Today on the emDOCs cast with Brit Long, MD (@long_brit), we cover acute compartment syndrome.
Compartment Syndrome
A surgical emergency, acute compartment syndrome (ACS) is the result of excessive pressure within a fascial compartment, leading to decreased perfusion.1-3 Incidence varies but is close to 0.7-7.3 cases per 100,000 people.2 Failure to treat ACS can cause long-term neurovascular deficits, and ACS is associated with significant medicolegal risk.4 In fact, 23% of medicolegal cases are due to misdiagnosis, and 32% of cases are due to delay to definitive treatment.5
The Risks
ACS is most common in patients < 35 years of age. These patients have increased risk of high-energy injuries, stronger fascia, and greater muscle bulk. Males are 10x more likely to experience ACS compared to females.2,6 Elderly patients have reduced muscle mass and more commonly hypertension, which increases perfusion pressures.7ACS most commonly occurs within 24 hours of the injury, but it can be delayed for days.8 Fractures are the most common cause, especially tibia fractures (2-9% of tibial fractures result in ACS).2,6,9-12 An open fracture does not mean ACS cannot occur, as the small fascial tears from these injuries do not decompress the compartment.12-15 Keep in mind that a variety of risk factors are associated with ACS:

How does ACS occur?
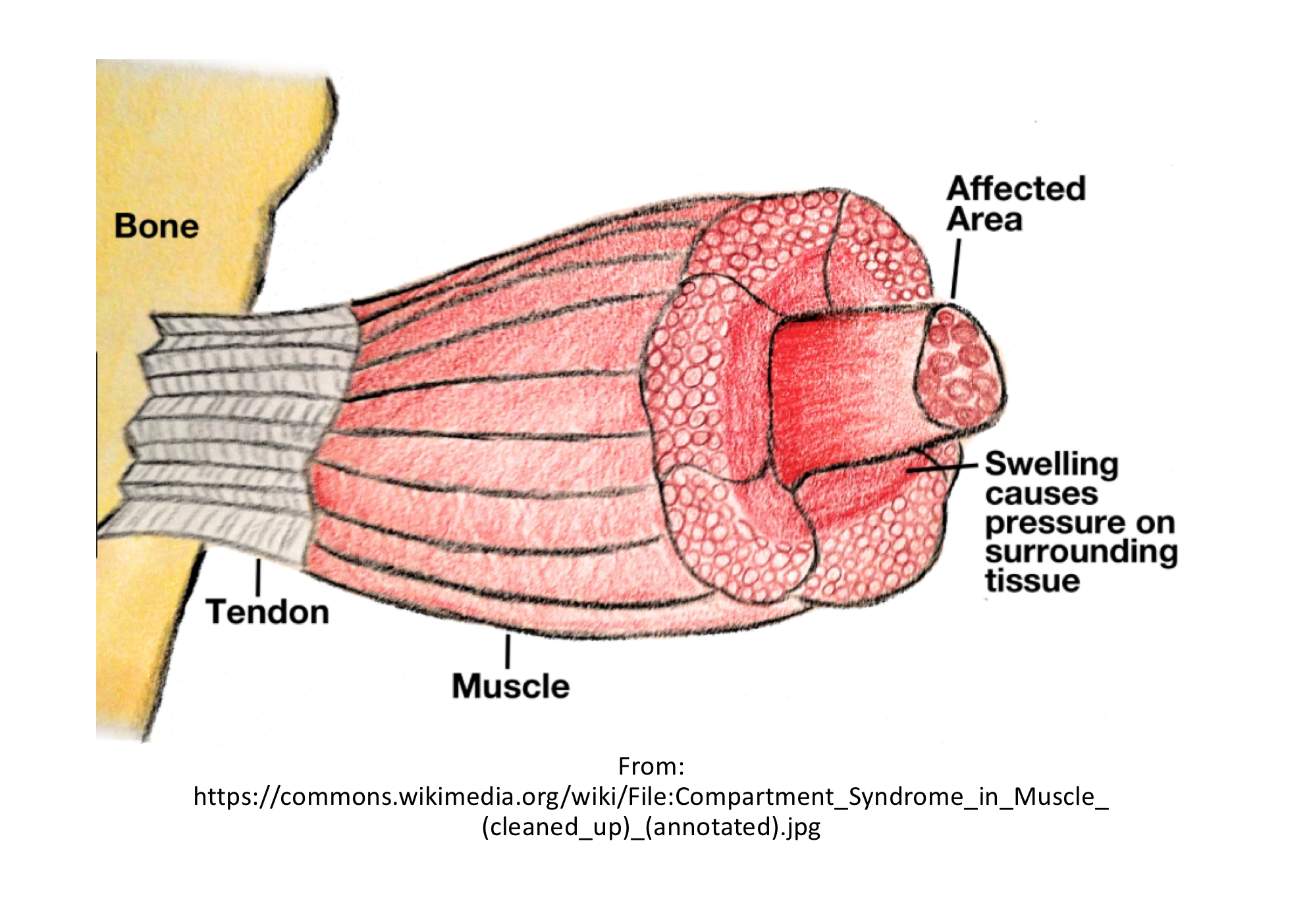
Increased pressure within a fascial or osteofascial compartment results in ACS, due to either increased volume within a fixed compartment (edema, hematomas) or decreased size of the compartment (extrinsic compression from body positioning, tight casts, or wound dressings).5,16-18 The increased pressure initially harms microcirculatory perfusion, but as the pressure continues to build, lymphatic, capillary, and small venule flow decrease, followed by reduction in the venous and arterial flow, leading to tissue ischemia and necrosis.5,16,17 If not treated, ACS can lead to fibrous tissue degeneration, neurologic damage, contractures, and even amputation.5,6,16,17 A cycle of worsening vascular flow and further increases in intracompartmental pressures is common. Necrosis can occur rapidly, as up to 1/3 of cases have necrosis of muscle within 3 hours after injury.19 One study found that neurologic injury is reversible if fasciotomy was performed within 4 hours, but injury is irreversible if the fasciotomy was delayed to after 12 hours.20
What compartments are commonly affected?
