
Author: Rachel Bridwell, MD (@rebridwell, EM Resident Physician, San Antonio, TX) // Reviewed by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX); Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 25-year-old male is brought to the ED by EMS with pain in the right scrotum after a motorcycle crash. The patient was wearing a helmet, could ambulate at the scene, and states his main concern is his right scrotal pain. Review of systems is unremarkable.
Exam reveals BP 141/90, HR 117, T 98.2 F oral, RR 15, SpO2 98% on room air. He has ecchymosis of right scrotum with exquisite tenderness and perineal bruising.
What’s the next step in your evaluation and treatment?
Answer: Testicle Rupture1-12
Epidemiology:
- Vast majority secondary to trauma1:
- Sports
- Motor vehicle collision
- Motor cycle collision
- 15% of testicular trauma is penetrating
- Gunshot wound, stabbing, animal bites, mutilation2
- Testicular tumors3
- Can rupture with trivial trauma
- It takes 20-50 kg of force for testicular rupture to occur2
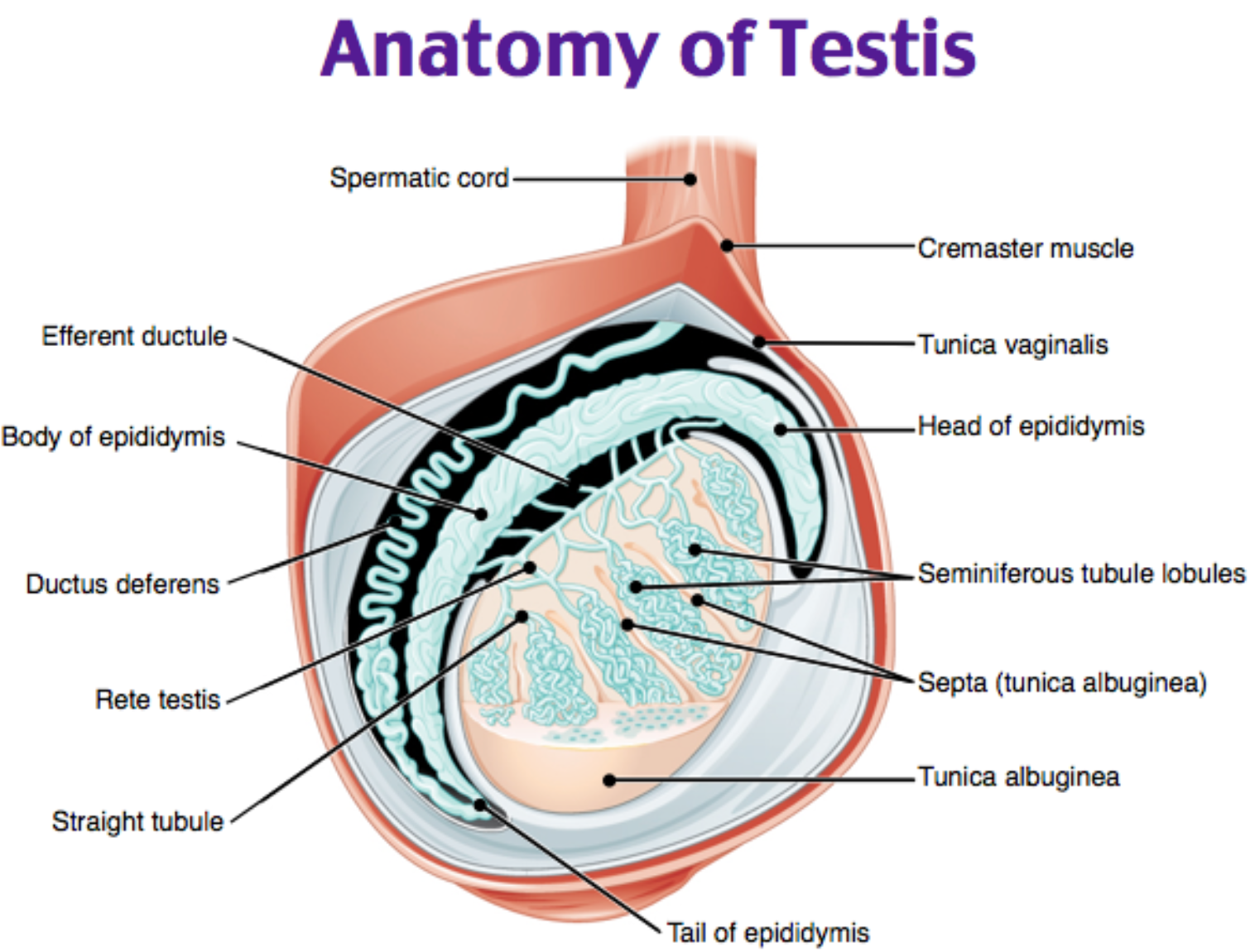
Anatomy:
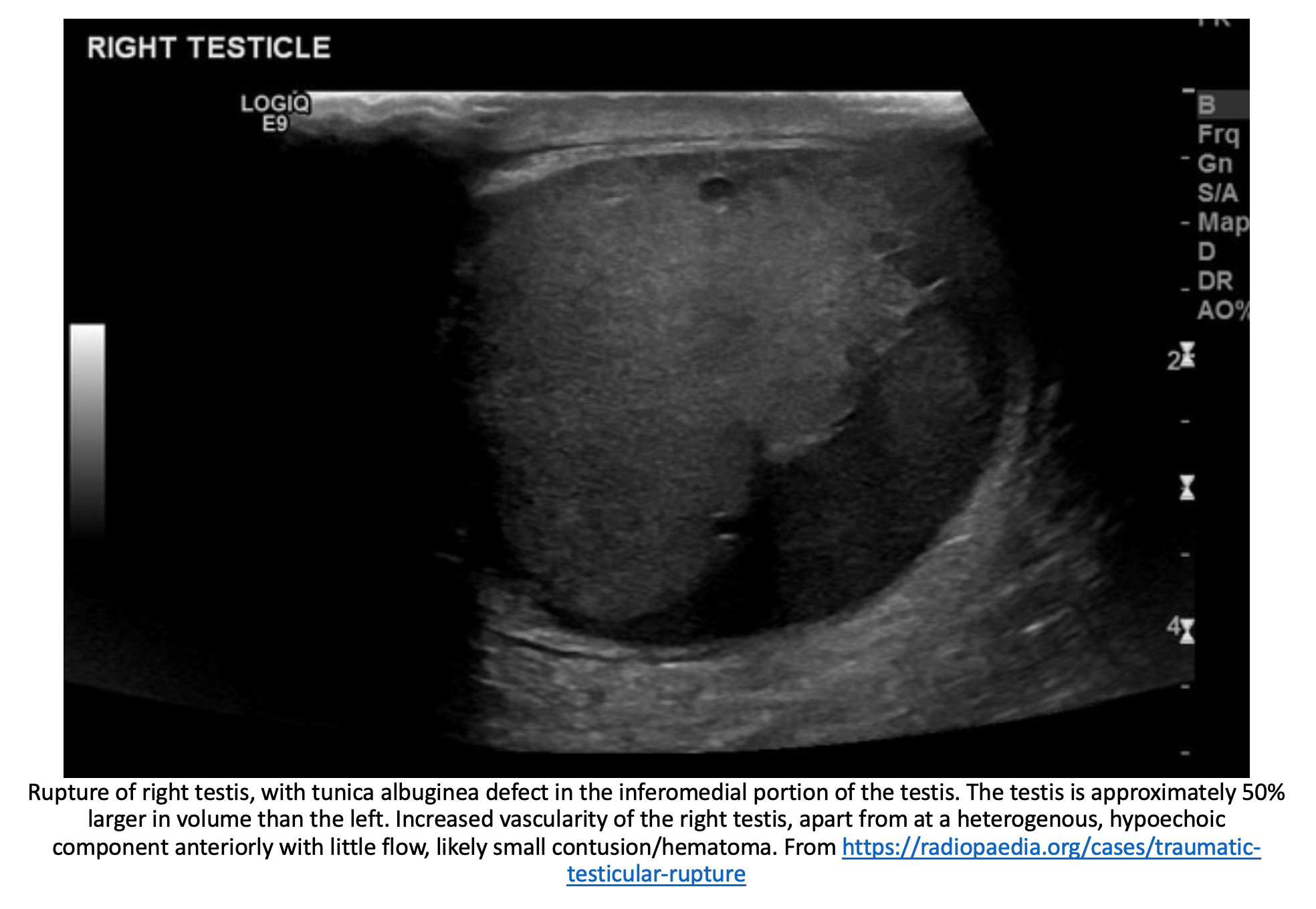
- Tunica albuginea is the rough fibrous layer covering the testis and disruption of this layer indications rupture4
- On ultrasound, normally appears as 2 parallel hyperechoic lines4
