Authors: Brit Long, MD (@long_brit) and Summer Chavez, DO, MPH, MPM (Health Policy Fellow, Georgetown University/Medstar) // Reviewed by: Alex Koyfman, MD (@EMHighAK)

In December 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) resulted in an epidemic beginning in Wuhan, China. This illness, known as Coronavirus Disease 2019 (COVID-19), has now spread internationally with over 5000 deaths.
COVID-19 most commonly results in cough, fever, and shortness of breath, though patients may also experience sore throat, headache, and gastrointestinal symptoms. At this point, a patient presenting to the ED should be presumed to have COVID-19. A small percentage of patients develop septic shock and even acute respiratory distress syndrome (ARDS), typically one week after the first onset of symptoms. Patients with comorbidities and older age are the most likely to have severe disease.
This post will not focus on screening, history/exam, testing, or management of stable patients. Instead, we will focus on management of the critically ill patient with COVID-19 by discussing the recently published Society of Critical Care Medicine and European Society of Intensive Care Medicine Guidelines. These are available at https://www.sccm.org/getattachment/Disaster/SSC-COVID19-Critical-Care-Guidelines.pdf?lang=en-US
The end of the post will contain a list of stellar #FOAMed resources for your use.
Infection Control
Recommendation: If performing an aerosol-generating procedure (intubation, administrating nebulized therapy, manual ventilation prior to intubation), they recommend using a fitted respiratory mask (N95) as opposed to surgical/medical masks with other personal protective equipment (PPE) (best practice statement).
Recommendation: They recommend performing aerosol-generating procedures in a negative pressure room if able (best practice statement).
Recommendation: If performing usual care or other non-aerosol generating procedures, they suggest using a surgical/medical mask (weak recommendation, low quality evidence).
Recommendation: For providers performing intubation, they suggest using video-guided laryngoscopy over direct laryngoscopy if able (weak recommendation, low quality evidence).
Recommendation: For patients requiring intubation, they recommend that the most experienced provider intubate to reduce the number of attempts and transmission risk (weak recommendation, low quality evidence).
Laboratory Diagnosis
Approximately 5% of patients with COVID-19 are critically ill, with approximately 1% developing septic shock. However, the incidence is higher in hospitalized patients. Cardiac injury may occur in 7-23% of patients.
Recommendation: In patients with COVID-19 with shock, they suggest using dynamic parameters such as skin temperature, capillary refill time, and/or serum lactate over static parameters to assess fluid responsiveness (weak recommendation, low quality evidence).
Supportive Care
Approximately 5% of patients with COVID-19 are critically ill, with approximately 1% developing septic shock. However, the incidence is higher in hospitalized patients. Cardiac injury may occur in 7-23% of patients.
Recommendation: In patients with COVID-19 with shock, they suggest using dynamic parameters such as skin temperature, capillary refill time, and/or serum lactate over static parameters to assess fluid responsiveness (weak recommendation, low quality evidence).
Fluid Therapy
Recommendation: For acute resuscitation of adults with COVID-19 and shock, they suggest using a conservative over liberal fluid strategy (weak recommendation, very low quality evidence).
Recommendation: They recommend using crystalloids rather than colloids (weak recommendation, low quality evidence).
Recommendation: They suggest using buffered/balanced crystalloids rather than unbalanced crystalloids (weak recommendation, moderate quality evidence).
Recommendation: They recommend against using hydroxyethyl starches for the resuscitation of patients with shock (strong recommendation, moderate quality evidence).
Recommendation: They suggest against using gelatins or dextran for resuscitation (weak recommendation, low quality evidence).
Recommendation: They suggest against routine use of albumin for initial resuscitation (weak recommendation, moderate quality evidence).
Vasoactive Agents:
Recommendation: They suggest using norepinephrine as the first-line vasopressor (weak recommendation, low quality evidence).
Recommendation: If norepinephrine is not available, they suggest using either vasopressin or epinephrine for the first-line vasopressor (weak recommendation, low quality evidence).
Recommendation: If norepinephrine is available, they recommend against using dopamine (strong recommendation, high quality evidence).