In the lower extremity, ACS most commonly affects the anterior compartment.21,22 Concern for ACS within the proximal leg or thigh requires a check of the anterior compartment of the thigh (due to its more frequent involvement),4,16,23,24 but isolated posterior compartment involvement can occur.25 For ACS of the foot, the interosseous intracompartmental pressure should be measured, and for hindfoot injuries, the calcaneal compartment should be assessed.26-32 ACS is most common in the volar compartment of the forearm for the upper extremity, but isolated dorsal ACS can occur.29-33 Monitoring of the arm anterior compartment and interosseous compartments of the hand is recommended.29,34-36
How reliable is your history and exam?
In the patient with severe trauma, the ABC’s come first. The injured extremity can be assessed after the ABCs, but keep in mind the key risk factors (Table 1), as well as any change in symptoms. Findings are often subtle, and early findings may only be found in alert patients.2,3,7 Diagnosis is tough in patients with altered mentation, severe trauma, substance abuse, and patients at the extremes of age.15 Severe pain is the earliest symptom (often out of proportion to exam).9,37,38 Patients often describe severe, burning, deep pain and worse with passive stretching,3 but pain is subjective and has poor sensitivity.9 Later symptoms include paresthesias, sensory deficits, and focal motor deficits.9,16,17 Pain can resolve in later stages with necrosis.15 Exam can reveal pain with palpation, pain with passive stretch, a tense or firm compartment, swelling of the affected limb, focal motor or sensory deficits, or decreased pulse or capillary refill.9,16,17 Paralysis and lack of pulses are rare, and compartment firmness is not reliable.3,21 Swelling is common, but again, subjective.7 The key to diagnosis is clinical suspicion and repeat exams!14,18 Digital palpation of the compartment is unreliable, with 49% sensitivity and 79% specificity for ACS of the hand and 24% sensitivity and 55% specificity for ACS of the leg.39,40 Abnormal pulse oximetry suggests poor limb perfusion, but a normal reading does not rule out ACS.7,9,15

Overall, signs and symptoms can suggest the diagnosis, but they are not definitive.9,41 Combining factors is better. A combination of pain with rest, pain with passive stretch, paralysis, and paresthesias increases sensitivity to 93%.9 Keep in mind that using clinical signs or symptoms alone is not recommended. Delayed diagnosis results in poor outcomes including infection, muscle necrosis, rhabdomyolysis, renal failure, muscle contractures, neurologic injury, chronic pain, fracture, amputation, and death.18,23,30,31,41-49 Missed diagnosis is associated with clinician inexperience, patient sedation, polytrauma, soft tissue injury, and reliance on signs and symptoms alone.9,23,42,50-55
What testing is needed?
