.1%.
- Standardized incidence rate for pericarditis requiring hospitalization was 3.3 cases per 100,000 person-years.
- Males were found to be affected more often than females (65% vs 35%). [1]
Causes and Risk Factors:
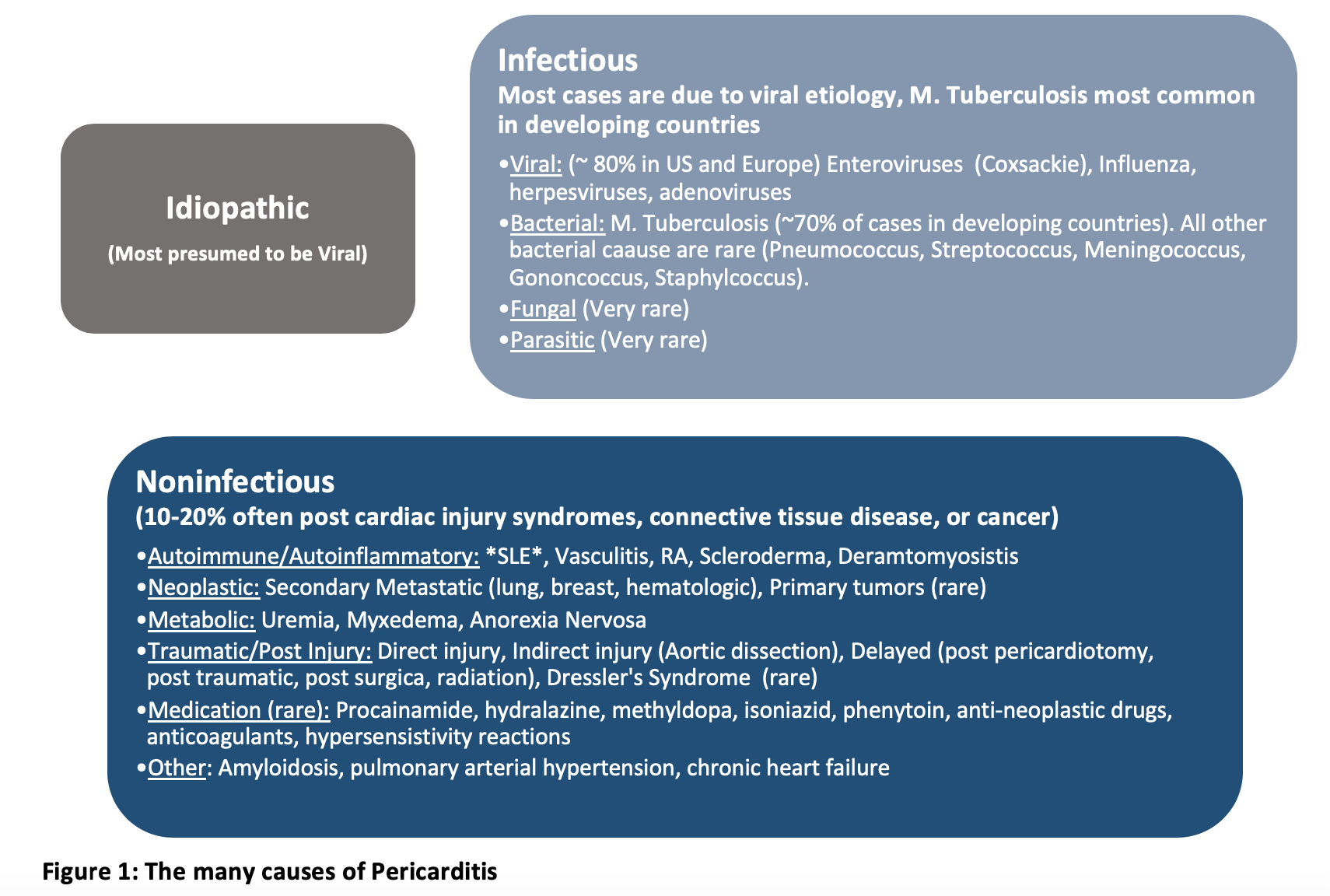
- Pericarditis has a wide range of underlying causes, including infectious, autoimmune, neoplastic, metabolic, traumatic, and pharmacologic (Figure 1). In the United states and Europe, pericarditis is most commonly idiopathic and presumed to be viral. Dresser’s Syndrome is now considered rare due to reperfusion therapy reducing the incidence of transmural myocardial infarction. [2]
Risk factors:
- Risk factors go hand in hand with the above causes of the disease
- Transmural MI
- Cardiac surgery
- Neoplasm
- Recent viral or bacterial Infections
- Uremia / history of dialysis
- In developing countries, pericarditis due to tuberculosis is common (70% of all cases)
- Prior to widespread availability of antiretroviral therapy, pericardial disease was the most frequent cardiovascular manifestation of the acquired immune deficiency syndrome (AIDS). [3]
Clinical Manifestations:
Symptoms:
- Chest pain that is the most common presenting symptom (~85% of cases).
