Author: Anna Pickens, MD (@AnnaEMin5, Creator of EMin5) // Reviewed by: Alex Koyfman, MD (@EMHighAK), Brit Long, MD (@long_brit), and Manpreet Singh, MD (@MprizzleER)
Welcome to this week’s edition of EMin5 by Dr. Anna Pickens. Today we review what to do when a health care worker comes to the ED with a needlestick injury!
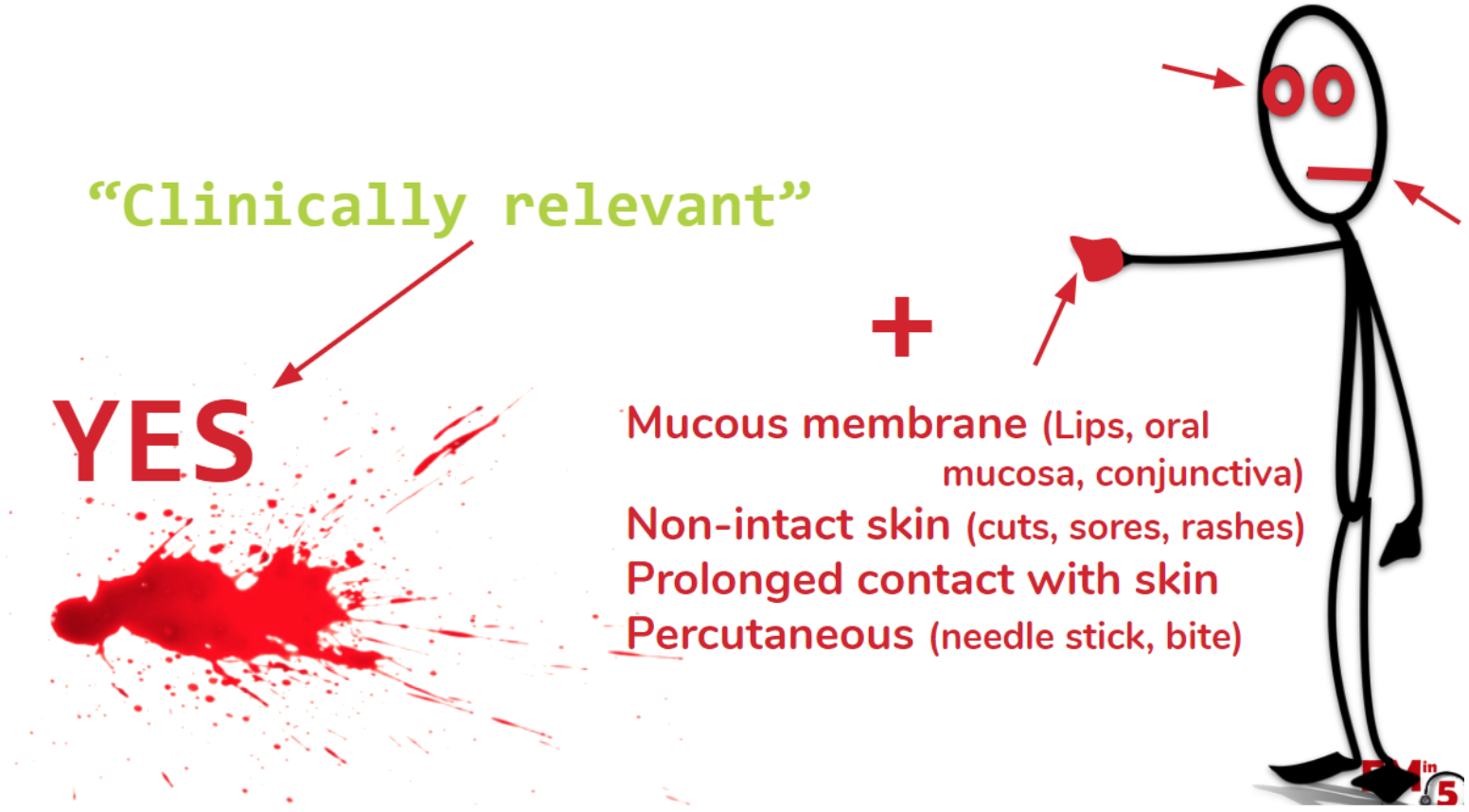
The first thing to consider is whether or not this is a clinically relevant exposure, and therefore if the health care worker even needs prophylaxis.
If the exposure is to intact skin, to any of the following, the answer is no, and the patient can be discharged. Easy!

If the exposure is from any of these fluids:

And comes in contact with mucous membranes, non-intact skin, prolonged exposure ot the skin, or is from a percutaneous injury, then the answer is YES, this is clinically relevant. And you need to go on to consider if the patient needs PEP.
Provide local wound care and make sure to document the important info:


Then draw the following labs on both the health care worker and the source patient (if availble):

And make sure the patient’s tetanus is up to date:

Here’s some food for thought to tell your patient about their risk:

(One take-away: The Hep B vaccine is amazing!)
The good news for Hep B and HIV is that PEP can go a long way to reduce risk of transmission:

Take-away #2: Hep C is kind of a bummer. There is no vaccine and no PEP, so follow up in 48 hrs with employee health.

Hep B:
There is a complicated chart from the CDC on how to decide who needs PEP for Hep B… BUT don’t get too down about it. We don’t actually need to know a lot of this in the ED setting (see below).
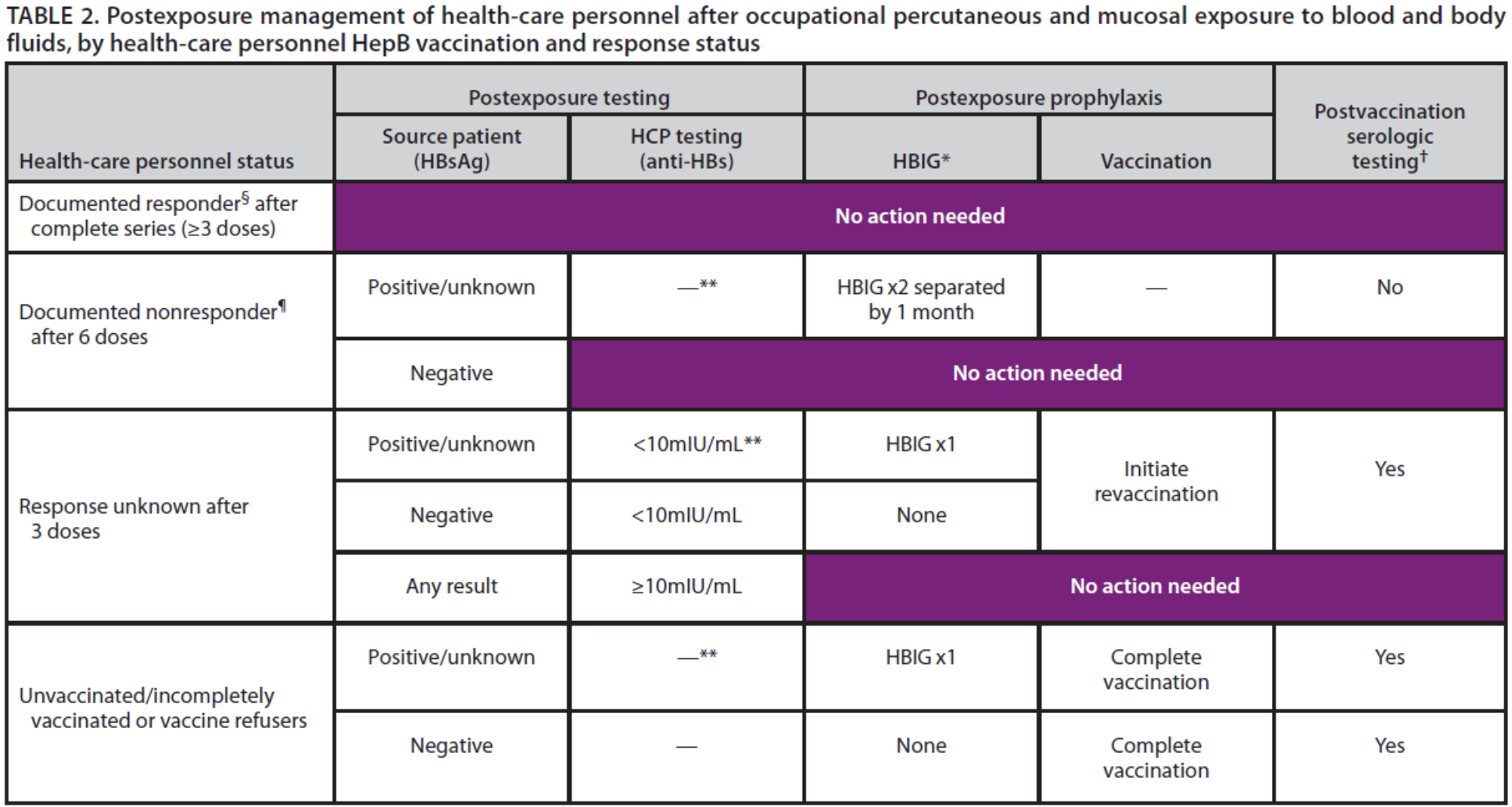
(but this is more important for employee health / ID / follow up purposes)
HERE’s the quick and dirty of what you need to know in the ED:

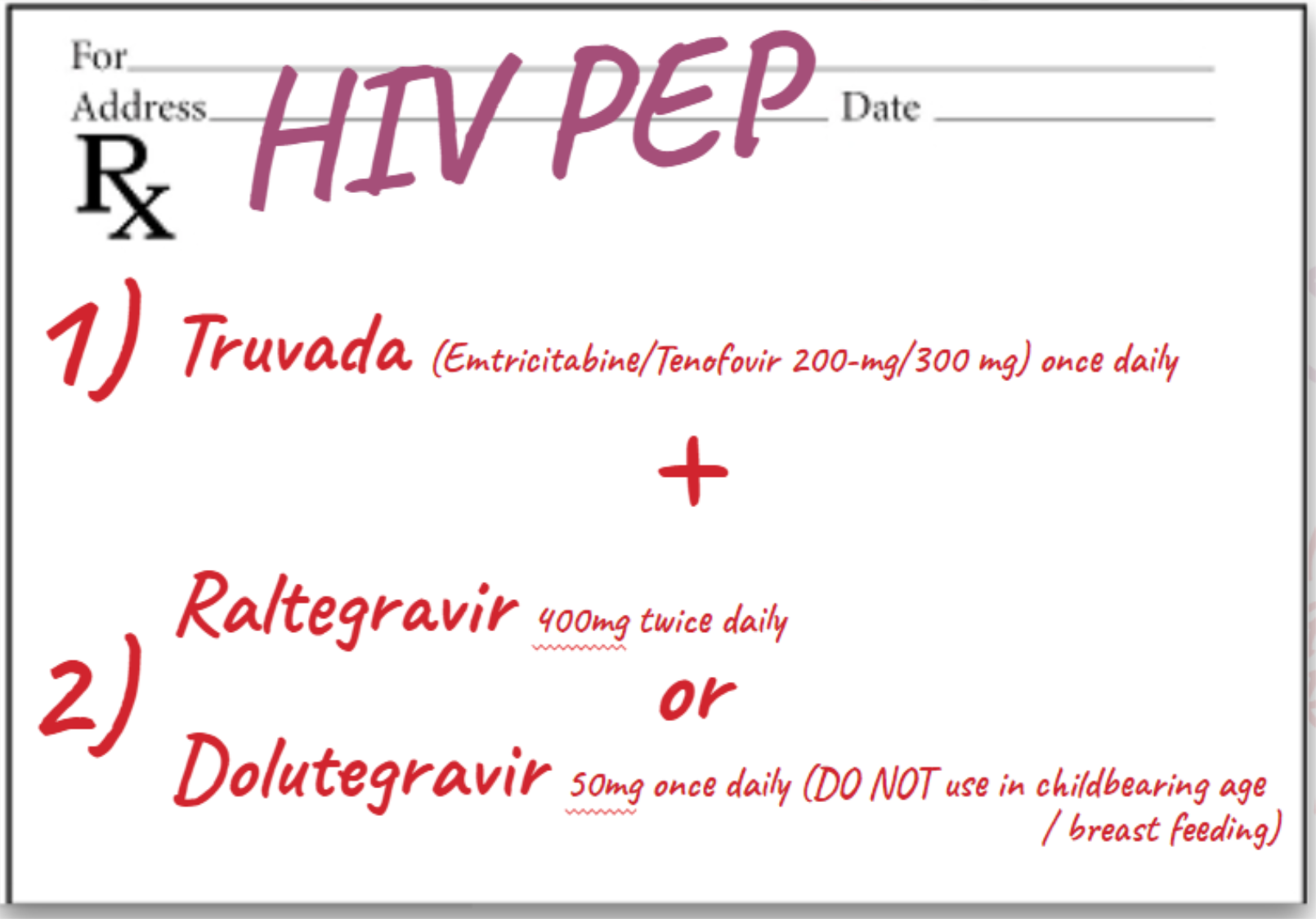
For HIV exposure / PEP:

** note that the first dose of PEP should be given in the ED.
Here’s an example of what to prescribe them for the next 5 days (although your hospital may have their own preference for a regimen):
And most important, make sure your patient knows that this is just the beginning. The next step is for them to follow up with ID or Employee Health to continue the evaluation, obtain results, and ensure appropriate therapy.
Have them follow up in 48 hours!

Have a question about a strange case or need help deciding on what to do?
Call the PEP hotline, specifically for health care providers in this situation:

Questions you may have for them:

Here’s the recap:

Suggested/Further Reading:
https://www.cdc.gov/niosh/topics/bbp/emergnedl.html
https://litfl.com/needle-stick-injuries/
https://coreem.net/journal-reviews/hiv-pep/