- Additionally extrusion of seminiferous tubules also indicates rupture4
- Rupture usually occurs from rapid deceleration or direct force against inferior pubic ramus5
Clinical Presentation:
- Signs and symptoms6
- Testicular pain
- Abdominal pain
- Dysuria
Evaluation:
- Assess ABCs
- Some injuries are from high energy blunt trauma so rule out life threats prior to assessing testicular rupture
- Perform a complete physical examination
- Abdomen: May reveal tenderness
- Genitourinary: Ecchymoses, hematoma of scrotum with swelling and tenderness, perineal ecchymosis
- Flank: +/- costovertebral angle tenderness
- Imaging:
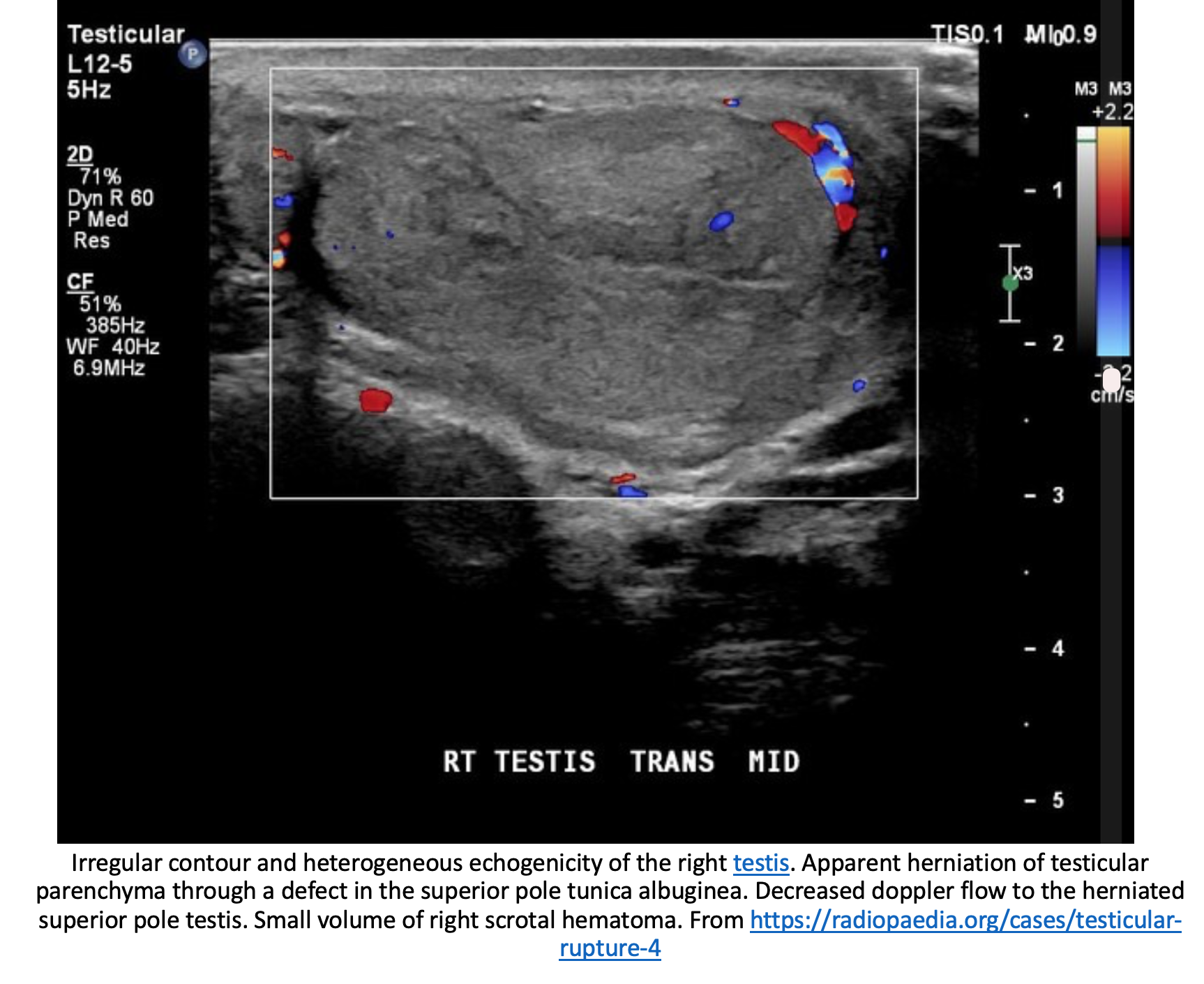
- Ultrasound (US): discontinuity of echogenic tunica albuginea, heterogenous echo pattern of parenchyma with loss of the contour definition7
- Specificity 93.5% and Sensitivity 100% in identifying surgically relevant rupture in n=65 pt%8
- Doppler allows for assessment of devascularization, with occurs with disruption of tunica algubinea9
- Computed tomography (CT) may demonstrate scrotal hematoma or traumatic hydrocele prompting further evaluation with other imaging modalities, ideally ultrasound10
- Magnetic Resonance Imaging (MRI) can be used if US does not show rupture and high clinical suspicion
