
Author: Erica Simon, DO, MHA (EM Resident Physician, San Antonio Uniformed Services Health Education Consortium, @E_M_Simon) // Edited by: Alex Koyfman, MD (@EMHighAK – emDOCs.net Editor-in-Chief; EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Manpreet Singh, MD (@MPrizzleER – emDOCs.net Associate Editor-in-Chief; Assistant Professor in Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center)
A 73 year-old patient presents to your ED with the chief complaint of “nosebleed.” Casually glancing down the hallway of your section, you see an elderly male shuffling to a bed, pressing a blood-soaked beach towel to his nares. As nursing staff performs their bedside triage, you enter the room and survey the monitor: BP 156/99, HR 122, RR 14, SpO2 96% RA.
The patient speaks in full sentences and is tolerating his secretions. He details a previous medical history of nasopharyngeal carcinoma, requiring recurrent radiation therapy. While discussing his family and social history, he begins to clear his mouth of large volumes of blood. The nurse reaches for a basin and an additional towel, while you survey the patient’s med list, which includes Plavix and aspirin.
On first glance, you observe active bleeding from the bilateral nares. Direct pressure has obtained hemostasis.
What is your next step? Topical vasoconstrictors? Nasal packing? Can this patient go home, or does he need to be admitted?
Let’s discuss a few key points about the management of posterior epistaxis.
The Epidemiology of Epistaxis
Epistaxis is one of the most commonly encountered ear, nose, and throat (ENT) emergencies in the US.1-4 It is estimated that up to 60% of the population will experience an episode of epistaxis throughout their lifetime; with approximately 10% having a bleeding source localized to the posterior nares.1-7 Current data demonstrate a bimodal age distribution of epistaxis with the majority of cases occurring amongst those aged 2-10 years and 50-80 years.1,3 Despite this reported prevalence of epistaxis, epidemiologic data cite only 6% of individuals as presenting to healthcare providers for anterior epistaxis treatment, and only 5% for posterior epistaxis treatment.3,5-7
Seasonal variation in the rates of epistaxis have been described in temperate and tropical climates.8 The majority of epistaxis episodes in the US occur during the winter months, a finding thought secondary to a decrease in ambient humidity and increase in concomitant upper respiratory infections.8 In tropical climates, epistaxis occurs frequently during dry seasons.8
Etiologies of Epistaxis
The following chart, adapted from Kucik et al.’s, 2005, and Yau’s, 2015 works provides an excellent summary:
| Local Causes | Systemic Causes |
| Chronic sinusitis | Hemophilia |
| Epistaxis digitorum (nose picking) | Leukemia |
| Foreign bodies | Medications (e.g., aspirin, anticoagulants, NSAIDs) |
| Intranasal neoplasm/polyp | Conditions causing platelet dysfunction (e.g., cirrhosis, uremia) |
| Irritants (e.g., cigarette smoke) | Thrombocytopenia |
| Medications (e.g., topical steroids) | |
| Rhinitis | |
| Septal deviation/perforation | |
| Trauma | |
| Vascular malformations/telangiectasias |
Table 1 – Etiologies of Epistaxis2,7
A Brief Anatomy Review
Clinically, epistaxis is classified as anterior or posterior according to the anatomic source of bleeding.
