Authors: Subhanir Sunil Chitnis, MD (@ChitnisMD, EM Resident Physician, Rutgers NJMS), Dawn Kabba, MD (EM Resident Physician, Rutgers NJMS), and Miriam Kulkarni, MD (EM Attending Physician, Rutgers NJMS) // Edited by: Alex Koyfman, MD & Justin Bright, MD
Introduction
- Calcium oxalate (and to some degree calcium phosphate) stones account for 80% of all kidney stones
- Remaining stones are uric acid (10%), struvite (10-15%) and cystine (1%) stones
- It is possible for patient to have multiple stones and for them to be more than one type of stone
Epidemiology
- Prevalence in the US is 5%, with annual incidence of 0.5-1%
- Lifetime risk is about 10%, male predominance of 2:1
- Average age is 20, with range from 20-50, and first occurrence is rarely after 60
- In pediatric population, sex distribution is 1:1, with 50% due to metabolic abnormalities, 20% due to urologic anomalies, and 15% due to infection
Risk Factors
- Crystallization occurs when otherwise soluble solutes precipitate due to supersaturation or changes in urinary pH, protein content, or due to reaction with other solutes
- Crystals cause epithelial injury, deposition of stone formation, bleeding, obstruction, and pain
- Frequently identified risk factors include hypercalciuria, hyperoxaluria, hypocitraturia, decreased calcium intake, increased oxalate intake, increased animal protein intake, and decreased hydration
- There is more than 2-fold increase in risk of kidney stones with positive family hx of kidney stones
- Patients with history of kidney stones have a 10-30% 3-5 year recurrence rate
- 25% of people with gout will get kidney stones
Signs and Symptoms
- Classic presentation is severe acute intermittent flank pain lasting 20-30 minutes per episode with radiation to the groin, testicles, or vulva, often with hematuria
- CVA tenderness is found in approximately 50% of patients with kidney stones
- Rebound tenderness is found in 29% and guarding in 61%
- Nausea and vomiting is present in 50% of the patients
- Microscopic hematuria is present in 85% of patients; gross hematuria is seen in 30% of cases
- Frequency, urgency and dysuria occur in 3-24% of patients
- Poor outcomes are associated with diabetes, hypertension, renal insufficiency, history of complicated stone disease, urinary tract instrumentation, urinary tract infection, and single, transplanted or horseshoe kidney
Diagnosis
- Use of CT scans has increased by factor of 10-fold over the past 15 years (2, 3)
- Bedside or Radiology Department ultrasonography has lower cumulative radiation exposure, without significant differences in complications, adverse events, pain scores, return emergency department visits, or hospitalizations when compared to CT scan. (2)
- In recent study, 40.7% of patients who had point of care U/S and 27.0% of people who had radiology department U/S underwent CT scan to evaluate for stones in the ED (2)
- Mean total costs and total radiation exposures are lower when patient undergoes ultrasound, despite the additional CT scans required for some cases
- Ultrasound is the recommended test of choice, with some cases requiring CT scan where ultrasound is equivocal or additional diagnostics are required.
- For all patients with suspected or diagnosed nephrolithiasis, obtain CBC with differential (assess for infection, anemia from gross hematuria, thrombocytopenia), serum chemistry (assess for acute and/or chronic kidney injury, hyperglycemia), UA + cx (assess for crystals, evidence of infection, casts)
Differential Diagnosis
- High-risk diagnoses include: abdominal aortic aneurysm with or without rupture, pneumonia with sepsis, appendicitis with rupture, diverticulitis with abscess or perforation, bowel ischemia or perforation, renal infarction, renal stone with abscess, pyelonephritis with sepsis or bacteremia, ovarian torsion with or without necrosis, testicular torsion, aortic dissection, ectopic pregnancy with or without rupture
- Other diagnoses include: cystitis, pancreatitis, pelvic inflammatory disease, epididymitis, colitis, ovarian cysts, endometriosis, biliary colic, renal tumors, bladder tumors, ureteral tumors, ureteral strictures, malingering
- In one study evaluating 714 patients, alternate diagnoses included appendicitis (4%), pyelonephritis (2.8%), ovarian cysts (1.7%), abdominal aortic aneurysm (1.3%), cholelithiasis (5%). (5)
Management
- Pain control: either NSAIDs (toradol) or opioids (morphine, dilaudid) or combination of both.18,24,25
- NSAIDs: decrease spasm of ureter and decrease kidney capsule pressure by decreasing GFR.24,25 Use caution in those with underlying renal disease or problems with GI bleeding.7
- Opiates: fast onset.