Recommendation: Rather than titrating norepinephrine if mean arterial pressure (MAP) cannot be reached with norepinephrine alone, they suggest adding vasopressin (weak recommendation, moderate quality evidence).
Recommendation: They suggest titrating vasopressors to a target MAP of 60-65 mm Hg (weak recommendation, low quality evidence).
Recommendation: For those with evidence of cardiac dysfunction and persistent hypoperfusion despite fluid and norepinephrine, they suggest adding dobutamine rather than increasing norepinephrine dose (weak recommendation, very low quality evidence).
Recommendation: For those with refractory shock, they suggest using low-dose corticosteroid therapy over no corticosteroid therapy (weak recommendation, low quality evidence). Hydrocortisone 200 mg per day by infusion or intermittent doses is recommended.
*Ventilatory Support
Recommendation: They suggest starting supplemental oxygen if saturation is < 92% (weak recommendation, low quality evidence) and recommend it if < 90% (strong recommendation, moderate quality evidence).
Recommendation: For those with acute hypoxemic respiratory failure on oxygen, they recommend titration oxygen saturation no higher than 96% (strong recommendation, moderate quality evidence).
Recommendation: For those with acute hypoxemic respiratory failure despite oxygen therapy, they suggest using high flow nasal cannula (HFNC) over conventional oxygen therapy (weak recommendation, low quality evidence).
Recommendation: For those with acute hypoxemic respiratory failure, they suggest using HFNC over NIPPV (weak recommendation, low quality evidence).
Recommendation: For those with acute hypoxemic respiratory failure but HFNC is not available, they suggest a trial of NIPPV with close monitoring (weak recommendation, very low quality evidence).
Recommendation: For those receiving HFNC or NIPPV, they recommend close monitoring for worsening respiratory status and early intubation if status worsens (best practice statement).

*Invasive Mechanical Ventilation
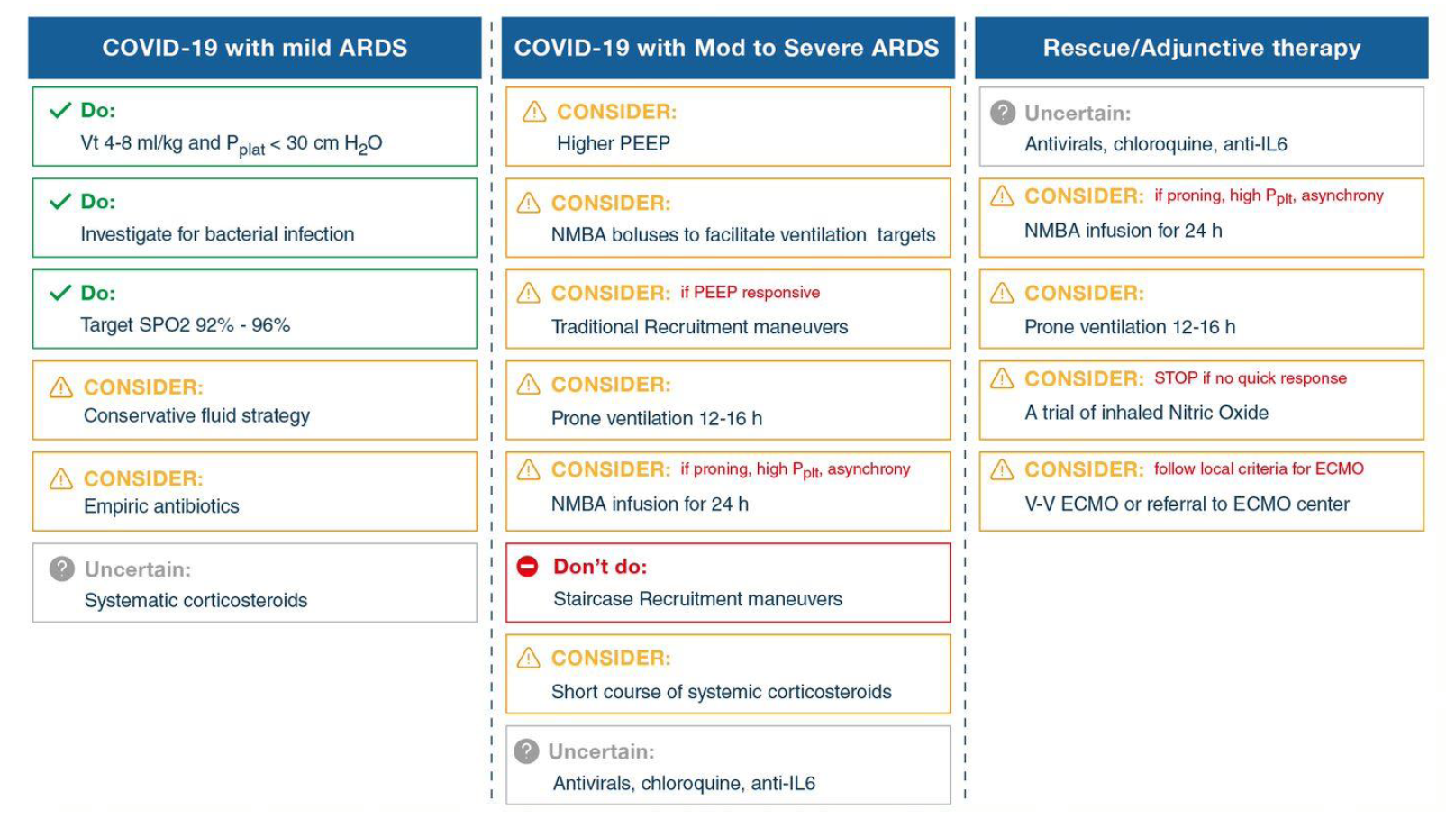
Recommendation: In mechanically ventilated patients with COVID-19 and ARDS, they recommend using low tidal volume ventilation (4-8 mL/kg of predicted body weight) over higher tidal volumes (strong recommendation, moderate quality evidence).