- Higher sensitivity of 100% in identifying concomitant testicular fracture or epididymal hematomas only11
- Laboratory evaluation:
- Complete blood count, complete metabolic panel, urinalysis
- Ensure no ureteral involvement
- Complete blood count, complete metabolic panel, urinalysis
- Ultrasound (US): discontinuity of echogenic tunica albuginea, heterogenous echo pattern of parenchyma with loss of the contour definition7
Treatment:
- Discontinuity of the tunica albuginea indicates rupture and necessitates surgical management4,7
- Rapid consultation to urology for evacuation of hematoma and debridement of necrotic tissue
- Delayed consultation and operative management incurs 6% orchiectomy rate12
- Patients generally require admission
Pearls:
- Testicular rupture occurs in up to 50% of patients presenting with traumatic hydrocele and thus is likely underdiagnosed1
- Trivial or minimal blunt injury in a patient with testicular cancer may cause testicular rupture

A 33-year-old man fell from a tree while cutting limbs. He sustained significant perineal and genital trauma. Disruption of which of the following structures indicates a testicular rupture?
A) Buck fascia
B) Tunica albuginea
C) Tunica vaginalis
D) Vas deferens
Answer: B
The common mechanisms of blunt genitourinary traumas are falls, assaults, motor vehicle-related injuries, and sports-related injuries. Penetrating injuries are usually due to stab wounds or gunshot wounds. Timely diagnosis and appropriate management are aimed at minimizing or preventing renal dysfunction, urinary incontinence, and sexual dysfunction. A detailed history should be obtained to determine the time and mechanism of injury. The external genitalia, perineum, and gluteal folds should be thoroughly checked. Blood found on the pants or underwear is an important finding that may suggest genitourinary trauma. A digital rectal examination should be performed to inspect for blood, sphincter tone, or prostate abnormalities (e.g., bogginess or “high riding” prostate). External genital trauma may include penile fractures, scrotal lacerations or avulsions, testicular rupture, or testicular dislocation. A rupture has occurred if the tunica albuginea, the thick fibrous capsule that envelops each testis, is disrupted. The tunica vaginalis fills with blood and forms a hematocele. Diagnosis of testicular trauma is best evaluated with color Doppler ultrasonography. In addition to parenteral analgesia and appropriate tetanus prophylaxis and antibiotics (when indicated), urology should be consulted for testicular blunt or penetrating trauma. Testicular ruptures require immediate repair.
Buck fascia (A) is one of many membranous tissue layers that define the male genitourinary system. It is the deep fascial layer of the penis and does not envelop the testes. The tunica vaginalis (C) is a potential space that remains intact in testicular rupture. It fills with blood and forms a hematocele. The integrity of the vas deferens (D) does not define testicular rupture as it is external to the testes.
Further Reading:
FOAM Resources
- http://www.emdocs.net/genitourinary-trauma-presentations-evaluation-and-management-updates/
- https://coreem.net/core/testicular-torsion/
- https://www.maimonidesem.org/blog/potd-testicular-dislocation
- https://www.thesgem.com/2018/02/sgem205-twist-shout-testicular-torsion/
References
- Munter DW, Faleski EJ. Blunt scrotal trauma: Emergency department evaluation and management. Am J Emerg Med. 1989;7(2):227-234. doi:10.1016/0735-6757(89)90143-5
- Saleh D, Shaw D, Biyani CS. A dog bite to the adult scrotum. J Can Urol Assoc. 2009;3(5). doi:10.5489/cuaj.1166
- Lunawat R, Craciun M, Omorphos S, Weston PMT, Biyani SC. Seminoma presented as testicular rupture: Case report and literature review. J Can Urol Assoc. 2014;8(9-10 OCTOBER):e749-e751. doi:10.5489/cuaj.2194
- Addas F, Yan S, Hadjipavlou M, Gonsalves M, Sabbagh S. Testicular Rupture or Testicular Fracture? A Case Report and Literature Review. Case Rep Urol. 2018;2018:1-3. doi:10.1155/2018/1323780
- Ballestero R, et al. Testicular reconstruction after testicular rupture and review of the literature – PubMed. Arch Esp Urol. 2014;66(4):372-376. https://pubmed.ncbi.nlm.nih.gov/23676542/. Accessed April 13, 2021.
- Rottenstreich M, Gofrit ON. Blunt Scrotal Trauma in Soldiers—Epidemiology and Outcome. Mil Med. 2017;182(9):e1929-e1931. doi:10.7205/MILMED-D-16-00375
- Dalton DM, Davis NF, O’Neill DC, Brady CM, Kiely EA, O’Brien MF. Aetiology, epidemiology and management strategies for blunt scrotal trauma. Surgeon. 2016;14(1):18-21. doi:10.1016/j.surge.2014.06.006
- Flores S, Herring AA. Ultrasound-guided dorsal penile nerve block for ED paraphimosis reduction. Am J Emerg Med. 2015;33(6):863.e3-863.e5. doi:10.1016/j.ajem.2014.12.041
- Seung HK, Park S, Seung HC, Woo KJ, Jun HC. Significant predictors for determination of testicular rupture on sonography: A prospective study. J Ultrasound Med. 2007;26(12):1649-1655. doi:10.7863/jum.2007.26.12.1649
- Isikbay M, Sugi MD, Bowman MS, Choi HH. Traumatic testicular rupture: Multimodality imaging with intraoperative correlate. Clin Imaging. 2021;71:13-16. doi:10.1016/j.clinimag.2020.10.042
- Kim SH, Park S, Choi SH, Jeong WK, Choi JH. The efficacy of magnetic resonance imaging for the diagnosis of testicular rupture: A prospective preliminary study. J Trauma – Inj Infect Crit Care. 2009;66(1):239-242. doi:10.1097/TA.0b013e318156867f
- Cass AS, Luxenberg M. Testicular injuries. Urology. 1991;37(6):528-530. doi:10.1016/0090-4295(91)80317-Z