- Combination therapy with NSAID and opiate may decrease length of stay in ED.24,7
- Antiemetics: Ondansetron (Zofran) and metoclopramide (Reglan) are commonly used. Reglan is the only antiemetic that has been studied in patients with renal colic.15,24,25 Reglan not only has antiemetic properties, but enhances the effects of analgesia. Two studies revealed that reglan provided equivalent pain relief compared to opioids.18,15
- IV hydration: routinely done, but no studies show that fluids enhance stone passage or affect outcome.24,25
- Medical expulsive therapy (MET): Alpha-1 antagonists are frequently used to relax ureteral smooth muscle cells and improve stone passage. A recent systematic review concluded that Tamsulosin (Flomax) improved stone passage when compared to placebo.9 While a few trials suggested that tamsulosin is an effective way to clear ureteral stones,9,11 other studies suggest that there is no benefit.10 So, the bottom line is that it is unclear if this is actually beneficial for the passage of renal stones, and therefore is not employed as primary management of renal colic in the Emergency Department.
Indications for admission
| ABSOLUTE INDICATIONS | RELATIVE INDICATIONS |
| *intractable pain or vomiting | fever |
| *sepsis 2/2 UTI/pyelo | obstructing stone with signs of urinary infection |
| *solitary or transplanted kidney with obstruction | solitary or transplanted kidney without obstruction |
| *Acute renal injury | urinary extravasation |
| *hypercalcemic crisis | stone unlikely to pass: >5mm and located proximal ureter |
Table 97-5 Adapted from Manthey et al., 2011.25
Does Stone Size affect Outcome?
| stone size (mm) | average # of days to passage | % likelihood of need for intervention |
| ≤ 2 | 8 | 3 |
| 3 | 12 | 14 |
| 4-6 | 22 | 50 |
| > 6 | 99 |
Adapted from AUA, 2014.21
Does Stone location affect rates of passage?
| Stone Location | % Spontaneous passage rate |
| proximal ureter | 48 |
| mid-ureter | 60 |
| distal ureter | 75 |
| ureterovesical junction | 79 |
Adapted from Coll et al., 2002.12
- Most stones that pass spontaneously pass within 1 month of symptom onset.21
- Who can be discharged home without urology consult?
- small stones, symptoms resolved, no evidence of infection 25
- Discharge Instructions 24,25
- Rx for NSAIDs or opioids or combination therapy +/- MET therapy
- Instructions to return for fever, vomiting, worsening pain, decreased urine output, nausea, and/or chills
- If stone has not passed, provide patient with strainer to collect stone for outpatient analysis
- Urology follow-up
Renal Injury in the Setting of Nephrolithiasis
Nephrolithiasis is not always a benign process and it’s important for the physician to identify which stones require urgent or emergent attention in order to optimize patient care. A literature review by Tang et al. noted that nephrolithiasis plays a role in causing kidney damage by mechanisms, which include 22
- post-obstructive acute kidney injury
- direct cellular toxicity
- chronic kidney disease (CKD) and end-stage renal disease (ESRD)
Post-obstructive AKI: increased risk for patients with larger stones, bilateral ureteral stones, those with pre-existing kidney disease, and those with a solitary kidney. Although this study suggests the incidence of post-obstructive AKI is rare (1-2%)22, it is important to think about your patient population and think about how many of them have underlying risk factors.
Direct Cellular Toxicity: studies have demonstrated that interaction of calcium oxalate with epithelial cells of the kidney results in mitochondrial dysfunction, release of oxygen free radicals, and subsequently cell death.22
CKD/ESRD: this review also suggests that nephrolithiasis as an independent risk factor for CKD and ESRD.22 A similar study which compared 21,474 patients with newly diagnosed CKD to matched controls showed that that CKD patients were almost 2 times more likely to have a prior diagnosis of urolithiasis.23
What Is the Utility of Ultrasound?