The vascular supply of the nose originates from the ethmoid branches of the internal carotid arteries, and the facial and internal maxillary divisions of the external carotid arteries.2,8 The anterior portion of the nasal septum is supplied by an anastomosis of the terminal branches of the sphenopalantine and anterior ethmoidal arteries, and the superior labial branch of the facial artery.2,8 This anastomosis is commonly known as Kiesselbach’s plexus, the area from which the majority of anterior epistaxis episodes arise.1-5,8
The sphenopalatine artery and terminal branches of the maxillary artery supply the lateral nasal wall (below the middle turbinates), and are commonly responsible for reported cases of posterior epistaxis. 2,8
The figure below details relevant anatomy:
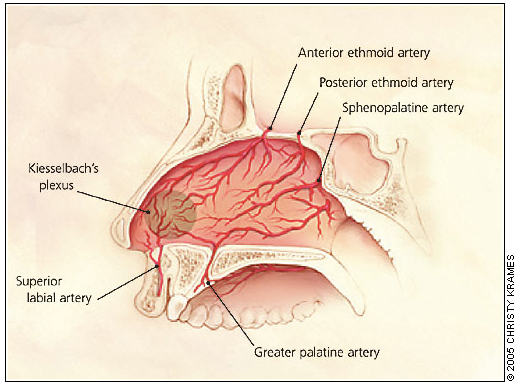
Figure 1 – Anatomy of the Nasopharynx2
The Evaluation of a Patient Presenting with Epistaxis
Evaluation should begin with an assessment of the ABCs. If the patient is actively bleeding, but protecting his airway and hemodynamically stable, he should be placed in a seated position (leaning forward so as to avoid increasing the flow of blood to the posterior oropharynx), and instructed on the application of direct pressure to the bilateral nares for approximately 5-10 minutes.1,2 Expectoration of blood residing in the oropharynx should be encouraged so as to reduce the risk of aspiration or emesis.2,3,7
If stable, important items to address in history taking include:
- Onset, activity undertaken prior to onset (digital trauma), duration, and laterality of the current bleed. If the patient has sought care for episodes of epistaxis previously, inquiries regarding methods utilized to obtain hemostasis should be made.
- Frequency of epistaxis/seasonality of symptoms.
- Review of systems: skin rashes (petechiae/pupura), easy bruising
- Previous medical history: hepatic disease (cirrhosis), renal disease (uremia), nasopharyngeal carcinoma requiring radiation therapy/oncologic surgery
- Social history: smoking (irritant), recreational drug use (specifically cocaine and other inhalants)
- Medication review: NSAIDs, aspirin, ADP receptor blockers, anticoagulants
- Family history: coagulation disorders1,6-7
Clues that the patient might be suffering from a posterior bleed include: the patient is an adult (children nearly always suffer from anterior epistaxis secondary to digital trauma or foreign body8), and he/she presents with symptoms of nausea, hematemesis, and hemoptysis in addition to, or in the absence of, epistaxis.2,3,7 Physical exam findings concerning for posterior epistaxis include blood draining from the bilateral nares, and large volumes of blood in the oropharynx.2,7 An inability to visualize an anterior source of bleeding on physical exam, and persistent bleeding despite the application of anterior nasal packing should also raise suspicion for a posterior source.2,3,7
If the patient presenting with epistaxis is unstable, appropriate intervention should be taken (preparation for a definitive airway, IV access, monitor placement, fluid resuscitation, CBC, coagulation panel, type and cross versus type and screen as appropriate).
Addressing Posterior Epistaxis