Creatine kinase (CK), renal function, liver function, urinalysis, and urine myoglobin are recommended. CK > 1000 units/mL or myoglobinuria suggest ACS, and CK levels will continue to increase during the course of ACS.7,9,15,56 Rhabdomyolysis is present in > 40% of traumatic ACS cases.56-58 Renal injury can occur, usually due to rhabdomyolysis.7,9,15,56 X-rays of the affected extremity are usually obtained to look for fractures and other potential underlying causes.18,23,42
Once ACS is suspected, definitive diagnosis involves obtaining the intracompartmental pressure, which is most commonly assessed with direct, invasive monitoring.7,9,16,59 There are a variety of invasive methods for measuring pressures, including needle manometry, the wick catheter, the Whitesides method, and the solid-state transducer intracompartmental catheter (STC) device (Table 3).7,16,17,59 The most common method is an STC device such as the Stryker monitorTM, or using an arterial line transducer system.7,9,16,17 For more, see this video from EM:RAP on using the Stryker monitorTM and this EPMonthly article for a step-by-step guide. The Stryker monitorTM is accurate, with a sensitivity of 94% and specificity of 98%.38,60,61 However, the literature for use of STC monitors in trauma patients is limited.50,51,62
Pearls for Obtaining Pressures
When obtaining intracompartmental pressures, place the catheter within 5 cm of the fracture level, with the transducer secured at the level of the measured compartment.42,63-65 Make sure to keep the catheter tip outside of the actual fracture site. If placed within the fracture, levels will be falsely high.7,66 Failure to place the transducer at the same height of the catheter tip will cause a falsely high or low, depending upon the position.42,63,65 If the first pressure is normal, but concern for ACS is present, a compartment recheck is needed, with another pressure assessment.7,9,16,17,42
There are several noninvasive techniques, but they need further study. Near-infrared spectroscopy assesses the oxygen saturation of tissues, which shows promise in healthy volunteers and correlates with intracompartmental pressures.7,67-69 Ultrasound can assess the arterial pulse waveform in the setting of increased intracompartmental pressure, with a sensitivity of 77% and specificity of 93% for correlation with intracompartmental pressures in healthy patients.70 Neither of these is ready for the sick trauma patient.
What are the keys to diagnosis and management?