CT is a widely accepted diagnostic modality for nephrolithiasis; however, due to risk of radiation, other modalities such as bedside ultrasound have been investigated. A recent study compared point of care ultrasound (POCUS) to radiology-performed ultrasound and CT scan and concluded that ultrasound is a good initial diagnostic test for nephrolithiasis.16 Ultrasound is associated with less radiation exposure with no difference in 30-day incidence of high risk diagnosis and diagnostic accuracy when compared with CT scan.16 Sensitivities of POCUS, radiology-performed ultrasound and CT were 54%, 57%, and 88% respectively. This data shows that ultrasound is NOT as sensitive as CT scan for the detection of stones. Although ultrasound is poor at detecting stones, research shows that ultrasound is both specific and sensitive for detecting hydronephrosis 14 which can help clinicians quickly stratify their patients and expedite management decisions.20 The drawback with ultrasound is that diagnostic accuracy greatly depends on practitioner experience.2 In addition, it may not identify other potential abdominal pathology that CT scan is utilized to identify. Herbst et al recently demonstrated that point of care ultrasound is sensitive for the detection of hydronephrosis, but fellowship trained physicians were better at detecting hydronephrosis on ultrasound when compared to non-fellowship trained physicians.2
So what if my patient has hydronephrosis?
Hydronephrosis indicates obstruction which is a threat to renal blood flow. A young healthy patient without any signs of renal impairment or infection can be discharged home with urology follow-up within 1 week. Patients that do not meet the above criteria will benefit from urology consult in the Emergency Department.
Provider’s Quick Guide to performing bedside renal ultrasound20
- probe selection: 2-5MHz probe is best; can use higher frequency probes in thin patients; but remember that higher frequency means less penetration
- position of patient: supine
- a complete exam includes 6 views:
- transverse and longitudinal view of right kidney
- transverse and longitudinal view of left kidney
- transverse and longitudinal view of bladder
- Start with longitudinal view of a kidney, and once located, rotate 90 degrees to get transverse view. Save multiple still images in each orientation.
- Left kidney is more cephalad and posterior than the right kidney and can likely be viewed in posterior axillary line and in lateral decubitus position
- Bladder view: place probe in suprapubic area; remember to get 2 views
- bladder volume can be estimated with formula 0.75 x width x length x height
- some machines can automatically calculate this value for you as well.