- Described as: sharp /pleuritic, improved by leaning forward, worse with lying down, and often radiates towards the left trapezius (pathognomonic for pericarditis). [4]
- May have associated signs and symptoms specific to underlying disorders.
- Preceding prodrome (fever, chills, myalgias, gastroenteritis) to suggest associated viral prodrome.
- Symptoms related to autoimmune disease or malignancy. [5]
Physical Exam:
- Pericardial friction rub (1/3 of cases)
- Occurs due to friction caused by sliding the inflamed visceral pericardium against the parietal pericardium (or the parietal pericardium against the pleura).
- Heard best along lower left sternal border and apex with patient upright and leaning forward.
- Described as a scratchy or squeaky sound (may sound like walking on dry snow). [6]
- Manifestations of Pericardial Effusion (typically mild)
- Beck’s triad (hypotension, muffled heart sounds, distended jugular veins).
- Pulsus paradoxus (drop in systolic blood pressure > 10 mm Hg during inspiration). [5]
Workup:
EKG:
- Reliable diagnostic tool, but distinguishing pericarditis from acute MI is the first and most important step.
-
- Although, classically pericarditis presents with diffuse ST-elevations, localized ST-elevations are possible.
- In acute pericarditis, ST-depressions should not be present except in leads V1 and aVR.
- Acute pericarditis is often associated with PR depression.
- STE in leads II and III helps differentiate STEMI from pericarditis.
- STE II > STE III favors pericarditis.
- STE III > STE II is highly suspicious for STEMI.
- Spodick’s Sign is seen in approximately 80% of patients with acute pericarditis and is represented by down-sloping of the TP Segment. This is best seen in lead II and the lateral precordial leads. [7]
- ST elevations are more commonly convex with STEMI, while concave upwards ST elevations are more likely to be pericarditis., There are also often concurrent T wave inversions, reciprocal changes (ST Depressions), Q waves, as well as dynamic changes in STEMI. [7]
- ST Segment Depression in aVL helps differentiate inferior STEMI from pericarditis and is sensitive and specific for coronary occlusion in inferior MI.
- The ST Elevation vector in inferior STEMI occurs between 60-120⁰ in leads II and III. This is a difference of 90° to 150° from lead aVL (-30°) and should result in some reciprocal ST-segment depression in lead aVL. Diffuse inflammation of the pericardium in pericarditis results in an ST axis of approximately 45° (apex of the heart). This is a difference of 75° to lead aVL (-30°) and should not result in reciprocal ST-segment depression in lead aVL.