Recommendation: They recommend targeting plateau pressures of < 30 cm H20 (strong recommendation, moderate quality evidence).
Recommendation: In mechanically ventilated patients with COVID-19 and moderate to severe ARDS, they recommend using a higher PEEP strategy over a lower PEEP strategy (weak recommendation, low quality evidence).
Recommendation: For those with COVID-19 and ARDS, they suggest using a conservative fluid strategy over a liberal strategy (weak recommendation, low quality evidence).
Recommendation: In mechanically ventilated patients with COVID-19 and ARDS, they suggest prone ventilation for 12-16 hours over no prone ventilation (weak recommendation, low quality evidence).
Recommendation: For those with COVID-19 and moderate to severe ARDS, they suggest using intermittent boluses of neuromuscular blocking agents (NMBA) over continuous NMBA infusion (weak recommendation, low quality evidence). They suggest using continuous NMBA infusion for up to 48 hours for those with persistent ventilator dyssynchrony, the need for ongoing deep sedation, prone ventilation, or persistently high plateau pressures (weak recommendation, very low quality evidence).
Recommendation: In mechanically ventilated patients with COVID-19 and ARDS, they suggest against the routine use of inhaled nitric oxide (strong recommendation, low quality evidence).
Recommendation: In mechanically ventilated patients with COVID-19, severe ARDS and hypoxemia despite other strategies, they suggest a trial of inhaled pulmonary vasodilator therapy. If no improvement is found, the treatment should be tapered off (weak recommendation, very low quality evidence).
Recommendation: In mechanically ventilated patients with hypoxemia despite optimizing ventilation, they suggesting using recruitment maneuvers over not recruitment maneuvers (weak recommendation, low quality evidence). They recommend against using incremental PEEP recruitment maneuvers (strong recommendation, moderate quality evidence).
Recommendation: For those with refractory hypoxemia despite ventilation optimization, rescue therapies, and proning, they suggest using venovenous ECMO if available, or referring to an ECMO center (weakrecommendation, low quality evidence).