- Do not misdiagnose the pyramids as hydronephrosis: pyramids are located just below cortex and are not connected to each other whereas the collecting system is in the center and should be hyperechoic in the absence of hydronephrosis
- Do not misdiagnose renal cysts as hydronephrosis: renal cysts are usually not located in renal pelvis which is in the center; they are usually peripheral
- Common causes of false positives: pregnancy causes non-pathological hydronephrosis due to ureteral compression
- Common cause of false negatives: severe dehydration can cause a false negative scan
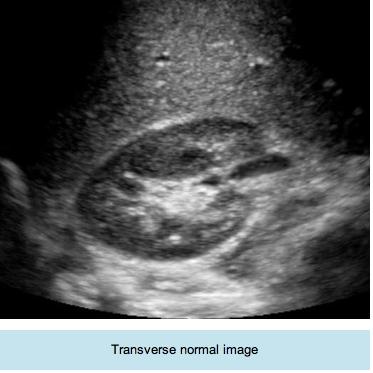
(notice the anechoic renal pyramids in periphery)
Image courtesy ultrasoundpaedia.com/normal-kidney
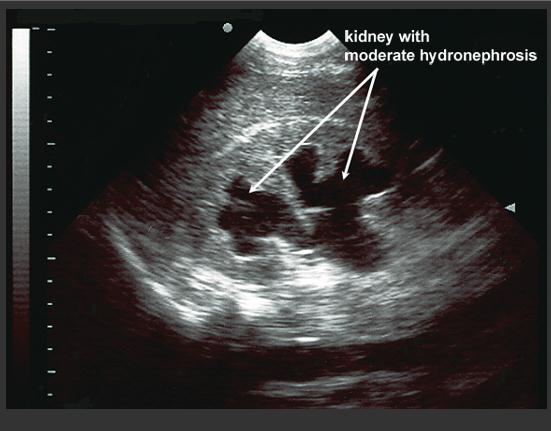
Image courtesy of Dr. Hoffmann, http://www.sonoguide.com/renal.html
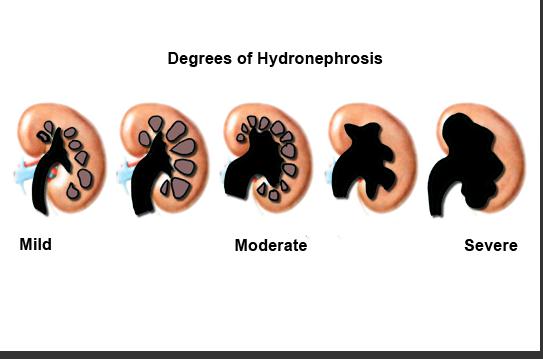
Image courtesy of Dr. Hoffmann, http://www.sonoguide.com/renal.html
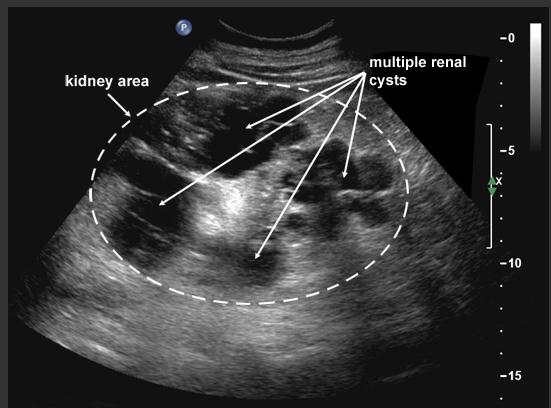
Image courtesy of Dr. Hoffmann, http://www.sonoguide.com/renal.html
References // Further Reading
- Curhan G, Aronson M, Preminger G. Diagnosis and acute management of suspected nephrolithiasis in adults. Available at : www.uptodate.com/contents/diagnosis-and-acute-management-of-suspected-nephrolithiasis-in-adults. Last accessed: October 21, 2014
- Herbst M, Rosenberg G, Daniels B et al. Effect of Provider Experience on Clinician-Performed Ultrasonography for Hydronephrosis in Patients With Suspected Renal Colic. Annals of emergency medicine. 2014;64(3):269-76. doi:10.1016/j.annemergmed.2014.01.012.
- Carnell J, Fischer J, Nagdev A. Ultrasound detection of obstructive pyelonephritis due to urolithiasis in the ED. The American Journal of Emergency Medicine. 2011;29(7):843.e1-843.e3. doi:10.1016/j.ajem.2010.07.006.
- Kalra O. Approach to a patient with urosepsis. Journal of Global Infectious Diseases. 2009;1(1):57-63. doi:10.4103/0974-777x.52984.
- Koroglu M, Wendel J, Ernst R, Oto A. Alternative diagnoses to stone disease on unenhanced CT to investigate acute flank pain. Emergency radiology. 2004;10(6):327–333.
- Soleimanpour H, Hassanzadeh K, Vaezi H, EJ Golzari S, Esfanjani R, Soleimanpour M. Effectiveness of intravenous lidocaine versus intravenous morphine for patients with renal colic in the emergency department. BMC Urol. 2012;12(1):13. doi:10.1186/1471-2490-12-13.
- Golzari S, Soleimanpour H, Rahmani F et al. Therapeutic Approaches for Renal Colic in the Emergency Department: A Review Article. Anesthesiology and Pain Medicine. 2014;4(1):e16222. doi:10.5812/aapm.16222.
- Lisander B. Evaluation of the analgesic effect of metoclopramide after opioid-free analgesia. British journal of anaesthesia. 1993;70(6):631–633.
- Lu Z, Dong Z, Ding H, Wang H, Ma B, Wang Z. Tamsulosin for Ureteral Stones: A Systematic Review and Meta-Analysis of a Randomized Controlled Trial. Urologia Internationalis. 2012;89(1):107-115. doi:10.1159/000338909.
- Vincendeau S, Bellissant E, Houlgatte A et al. Tamsulosin hydrochloride vs placebo for management of distal ureteral stones: a multicenter, randomized, double-blind trial. Archives of internal medicine. 2010;170(22):2021–2027.
- Singh A, Alter H, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Annals of emergency medicine. 2007;50(5):552–563.
- Coll D, Varanelli M, Smith R. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. American Journal of Roentgenology. 2002;178(1):101–103.
- Turk C, Knoll T, Petrik A, Sarica K, Straub M, Seitz C. Guidelines on Urolithiasis. European Association of Urology. 2014. Available at: http://www.uroweb.org/guidelines/online-guidelines. Accessed October 31, 2014.
- Rosen C, Brown D, Sagarin M, Chang Y, McCabe C, Wolfe R. Ultrasonography by emergency physicians in patients with suspected ureteral colic. The Journal of emergency medicine. 1998;16(6):865–870.
- M”uller T, Naesh O, Svare E, Jensen A, Glyngdal P. Metoclopramide (Primperantextregistered) in the Treatment of Ureterolithiasis. Urologia internationalis. 1990;45(2):112–113.
- Smith-Bindman R, Aubin C, Bailitz J et al. Ultrasonography versus Computed Tomography for Suspected Nephrolithiasis. New England Journal of Medicine. 2014;371(12):1100-1110. doi:10.1056/nejmoa1404446.
- Westphalen A, Hsia R, Maselli J, Wang R, Gonzales R. Radiological Imaging of Patients With Suspected Urinary Tract Stones: National Trends, Diagnoses, and Predictors. Academic Emergency Medicine. 2011;18(7):699-707. doi:10.1111/j.1553-2712.2011.01103.x.
- Pearle M, Goldfarb D, Assimos D et al. Medical Management of Kidney Stones: AUA Guideline. The Journal of Urology. 2014;192(2):316-324. doi:10.1016/j.juro.2014.05.006.
- Hoffmann B, Blok B. Renal Ultrasound. Sonoguidecom. 2014. Available at: http://www.sonoguide.com/renal.html. Accessed October 31, 2014.
- Noble V, Nelson B. Manual Of Emergency And Critical Care Ultrasound. 2nd ed. Cambridge: Cambridge University Press; 2011:133-146.
- org. Kidney Stones: American Urological Association. 2014. Available at: http://www.auanet.org/education/kidney-stones.cfm. Accessed October 31, 2014.
- Tang X, Lieske J. Acute and chronic kidney injury in nephrolithiasis. Current Opinion in Nephrology and Hypertension. 2014;23(4):385-390. doi:10.1097/01.mnh.0000447017.28852.52.
- Keller J, Chen Y, Lin H. Association between chronic kidney disease and urinary calculus by stone location: a population-based study. BJU International. 2012;110(11c):E1074-E1078. doi:10.1111/j.1464-410x.2012.11380.x.
- Baun K, Easter J. Marx: Rosen’s Emergency Medicine-Concepts And Clinical Practice. 8th ed. Elsevier Health Sciences; 2013:1336-1342.
- Manthey DE, Nicks BA. Chapter 97. Urologic Stone Disease. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill
- http://www.ncbi.nlm.nih.gov/pubmed/23850311
- http://www.ncbi.nlm.nih.gov/pubmed/22685250
- http://www.ncbi.nlm.nih.gov/pubmed/24440589
- http://www.ncbi.nlm.nih.gov/pubmed/22981138
- http://www.ncbi.nlm.nih.gov/pubmed/23528508





2 thoughts on “Nephrolithiasis: Diagnosis and Management in the ED”
Pingback: emDOCs.net – Emergency Medicine EducationPain Profiles: Intravenous Lidocaine for Intractable Renal Colic Unresponsive to Standard Therapy - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationPain Profiles: Ketorolac and Morphine in Renal Colic - emDOCs.net - Emergency Medicine Education