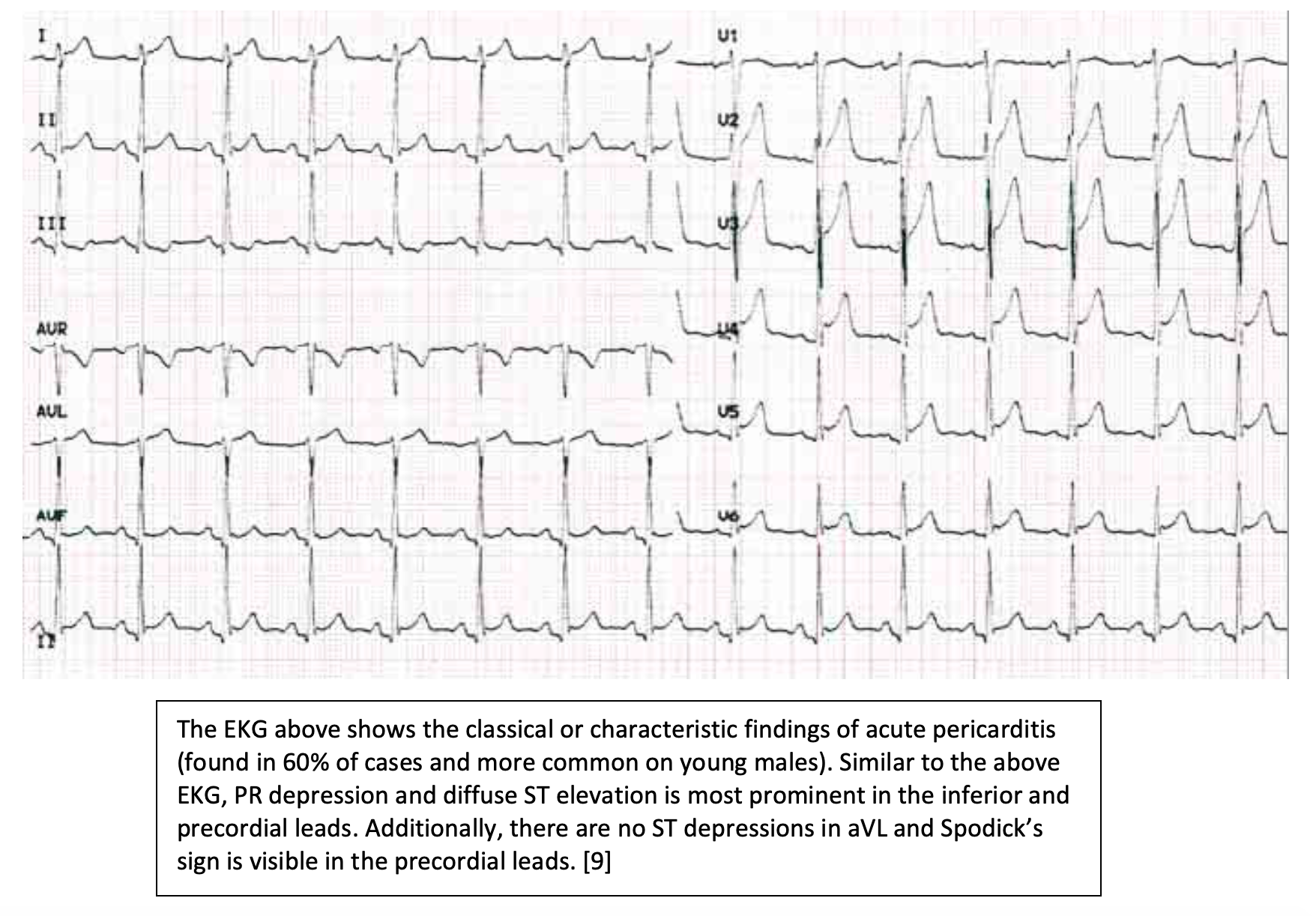
- Only 60% of patients will manifest the classical findings in pericarditis of widespread ST elevation (Figure 2).
- PR depression is most common in the interior (II, III, aVF) and precordial leads (V2-V6). [4]
- Over the course of disease the EKG may evolve significantly.
