
Author: Ben Shepherd, MBBS FACEM DRANZCOG (Adv) (@OBCast, Emergency Physician Wollongong & Shoalhaven Hospitals NSW Australia) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); and Manpreet Singh, MD (@MprizzleER)

emDocs is proud to host posts from Ben Shepherd, creater of OBCast. From Ben: “During my emergency medicine specialist training I spent time training towards and working as a rural GP obstetrician. It remains some of the most enjoyable and rewarding time I have spent in medicine. Coming back to emergency medicine it is obvious that my colleagues are often uncomfortable managing pregnancy-related problems, particularly those in the latter stages. The goal of ‘OBcast’ is to provide clear and practical information for ‘the reluctant obstetrician’ (emergency physician, rural GP) and improve confidence and the quality of care these families receive during what is both a stressful and wonderful time of their lives.”
This post evaluates ectopic pregnancy. Each post will contain a video presentation and downloadable slides for learning on the go.
PDF: https://obcast.net/wp-content/uploads/2019/01/Ectopic-Pregnancy.pdf
We have all heard the words: “Every woman of child-bearing age has an ectopic pregnancy until proven otherwise”. This is the classic emergency medicine example of a condition for which we have developed a high index of suspicion. It is still a potential cause of maternal mortality but thankfully one we are generally managing well. It is defined as an extrauterine pregnancy, and although most are tubal, other locations can and do occur.

- 1-2% of pregnancies are extrauterine
- Incidence is rising
- Vast majority are tubal, 2-5% are outside tube
- Increased in IVF
- But becoming similar to spontaneous pregnancy
- Heterotropic pregnancy = IUP + Ectopic
- General incidence~1:4000
- Higher in assisted fertility
Risk Factors for Ectopic Pregnancy
- Risk factors with OR>4.0
- Prior tubal surgery
- Prior ectopic pregnancy
- Sterilization
- Use of IUD
- Risk factors with OR>2.0
- Current or ascending infection
- Cigarette smoking
- >1 sexual partner
- Tubal pathology

Patient Assessment
- History
- General and Obstetric History
- Pain, bleeding, prior episodes, complications in pregnancy, prior pregnancies, history of IVF
- Exploration of symptoms / risk factors
- Consideration of differential diagnosis
- Exam
- Haemodynamic status
- Localized abdominal findings / peritonitis
- Role of pelvic and speculum exam controversial
- PoCUS – Imaging modality of choice! Ask the following:
- Free fluid?
- IUP present?
- Viability?
- Labs
- Bloods: Hb, Group & Hold, BhCG
Ultrasound Findings
- 88% of ectopic pregnancies are identifiable by:
- No IUP
- Adnexal mass
- Diagnosis confirmed if: yolk sac, fetus seen in ectopic tissue
- Rupture can be suspected if:
- Free fluid Pouch of Douglas
- Free fluid in Morrisons pouch
- Operative therapy needed
Management – Unstable
- Resuscitation: Fluid resuscitation, Early O Neg +/- MTP
- Supportive Care: Analgesia
- Specific Care: Operative therapy for Salpingectomy
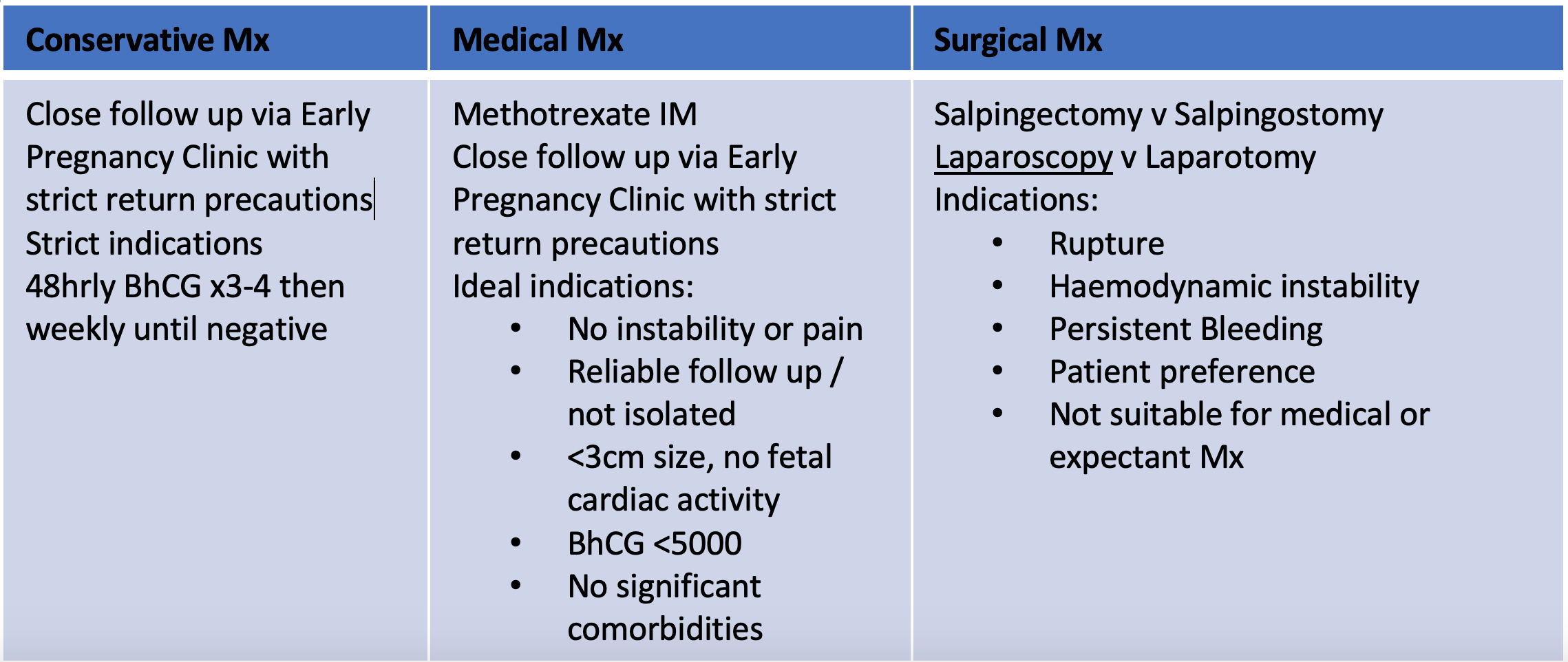
Management – Stable
From Dr. Katelyn Hanson and Hanson’s Anatomy:

More #FOAMed:
- Core EM
- Emergency Medicine Cases Best Case Ever
- emDocs EM@3AM
- emDocs
- emDocs US Probe
- Emergency Medicine Cases Rapid Review Videos
- EM Updates – Ectopic Rule Out
- Life in the Fast Lane
- REBEL EM – MTX Failure






1 thought on “OBCast: Ectopic Pregnancy”
Pingback: Ektopisk / Extrauterin graviditet – Mind palace of an ER doc