The most important point is to consider ACS. Once you suspect ACS, consult orthopedic or general surgery, remove any constrictive dressings, and avoid a dependent position of the extremity (try your best to keep the extremity at the level of the heart).7,9,14 Removing external compressive devices alone can reduce pressures by 65-85%.16,17,71,72 Reducing a displaced fracture will decrease edema.16,17,42 Analgesia is needed, but regional blocks are not recommended (they can make monitoring based on symptoms challenging).50,73-76 If the patient is hypotensive, resuscitation is needed to restore circulating volume.7,9,16,17
What’s this about using intracompartmental pressure alone versus differential pressure (ΔP)?7,9,16,17.42 The normal resting pressure within muscle is close to 8-10 mm Hg in adults and 10-15 mm Hg in children.77-81 Previous recommendations used an absolute intracompartmental pressure of 30-40 mm Hg as a threshold for fasciotomy.16,17,59,77,82-84 The problem with using an absolute pressure is that patients can vary widely concerning intracompartmental pressures.7,9,15 Also, different compartments have different pressure thresholds.16,17 Take the hand: an intracompartmental pressure > 15-20 mm Hg in the hand is a relative indication for fasciotomy.7,38 The key is perfusion pressure, but this can also vary based on many factors (age, pre-existing hypertension, vascular disease).13,59,60,85-87 The differential pressure is the diastolic pressure minus the intracompartmental pressure.7,9,16,17 Studies suggest that differential pressures of <30 mm Hg are an indication for fasciotomy, though critical ΔP is probably higher in muscle undergoing trauma or ischemia.7,13,22,64,88-90
Another important point is that outcomes improve with rapid diagnosis and decompression. Rapid fasciotomy is correlated with improved outcomes, including muscle and nerve injury and death.7,19,20,22,46,90 Unfortunately, a motor deficit due to ACS rarely improves with fasciotomy.3,7,42,46
A dynamic relationship exists among blood pressure, intracompartmental pressure, and time of elevated pressures.3,7,9,16,17,90 Higher pressures result in severe damage over a short period of time, but lower pressures sustained for long periods of time can cause similar damage.3,7,16,17 Do you need multiple measurements? Some use repeat clinical assessments, while others recommend continuous monitoring with a catheter attached to an arterial transducer in patients for whom assessment is difficult.3,7,13,91-93 The issue with single compartment measurement is that this can result in overdiagnosis and overtreatment.3,7,38,42 Several different protocols can be used pressure measurement, with studies comparing continuous pressure monitoring with serial monitoring.3,7,38,42 For continuous compartment measurements, clinical symptoms in combination