- Diffuse ST elevation -> normalization of ST and PR segments -> negative T wave deflection -> overall normalization (Figure 3). [9]
Labs:
- There is no single lab test with a high enough sensitivity or specificity to rule in or rule out pericarditis and differentiate from myocardial infarction.
-
- CBC (Leukocytosis), CMP (especially creatinine), Troponin, CRP, and ESR. Consider obtaining TSH, ANA as dictated by clinical suspicion.
- WBC may be elevated in acute stress due to MI; troponins may be elevated due MI as well as myopericarditis or myocarditis. [9]
- CBC (Leukocytosis), CMP (especially creatinine), Troponin, CRP, and ESR. Consider obtaining TSH, ANA as dictated by clinical suspicion.
Imaging:
- Echocardiogram
- Up to 60% cases will have pericardial effusion.
- Most effusions are mild (<10mm), but always consider cardiac tamponade.
- Large effusions (>20mm) are associated with complications / increased mortality.
- Up to 60% cases will have pericardial effusion.
- No focal wall motion abnormalities should be present.
- The absence of a pericardial effusion does not exclude pericarditis. [8]
- Chest-X-Ray is generally normal but recommended in all patients suspected of having acute pericarditis.
- May show an increased cardiothoracic (water bottle sign) ratio from chronic pericardial effusion (rare) or pleural effusion. [5]
- CT and MRI:
- Only necessary if the diagnosis is suspected, but difficult to confirm. Allow for detection of pericardial inflammation, pericardial thickness, and the presence of constrictive and/or effusive physiology. [10]
Diagnosis:
- Acute Pericarditis: requires two of four criteria.
-
- Characteristic Chest Pain
- Sharp/pleuritic that is improved by sitting up and leaning forward.
- Pericardial Friction rub
- Typical EKG changes: Widespread ST Elevation and/or PR depression
- New or worsening pericardial effusion
- Additional Supporting findings include elevated inflammatory markers and evidence of pericardial inflammation on CT or MRI. [3, 4]
- Characteristic Chest Pain
- Incessant Pericarditis: Pericarditis lasting for >4-6 weeks, but less than 3 months without remission.
- Recurrent Pericarditis: History of acute pericarditis with a 4-6 week period free of symptoms followed by recurrence of symptoms.
- Chronic Pericarditis: Pericarditis lasting for greater than 3 months. [5]
Treatment:
- Idiopathic and viral pericarditis is likely to resolve in 1-3 weeks without any intervention.
- First Line Therapy
- NSAIDS: No single NSAID appears to be more effective than another. Aspirin is preferred for any patient with a history of myocardial infarction. Treatment should be tapered until resolution of symptoms or normalization of inflammatory markers.
- Ibuprofen 400-800mg TID for 7-14 days; decrease by 200-40mg every 1-2 weeks.
- Aspirin 650-975 mg TID for 7-14 days; decrease by 200-400mg every 1-2 weeks.
- Colchicine: An important adjunct that improves outcomes. The ICAP trial (RCT) revealed that the use of colchicine reduced symptoms at 72 hours, rate of recurrence, rate of hospitalizations, and time to first recurrence.
- 0.5mg daily <70kg or 0.5mg twice daily >70kg for 3 months.
- Side effects: diarrhea
- Contraindications:
- Bacterial or neoplastic origin
- Severe liver disease
- Serum Cr > 2.5 mg/dL
- Elevated CK
- Blood dyscrasia
- Inflammatory Bowel disease
- Pregnancy / Women of childbearing age not on contraception [5, 11]
- NSAIDS: No single NSAID appears to be more effective than another. Aspirin is preferred for any patient with a history of myocardial infarction. Treatment should be tapered until resolution of symptoms or normalization of inflammatory markers.