COVID-19 Therapy
*Recommendation: For mechanically ventilated patients with COVID-19 and respiratory failure but no ARDS, they suggest against routine use of systemic corticosteroids (weak recommendation, low quality evidence). For those with ARDS, they suggest using systemic corticosteroids (weak recommendation, low quality evidence).
Recommendation: For mechanically ventilated patients with COVID-19 and respiratory failure, they suggest using empiric antibiotics over no antibiotics (weak recommendation, low quality evidence).
Recommendation: For critically ill adults who develop fever, they suggest using acetaminophen for temperature control over no therapy (weak recommendation, low quality evidence).
Recommendation: For critically ill adults, they suggest against standard use of IVIG (weak recommendation, low quality evidence).
Recommendation: For critically ill adults, they suggest against routine use of convalescent plasma (weak recommendation, low quality evidence).
Recommendation: For critically ill adults, they suggest against routine use lopinavir/ritonavir (weak recommendation, low quality evidence). There is insufficient evidence to issue a recommendation on other antivirals in critically ill patients.
There is insufficient evidence to provide a recommendation on use of recombinant interferons (rIFNs), alone or in combination with antivirals, in critically ill adults with COVID-19.
There is insufficient evidence to provide a recommendation on use chloroquine or hydroxychloroquine in critically ill adults with COVID-19.
There is insufficient evidence to provide a recommendation on use of tocilizumab in critically ill adults with COVID-19.
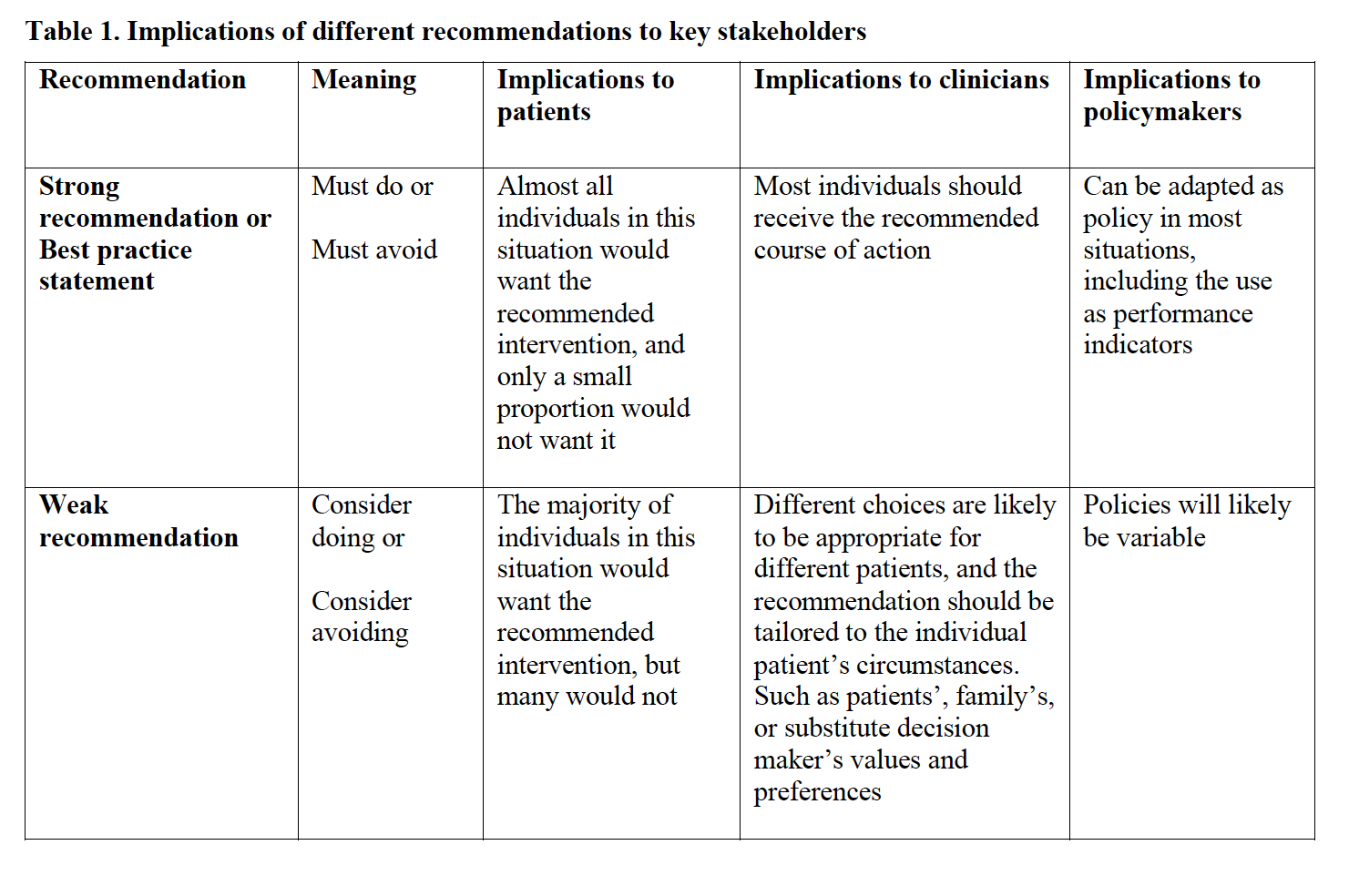
Recommendation Interpretation
*Update:
Based on the RECOVERY trial published in the New England Journal of Medicine, patients requiring supplemental oxygen or mechanical ventilation should receive dexamethasone, 6 mg (PO or IV), which is associated with reduced mortality.
HFNC has proven safe and improves patient comfort. This can improve respiratory fatigue and oxygenation.
Do not just focus on the oxygen saturation in determining need for intubation. Consider mental status, work of breathing, and diaphoresis in your evaluation.
Proning/awake repositioning improves oxygen saturation and reduces pulmonary ischemia. It remains controversial whether it improves lung recruitment in a significant manner.