At this point, as we return to our patient, we’ll assume that he’s blown his nose, and cleared his nasopharynx of blood and clot, but due to the volume of blood actively draining from his nares, you’ve been unsuccessful in localizing an anterior source of bleeding. Your attempts at medical treatment with topical vasoconstrictors (oxymetazoline and LET soaked gauze pledgets (lidocaine 4%, epinephrine 0.1%, and tetracaine 0.4%)) have failed to obtain hemostasis, and despite placing a Rapid Rhino anterior nasal pack, the patient continues to bleed around the nasal pack and into his oropharynx. At this point, it is likely that the patient’s episode of epistaxis is originating from the posterior oropharynx. After removing his anterior packing, and once again clearing the blood and clots from the nares and oropharynx, a number of management options may be chosen:
A quick note: Analgesia should be provided prior to the application of nasal packing. It is also advised that after packing is placed, pulse oximetry be maintained to monitor for hypoxia.3
Methods for Obtaining Hemostasis
Nasal Tampons: Commonly composed of cotton or foam, numerous models of nasal tampons are available in the US for the control of epistaxis. Merocel manufactures one such model, composed of foam, designed for insertion along the septal floor, parallel to the hard palate, and offering direct mechanical pressure upon expansion (secondary to absorption of blood in the nasal cavity).9
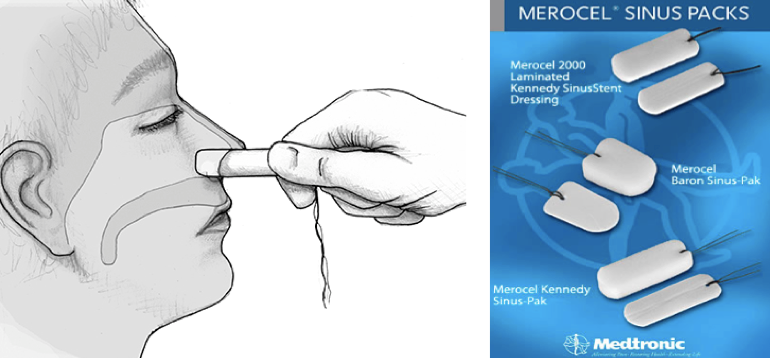
Figure 2 – Commercial Nasal Tampon9
The Rhino Rocket, a second example of a nasal tampon, was designed by Shippert Medical Technologies Incorporated for ease of application through the utilization of its patented nasal applicator.10
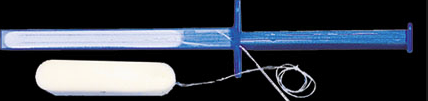
Figure 3 – Rhino Rocket10
Balloon Devices:
The Rapid Rhino – the Rapid Rhino is an inflatable balloon, coated with a hydrocolloid of carboxymethylcellulose (CMC). In addition to providing direct mechanical pressure, the Rhino’s CMC functions as a lubricator (ease of application) and platelet aggregator upon exposure to water. In order to place the Rapid Rhino (activate the CMC), the device is submerged in sterile water for approximately 30 seconds prior to its insertion along the septal floor, parallel to the hard palate. A 20cc syringe is then used to inflate the balloon until the pilot cuff is rounded and firm to the touch.2,3,12
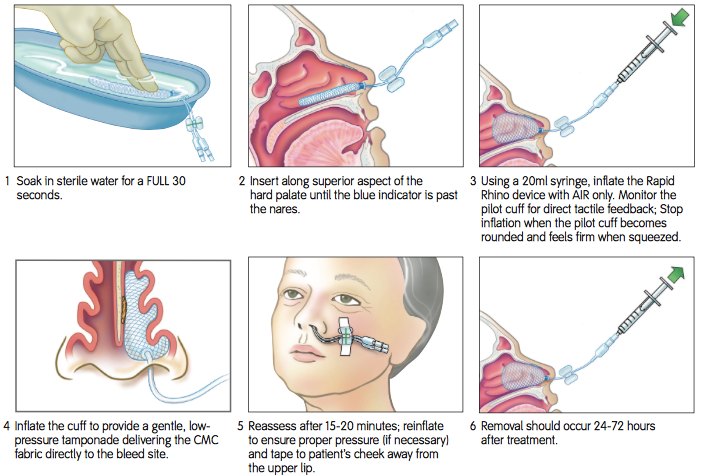
Figure 4 – Utilization of the Rapid Rhino Anterior Nasal Pack13
Rapid Rhinos are commercially available in numerous sizes: 4.5cm for children, 5.5cm and 7.5cm for anterior epistaxis in adults, 9cm for sphenopalantine artery bleeds, and 5.5cm and 7.5cm bilateral nares models for bilateral bleeds.13
Note: Despite their equivalence in obtaining hemostasis, randomized control trials have demonstrated the Rapid Rhino as superior to the Rhino Rocket in terms of pain upon insertion and ease of extraction.3,13-14
Placement of A Foley Catheter – Cited as the most commonly utilized posterior nasal packing device, a Foley catheter (size 10, 12, or 14 French) is lubricated and advanced until the tip and balloon are in the nasopharynx. The Foley balloon is then filled with approximately 5-10cc of saline and traction is applied until the balloon sits firmly against the posterior nasal choana. Anterior traction is maintained with the placement of an umbilical or c-clamp at the nasal ala.14,15 If hemostasis is not achieved status post placement of the Foley catheter, anterior nasal packing may be utilized as an adjunct.2 Appropriate application of the umbilical or c-clamp is essential to preventing the complication of pressure necrosis (detailed below). Neither the umbilical clamp nor the c-clamp should be affixed directly to the nasal ala.
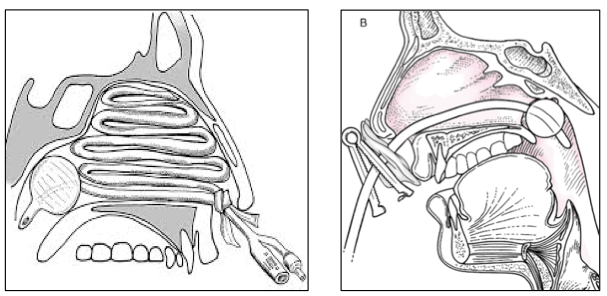
Figure 5 – Application of a Foley Catheter in Posterior Epistaxis14,15
A quick tutorial on the placement of anterior packing as cited by Kucik and Cleney, 2005:
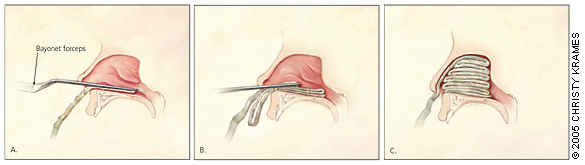
Figure 6 – Application of Anterior Packing. A. Gauze impregnated with petroleum jelly is gripped with forceps and inserted into the anterior nasal cavity. B. With a nasal speculum (not shown) used for exposure, the first packing layer is inserted along the floor of the anterior nasal cavity. Forceps and speculum are then withdrawn. C. Additional layers of packing are added in accordion-fold fashion, with the nasal speculum used to hold the positioned layers down while a new layer is inserted. Packing is continued until the anterior nasal cavity is filled.2
The Epistat or Storz T3100 – As an alternative to the Foley catheter, the Epistat or Storz t3100 is a device with anterior and posterior balloons for the control of epistaxis. The device is inserted until the posterior balloon enters the posterior nasal cavity, inflated with 5-10cc of saline, and then pulled forward until snug. The anterior balloon is then filled with 15-30cc of saline and secured with an umbilical or c-clamp at the nasal ala.3,17
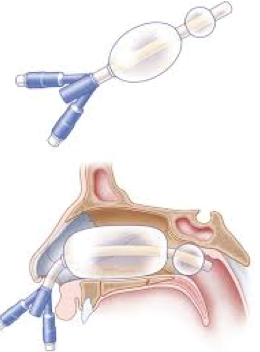
Figure 7 – Storz T310017
Posterior Nasal Packing
While rarely employed in the emergency department secondary to its difficulty in application, posterior nasal packing is also cited in the literature as a mechanism of controlling posterior epistaxis.2,3
Again as depicted by Kucik and Cleney, 2005:
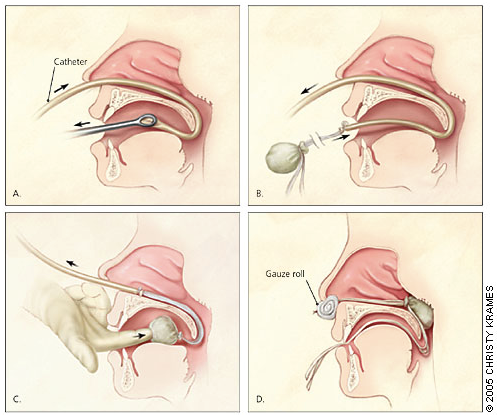
Figure 8 – Application of Posterior Nasal Packing. A. After anesthesia is obtained, a catheter is passed through the affected nostril and through the nasopharynx, and drawn out the mouth with the aid of ring forceps. B. A gauze pack is secured to the end of the catheter using umbilical tape or suture material, with long tails left to protrude from the mouth. C. The gauze pack is guided through the mouth and around the soft palate using a combination of careful traction on the catheter and pushing with a gloved finger. (A bite block, not shown, should be used to protect the physician’s finger). D. The gauze pack should rest in the posterior nasal cavity. It is secured in position by maintaining tension on the catheter with a padded clamp or gauze roll placed anterior to the nostril. Ties protruding from the mouth (used to remove the pack) should be secured to the patient’s cheek.2
Complications of Methods for Obtaining Hemostasis
Complications associated with posterior nasal packing include patient discomfort, otitis media, sinus obstruction, pressure necrosis of the nasal mucosa and cartilage, pressure necrosis of the nasal ala (if packing secured inappropriately), hypoventilation, and toxic shock syndrome (TSS). 1,18
Major adverse events including myocardial infarction and death have also been reported as complications of posterior nasal packing.1,17 Early literature (1980s-early 1990s) attributed these events to a nasopulmonary reflex – a postulated change in nasopulmonary function secondary to posterior nasal packing, resulting in a decrease in arterial oxygen content.18-20 Today, however, the existence of the reflex is controversial as the majority of studies now cite vagal nerve stimulation, symptomatic anemia, recurrent bleeding resulting in apnea and concomitant hypoxia, and over-sedation secondary to analgesia as the likely etiologies of the aforementioned complications. 18-20
TSS – An aside regarding TSS and antibiotic therapy in the setting of nasal packing: Case reports and case reviews regarding epistaxis management favor the lubrication of nasal tampons/gauze with antibiotic ointment, and the provision of systemic antibiotics post packing in order to prevent the occurrence of TSS secondary to S. aureaus infection. Several studies cite a reduction in nasal colonization by Staph species and decreased incidence of post-packing sinusitis when topical and systemic antibiotic therapy is utilized.2,21 As the literature regarding this topic is immense and not addressed entirely in this review; suffice it to say that the ACEP Clinical Practice Management Guide on Epistaxis recommends the application of topical antibiotic ointment, and the provision of systemic antibiotic therapy.2 This is a controversial practice; see here: http://rebelem.com/do-patients-with-epistaxis-managed-by-nasal-packing-require-prophylactic-antibiotics/
Recommended Adult Antibiotic Regimens Include:
First Line: PO cephalexin 250–500 mg QID or PO amoxicillin/clavulanate 250–500 mg TID
Second line: PO clindamycin 150–300 mg QID or PO trimethoprim/sulfamethoxazole DS
Therapy should be continued for 7-10 days.3,21
Patient Disposition
All patients requiring posterior packing should be admitted to the hospital given the risk of hypoxia occurring after packing, and the necessity to monitory for dysrhythmias and recurrent bleeds. If not already completed, a CBC and coagulation panel should be obtained, in addition to studies considered pertinent given the patient’s H&P (bleeding time, factor assays, etc.). ENT consultation is required as nasal packing is commonly removed within 48-72 hours.2,3,7 Patients refractory to the hemostatic measures described above require urgent vs. emergent ENT evaluation for endoscopic assessment with the potential for ligation or embolization.2,7
Extra Credit: Hypertension and Epistaxis – Cause and Effect?
The association between hypertension and epistaxis is complex. To date, studies have failed to demonstrate a causal relationship between hypertension and epistaxis. Data regarding an association between hypertension and epistaxis varies widely.3,22-24 At least one retrospective cohort study of a Marshfield, Ohio clinic, performed by Abrich, et al., 2014, (n = 431) demonstrated hypertension as a risk factor for epistaxis and recurrent epistaxis.22
A systematic review performed by Kikidis, et al., 2014, (EMBASE, Medline, and Ovid SP search of hypertension and epistaxis, Jan1975 – Jan 2012) revealed 6 of 9 total studies (n = 2,994) identifying the presence of hypertension in patients with epistaxis. As the authors identify, however, “the presence of high arterial blood pressure during the actual episode of nasal bleeding cannot establish a causative relationship with epistaxis, because of confounding stress and possible white coat phenomenon.”24
Given the lack of a direct causal relationship between hypertension and epistaxis, epistaxis therapy should focus on control of the hemorrhage rather than reduction of the blood pressure.3 As ACEP identifies, the provision of analgesia and mild sedation are preferable to antihypertensive therapy.3
References / Further Reading
- Viehweg T, Rogerson J, Hudson J. Epistaxis: diagnosis and treatment. J Oral Maxillofac Surg. 2006; 64:511-8.
- Kucik C, Clenney T. Management of epistaxis. Am Fam Physician. 2005;71(2):305-311.