-
- Proton Pump Inhibitor (PPI): All patients in the ICAP trial and other previous studies received a proton pump inhibitor for gastroduodenal prophylaxis. Patients with acute pericarditis should receive a PPI for the duration of therapy with NSAIDS/Aspirin and colchicine. [11]
- Second Line
-
- Corticosteroids: Though initially the therapy of choice for pericarditis associated with pericardial effusion, multiple studies have shown corticosteroids to be associated with many adverse effects. These include prolonged disease course and increased rates of recurrence.
- Consider using in specific patient groups such as pregnancy and systemic inflammatory diseases as well as cases where NSAIDS and Colchicine are insufficient.
- Exclude infectious etiology.
- Dose: 0.25-0.5 mg/kg/day for 2 weeks and then a slow taper.
- IVIG, Azathioprine, Subcutaneous Anakinra
- Corticosteroids: Though initially the therapy of choice for pericarditis associated with pericardial effusion, multiple studies have shown corticosteroids to be associated with many adverse effects. These include prolonged disease course and increased rates of recurrence.
- Recurrent cases where symptoms cannot be controlled with multiple drugs. These medications are typically not given in the ED. [8]
- Invasive Options: In the case of cardiac tamponade, hemodynamically significant pericardial effusion, or if the suspicion for bacterial etiology of effusion, pericardiocentesis may be necessary. If there is evidence of constrictive pericarditis, effusive pericarditis, and as last resort for refractory disease pericardiectomy should be considered. [2, 3]
Disposition:
- Although most patients can be safely sent home on empiric anti-inflammatory therapy, certain features are indicative of increased risk for complication and poor prognosis (nonidiopathic causes). The likely need for admission and need for targeted work up and therapy are divided into major and minor “red flags”. Hospital admission and search for etiology is necessary or indicated in patients with high risk features, and one feature alone is sufficient to identify a high-risk case. These features have been verified by multivariate analysis. The “minor” red flags are based on clinical expertise and literature review and should also prompt consideration for admission. [4, 5]
- Major Red flags
- Fever (>100.3⁰F, 38⁰C)
- Subacute onset
- Large pericardial effusion (>20mm on echocardiography)
- Cardiac tamponade
- Failure or lack of response to NSAID after 1 week of treatment.
- Minor red flags (based on expert opinion)
- Pericarditis associated with myocarditis
- Immunosuppression
- Trauma
- Current use of anticoagulants
Complications:
- Recurrent pericarditis occurs in approximately15-30% of cases.
- Myocarditis occurs concurrently in approximately 1/3 of cases.
- Defined by cardiac injury.
- Can be manifest as elevated cardiac biomarkers.
- Focal wall motion abnormalities and/or Left-ventricular dysfunction on ultrasound.
- Clinical heart failure and arrhythmias at the time of presentation are rare.
- Long-term prognosis for patients who have idiopathic pericarditis with associated myocarditis is excellent.
- Large effusions occur in approximately 3% of cases, but rarely cause cardiac tamponade.
- Although rare, large effusions are more common in with specific etiologies such at tuberculosis or neoplasm.
- Can progress to effusive constrictive pericarditis. [2]
From Dr. Katy Hanson at Hanson’s Anatomy:


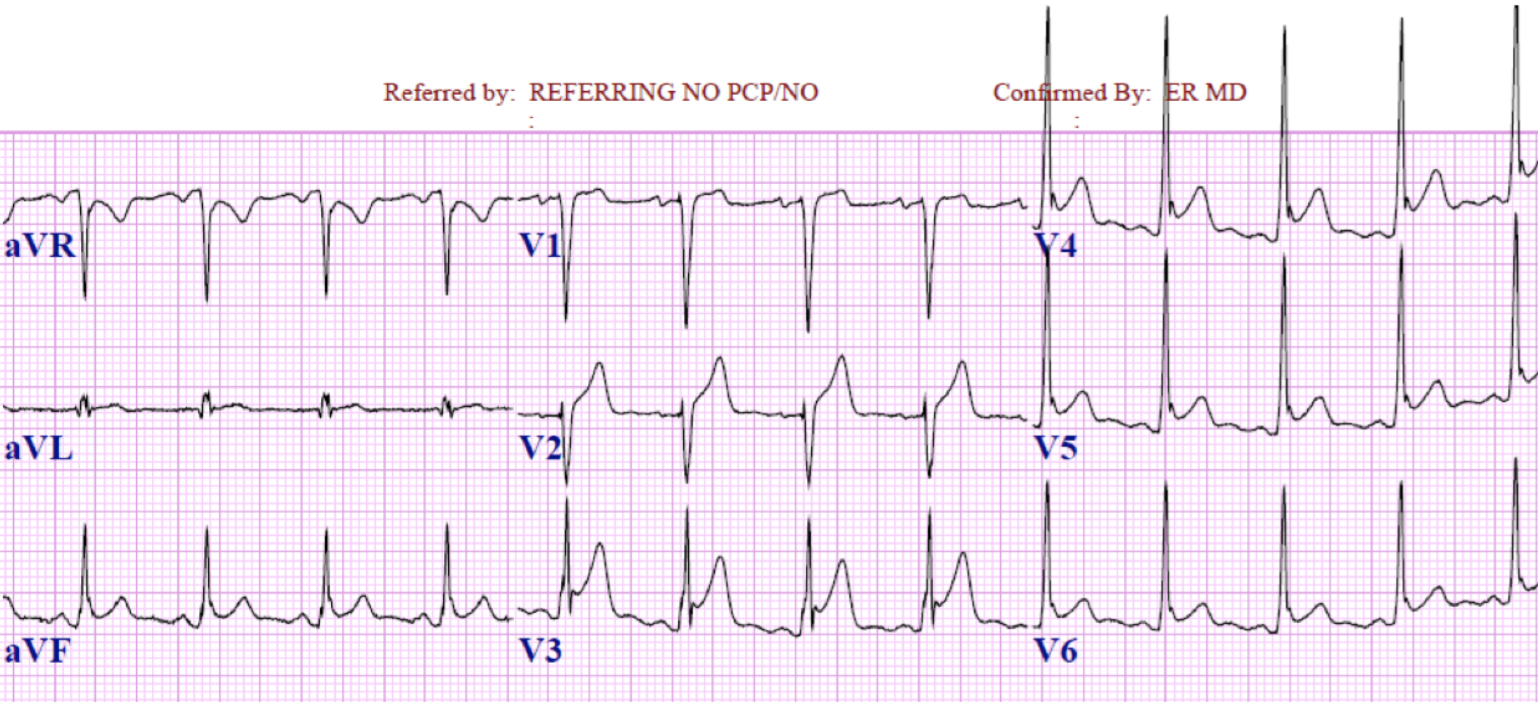
A 45-year-old man presents with a one day history of chest pain. The patient’s past medical history is significant for hypertension, hyperlipidemia, diabetes mellitus type II, and anxiety. He admits to feeling well prior to today other than a cold he recently got over last week. He describes the pain as sharp with radiation into his back. The pain worsens with lying flat and deep inspiration and improves when he leans forward. His vital signs are all within normal limits. He appears uncomfortable, sitting on the edge of the bed leaning forward. On exam, the patient has bilateral and equal breath sounds, and heart sounds are regular rate and rhythm. There is some minor reproducibility of the pain with palpation of the chest wall. The ECG is shown above. What is the likely diagnosis?
A) Myocarditis
B) Pericarditis
C) Pneumothorax
D) ST elevation myocardial infarction
Answer: B
Pericarditis is inflammation of the pericardial sac that surrounds the heart. This may be a result of infection, most commonly by a virus, however, bacteria and fungi have also been reported. Other etiologies include malignancy, drugs, uremia, or postmyocardial infarction. Pericarditis may also be idiopathic, which is thought to represent most cases. The patient typically presents with sudden or gradual chest pain that they describe as sharp or stabbing. Frequently, there is radiation to the back, neck, or left shoulder or arm. The pain may be worsened by movement or inspiration and will classically improve with sitting up and leaning forward and be made more severe by lying supine. Associated symptoms may include fevers, dyspnea, or dysphagia. A recent viral infection may also be reported. Physical exam may reveal a friction rub that is best heard at the left lower sternal border or apex. ECG findings of acute pericarditis consist of diffuse ST elevation that appears more convex in most leads. Rarely are there reciprocal changes. There is also PR segment depression. These changes are transient and therefore patients may have pericarditis without ECG changes. The diagnosis of acute pericarditis is made by the presence of two or more of the following: sharp and pleuritic chest pain, pericardial friction rub, ECG findings consistent with pericarditis, and new or worsening pericardial effusion. Additional lab tests and imaging is directed toward determining an etiology if concerns are present for causes other than idiopathic or viral pericarditis. Treatment for acute pericarditis can be outpatient, if the etiology is presumed to be viral or idiopathic and the patient is hemodynamically stable, with nonsteroidal anti-inflammatory drugs and follow-up. If other etiologies are present, then treatment will be specific to those causes and may require admission. Any patient with myocarditis, uremic pericarditis, enlarged pericardial silhouette on chest X-ray, or hemodynamic compromise requires admission.
Pneumothorax (C) occurs when air enters the potential space between the parietal and visceral pleural leading to a partial collapse of the lung. Smoking is the most common risk factor for spontaneous pneumothorax. Patients present with symptoms that are directly related to the size of the pneumothorax, rate of development, and health of underlying lung tissue. Acute pleuritic pain is found in most patients, however, a large volume pneumothorax may cause dyspnea, tachycardia, and hypotension. Tension pneumothorax is a life-threatening complication of a spontaneous pneumothorax and has clinical features of hypotension, tracheal deviation, and hyperresonance as hallmark signs. It is usually diagnosed on chest X-ray, however, anterior/posterior chest X-ray films have a documented sensitivity of only 83%, so further testing is warranted if there is a high index of suspicion. CT scans of the chest have higher sensitivity and may be more helpful in patients with bullous disease. Ultrasound can also be used for the diagnosis with better sensitivities reported compared to chest X-ray. Myocarditis (A) is caused by inflammation of the myocardium as a result of a systemic disease or an infectious agent. Viral etiologies are the most common of the infectious causes, but bacterial etiologies are also present. Clinical features include headaches, myalgias, rigors, and fever. Tachycardia is present in most cases and is usually disproportionate to the degree of temperature elevation. Chest pain may be present if there is coexisting pericarditis. In severe cases, there may be symptoms of progressive heart failure or cardiogenic shock. ECG may be normal or have nonspecific changes. Atrioventricular blocks or prolonged QRS may also be present. Cardiac enzymes may be normal or minimally elevated, and chest X-ray is typically normal. Treatment is supportive unless a bacterial cause is suspected. Many patients require admission for progressive congestive heart failure or require supportive treatment for cardiogenic shock. ST elevation myocardial infarction (D) is characterized by ST segment elevation typically in an anatomical distribution. Inferior myocardial infarction will demonstrate elevation in leads II, III and aVF. Posterior myocardial infarction will show depression in leads V1 and V2. Anterior and septal myocardial infarction will have elevation in the precordial leads. Reciprocal depression is typically noted in leads opposite to the elevation. Chest pain is the main symptom, however, associated symptoms such as shortness of breath, weakness, lightheadedness, syncope, and palpitations are also frequently reported. Primary percutaneous coronary intervention with stenting is the first-line and preferred therapy, however, fibrinolytics can be administered in the appropriate setting.





1 thought on “EM@3AM: Pericarditis”
Pingback: Perikardit – Översikt – Mind palace of an ER doc