IDSA treatment recommendations as of December 10, 2020:
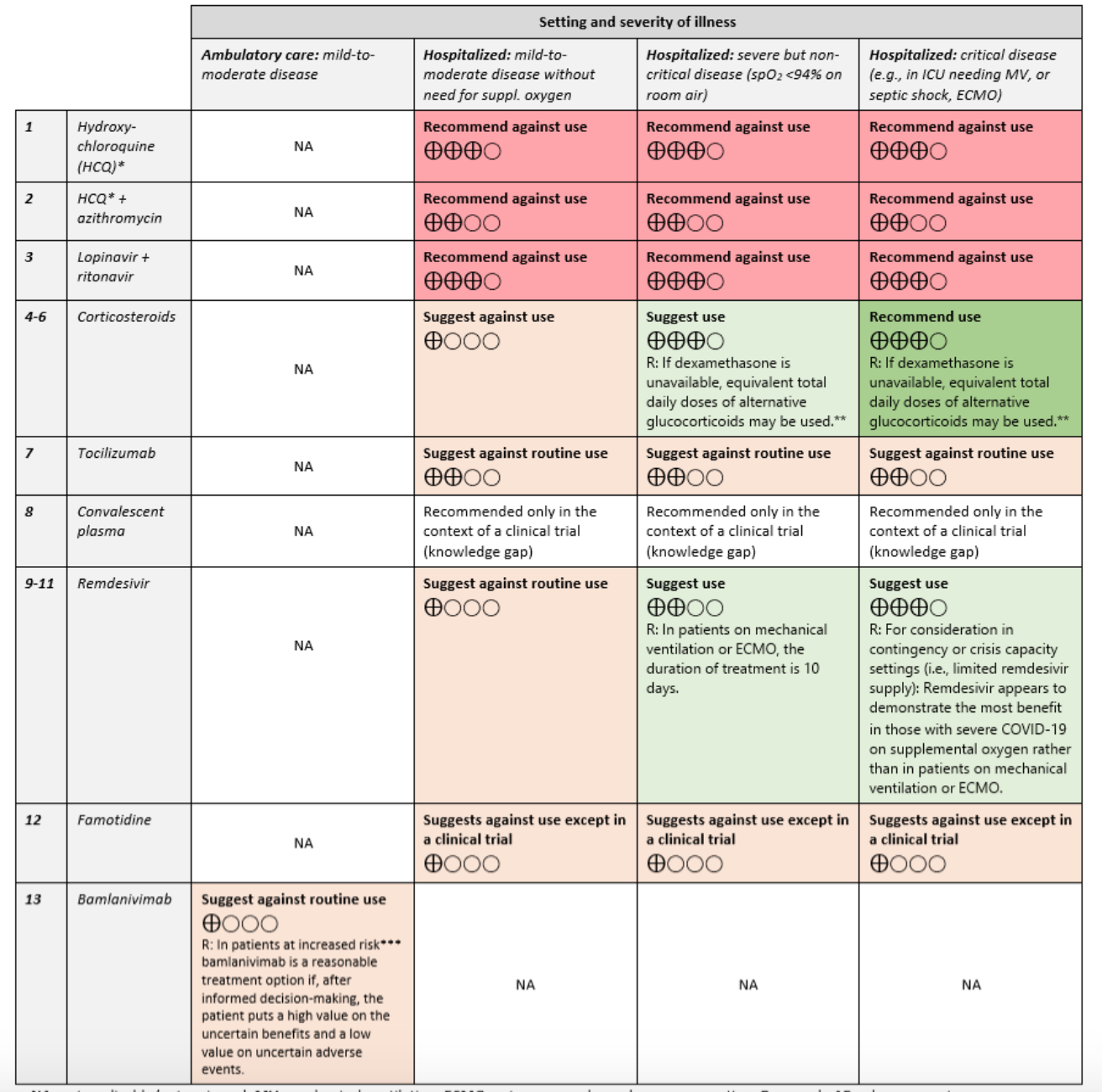
Hydroxychloroquine/chloroquine alone or in combination with azithromycin are not recommended. Lopinavir and ritonavir are also not recommended.
From Dr. Katy Hanson at Hanson’s Anatomy:

Other #FOAMed resources:
- Hippo ED Resources
- Journal Feed
- Emergency Medicine Cases on Screening, Diagnosis and Management
- COVID-19 chapter in the Internet Book of Critical Care
- REBEL EM COVID page
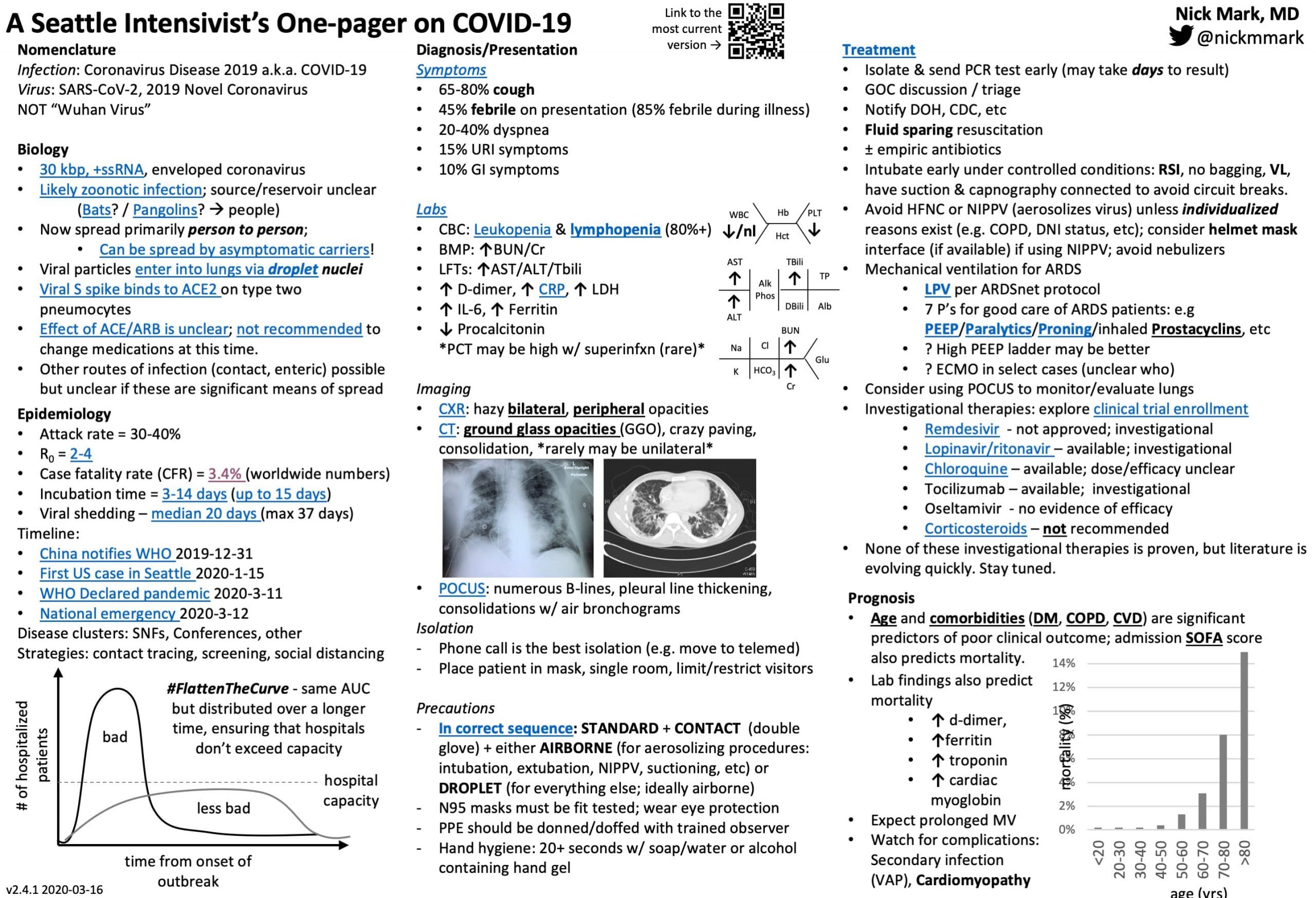
- COVID one-pager from Seattle intensivist
- Surviving Sepsis COVID Guidelines March 19th, 2020.
- Strategies for Optimizing the Supply of N95 Respirators during the COVID-19 Response
- ACEP wellness assistance program – 3 free counseling sessions for ACEP members
- How to make a reuseable respirator as a replacement for N95 mask
- Evidence based summary of pediatric COVID-19 literature
- Video discharge instructions for patients





{kind=link}
3 thoughts on “Managing the Critical COVID-19 Patient – SCCM Guidelines”
Pingback: COVID 19 – Diagnostik & Therapie – Notfallmedizin/ EMcare
Hi Brit,
thanks for your synopsis.
A comment about ventilation management.
In our experience on 900 admitted pneumonias since 21st February, more than 30% need an FiO2 > 50%.
Among them, we observed that those who cannot reach 90% of peripheral saturation with a reservoir mask at 15 L/min respond better to Helmet CPAP than to HFNC, since PEEP application determines alveolar recruitment and prompt oxygenation increase.
The risk with CPAP use is to delay intubation or perpetuate the SILI occurring with patient respiratory efforts.
The advantage is to treat patients immediately with symptom relief and improved oxygenation without admitting patients to ICU which is the most critical resource in this huge surge of COVID outbreak.
Good luck
@rob_cosentini
Respiratory Drive in the Acute Respiratory Distress Syndrome: Pathophysiology, Monitoring, and Therapeutic Interventions
Elena Spinelli , Tommaso Mauri , Jeremy R Beitler, Antonio Pesenti, Daniel Brodie PMID: 32016537 DOI: 10.1007/s00134-020-05942-6
Pingback: Surviving Sepsis Campaign Guidelines on the Management of Critically Ill Adults with COVID-19 - REBEL EM - Emergency Medicine Blog