- Gilman C. Focus on: treatment of epistaxis. American College of Emergency Physicians. Clinical & Practice Mangement. 2009. Available at https://www.acep.org/Clinical—Practice-Management/Focus-On–Treatment-of-Epistaxis/
- Bent J, Woods B. Complications resulting from treatment of severe posterior epistaxis. J Laryngol Otol. 1999;113(3):252-254.
- Ho E, Mansell N. How we do it: a practical approach to foley catheter posterior nasal packing. Clin Otolaryngol Allied Scie. 2004;29(6):754-757.
- Elahi M, Parnes L, Fox A, Pelz D, Lee D, et al. Therapeutic embolization in the treatment of intractable epistaxis. Arch Otolaryngol Head Neck Surg. 1995; 121(1):65-69.
- Yau, S. An update on epistaxis. AFP. 2015; 44(9):653-656.
- Douglas R, Wormwald P. Update on epistaxis. Curr Opin Otolaryngol Head Neck Surg. 2007;15:180-183.
- Merocel products. Medtronic. 2012. Available at http://www.merocel.com/products/index.htm
- Rhino rocket with applicator. Shippert Medical Technologies Incorporated. 2014. Available at https://www.shippertmedical.com/rhino-rocket-with-applicator.html
- Tan L, Calhoun K. Epistaxis. Med Clin North Am. 1999;83:43-56.
- Liudvikas J, Daniel M. Mangement of Epistaxis in the emergency department. Emergency Medicine Reports. 2006. Available at http://www.ahcmedia.com/articles/122580-management-of-epistaxis-in-the-emergency-department
- Rhapid rhino epistaxis products. Smith & Nephew, Incorporated. 2015. Available at http://www.kebomed.no/files/78/smith_nephew_rapid_rhino.pdf
- Singer A, Blanda M, Cronin K, LoGiudice-Khwaja M, Gulla J, Bradshaw J, et al. Comparison of nasal tampons for the treatment of epistaxis in the emergency department: a randomized control trial. Ann Emerg Med. 2005; 45(3):134-139.
- Reichman E. 2013. Chapter 172: Epistaxis management. Tintinalli’s Emergency Procedures 2e. Chapel Hill, NC, McGraw-Hill Holdings, LLC
- Thomas L, Karagama Y, Watson C. Avoiding alar necrosis with post-nasal packs. J Laryngol Otol. 2005;119(9):727-728.
- Halverson, D, Borgstrom. 2015. Chapter 16: Epistaxis. Advanced Surgical Techniques for Rural Surgeons. Springer Science+Business Media New York
- Monte E, Belmont M, Wax M. Mangement paradigms for posterior epistaxis: a comparison of costs and complications. Otolaryngol Head Neck Surg.1999;121:103-106.
- Jacobs J, Levine L, Davis H, Lefrak S, Druck N, et al. Posterior packs and the nasopulmonary reflex. Laryngoscope. 1981;91(2):279-284.
- Loftus B, Blitzer A, Cozine K. Epistaxis, medical history, and the nasopumonary reflex: what is clinically relevant? Otolaryngol Head Neck Surg. 1994; 110(4):363-369.
- Rubin J, Rood S, Myers E, Johnson J. The management of epistaxis. Self-instructional package. Alexandria, Va.: American Academy of Otolaryngology-Head and Neck Surgery 1990
- Abrich V, Brozek A, Boyle T, Chyou P, Yale S. Risk factors for recurrent spontaneous epistaxis. Mayo Clinic Proceedings. 2014;89(12):1636-1643.
- Sarhan N, Algamal A. Relationship between epistaxis and hypertension: A cause and effect or coincidence? J Saudi Heart Assoc. 2015;27(2):79-84.
- Kikidis D, Tsioufis K, Papanikolaou V, Zerva K, Hantzakos A. Is epistaxis associated with arterial hypertension? A systemic review of the literature. Eur Arch Otorhinolaryngol. 2014; 271(2):237-243.






3 thoughts on “The Emergency Department Management of Posterior Epistaxis”
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM: Epistaxis - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationThe EM Educator Series: Nosebleed that won’t stop - emDOCs.net - Emergency Medicine Education
Pingback: Epistaxis – The Good Doctor