with ΔP (<30 mm Hg) results in a sensitivity of 61% and specificity of 97%, while using ΔP in isolation results in a sensitivity of 89% and specificity of 65%.3,7,93 Diagnosing on single measures can result in unnecessary fasciotomies, with a false positive rate approaching 35%.98 Monitoring pressures over 2 hours using ΔP < 30 mm Hg as diagnostic criterion for ACS displays a sensitivity of 94% and specificity of 98.4%.13,38,42 What should you do? We recommend using a single measurement for patients who you can obtain a reliable history and exam, with repeat assessment if the first is normal and clinical suspicion for ACS still remains. If the patient cannot provide a reliable history and exam, use continuous monitoring over at least two hours or several repeat assessments.3,7,16,17 A ΔP < 20 mm Hg is a definitive indication for fasciotomy, with < 30 mm Hg a relative indication.3,7,13,88,89 Using ΔP may also help diagnose ACS in hypotensive trauma patients.7,9,13,38,42 Signs of ACS and absolute intracompartmental pressures > 30 mmHg also require fasciotomy.3,7,16,17 If elevated pressures have been present for > 3 days, a fasciotomy is unlikely to help, and in these cases, no decompression is advised. Instead it should be allowed to form scar tissue.3,7,9

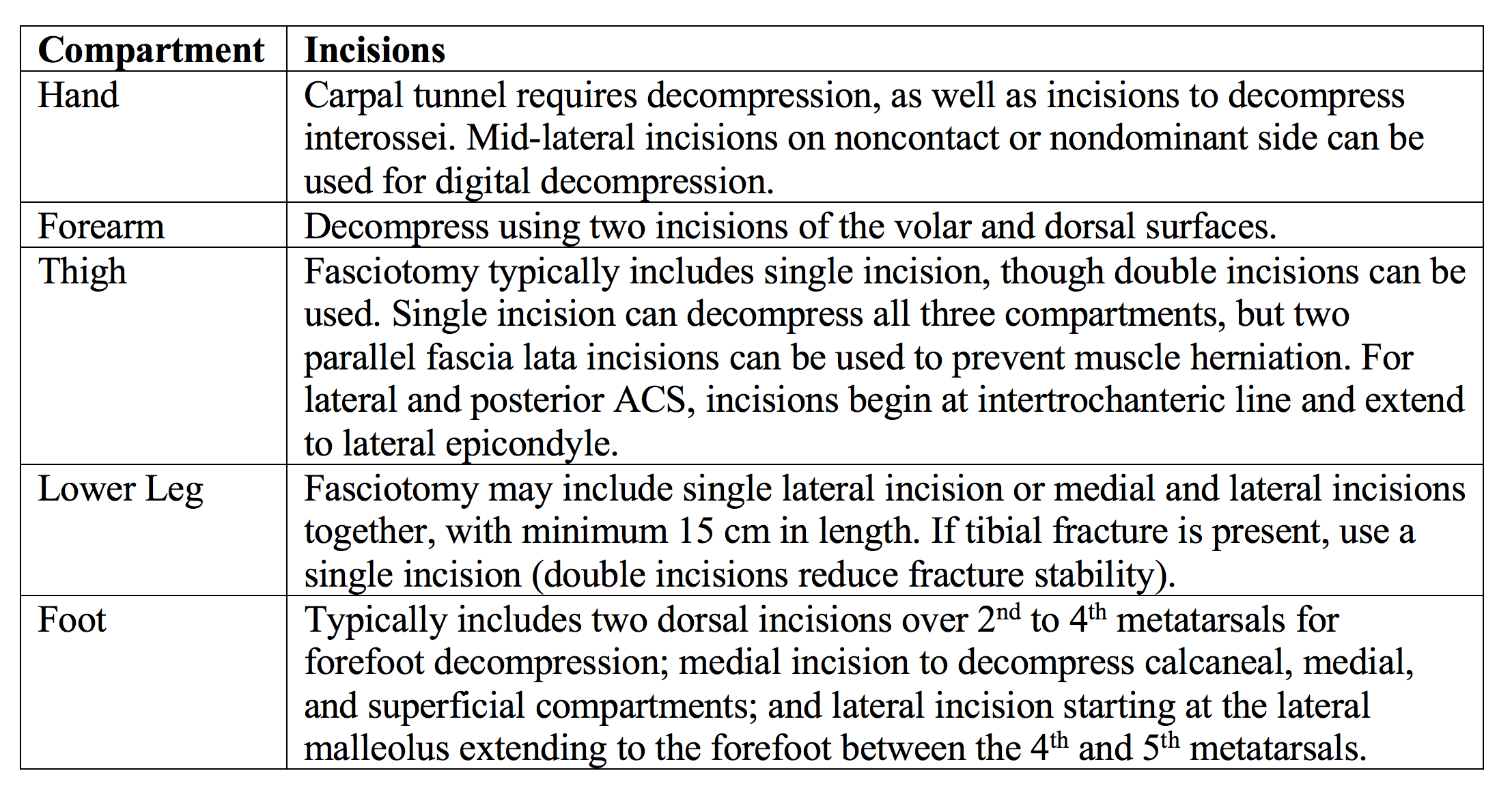
As discussed, definitive therapy is fasciotomy.56,97,98 The affected extremity and the number of compartments affects the approach.97-99
Approaches for Fasciotomy
Hyperbaric oxygen (HBO) may assist in management. HBO causes hyperoxic vasoconstriction, which can decrease edema and improve oxygenation.100,101 Keep in mind that HBO should not delay fasciotomy.100,101 At this point, more research is needed concerning HBO in ACS.
Disposition
ACS requires emergent evaluation by a surgeon (preferably orthopedics) with transfer to the OR. If the patient is at risk for ACS or ACS is suspected, admission with monitoring is the best course of action.3,7,9
Key Points
– Compartment syndrome is a time-sensitive surgical emergency caused by increased pressure within a closed compartment.
– ACS is associated with a number of risk factors but occurs most frequently after a fracture or trauma to the involved area.
– Pain out of proportion to the injury, paresthesias, pain with passive stretch, tense compartment, focal motor or sensory deficits, or decreased pulse or capillary refill time are signs and symptoms concerning for ACS.
– Pain is the earliest finding in patients with ACS, but findings on history and exam cannot rule out the diagnosis.
– Measurement of intracompartmental pressures using a pressure monitor is the most reliable test.
– Treatment involves analgesia, removing constrictive dressing, placing the limb at heart level, and surgical consultation for emergent fasciotomy.
From Dr. Katy Hanson at Hanson’s Anatomy:





