Author: Richard Slama, MD (EM Resident Physician, Naval Medical Center Portsmouth) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
Introduction/Case Presentation
A 17 month-old adopted male with no major medical history presents for evaluation of inconsolability and refusal to use his right arm. Mother states that this had been going on for approximately one day and is not associated with any fevers, vomiting, diarrhea, or URI type symptoms. He has no major medical/surgical history, no allergies, and does not take any medications. Vital signs on arrival are within normal limits for his age range, and his physical exam including neurologic were within normal limits with the exception of refusal to use his right arm.
Because of his symptoms he is diagnosed with a nursemaid’s elbow, reduced at bedside with a palpable clunk, and later discharged with return precautions and follow up with PCM. Unfortunately the child presented later that evening with complete right upper extremity hemiplegia, right facial droop, and excessive drooling. He was then sent for an MRI which revealed a large MCA stroke.
The above case is not uncommon for pediatric stroke, as they are very often atypical presentations initially. This is especially true of the very young, and just as in adults, this disease can have devastating and potentially lifelong consequences. So the question now becomes how should we as Emergency Physicians be diagnosing and treating this condition?
Epidemiology
- 9/100,000 will have a stroke1
- This occurs in males more than females
- African Americans are among the highest risk patients (Sickle Cell)
Causes
Though the risks of adult stroke can usually be predicted based on a defined set of long term risk factors, most pediatric strokes are from some type of congenital anomaly or inborn error of metabolism. For simplicity, the risk factors for pediatric stroke can be broken down into four main categories.2
- Cardioembolic
- Patent foramen ovale, ASD, other Congenital Heart Disease
- Hematologic
- Sickle Cell (the most common cause overall), Anemia (particularly iron deficiency), Antiphospholipid syndrome, Abnormal activated protein C resistance (usually related to the Factor V Leiden mutation), Protein C deficiency, Protein S deficiency, etc.
- Vasculopathic
- Traumatic Carotid dissection, fibromuscular dysplasia, Ehlers-Danlos, Marfan, Osteogenesis Imperfecta, etc.
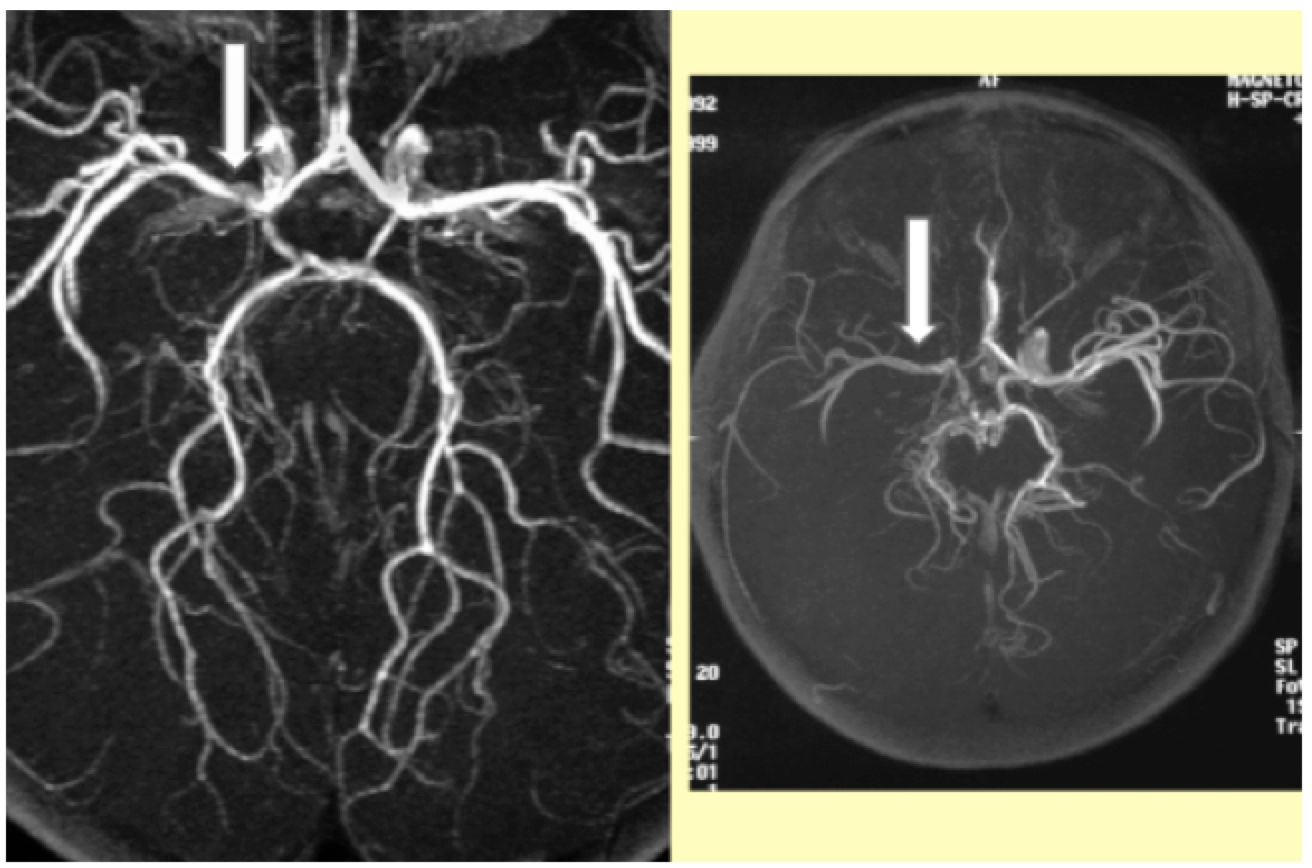
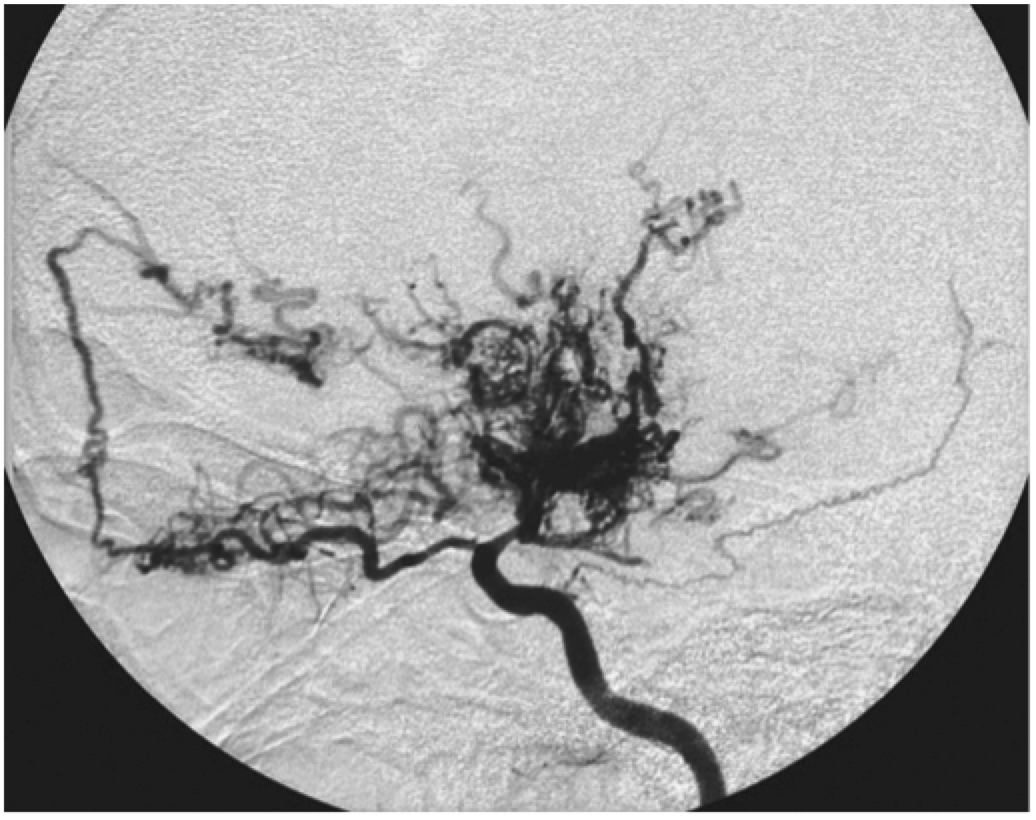
- Moyamoya – syndrome that causes progressive stenosis of the carotid arteries with formation of collateral vessels (puff of smoke appearance on CT, shown below)4
- Occurs mainly in Asian populations and may have a genetic basis
- Recurrent TIA and strokes from a young age
 4. Metabolic – all the weird ones that no one will diagnose in the ED
4. Metabolic – all the weird ones that no one will diagnose in the ED
- Methylmalonic academia, Propionic academia, Isovaleric academia, Glutaric aciduria types 1, Fabry Disease
Presentation
The presentation of stroke can be an exceedingly difficult diagnosis to make in children mostly because of non-classical presentation and limited ability to conduct full neurological examination. Typically older children will present with symptoms that are more along the same spectrum as adults with weakness, cranial nerve deficits, sensory deficits, etc. Young children and infants can have a very broad spectrum of presentations that may present with focal neurological deficits, but are much more likely to present with altered mental status and/or seizures.5,6 This is yet another example of how young children’s disease processes can differ vastly from the adult population.
Diagnosis
While the ED workup of children is fairly similar to adults, there are some major differences that apply to this population. The first major difference is that any child with a suspected stroke should receive an MRI instead of a CT when available.7 The reasoning for this is twofold: First, MRI is more reliable in children than adults, and second, radiation exposure is avoided using this technique. All basic labs should be ordered including CBC, BMP, PT/INR, PTT. Adjunct studies that may be useful include Echo, EEG, Tox Screen, and lumbar puncture.
Treatment
Yet again there is another major difference between adults and children. There is no indication for TPA usage in children at this point in time. The reason being is that there have been no successfully randomized control trials to prove this intervention works. There was a study in 2010 called the Thrombolysis in Pediatric Stroke Study (TIPS), which was aimed at determining the efficacy of tPA in children. Unfortunately the study’s funding was pulled by the NIH for a lack of enrollment. There were 17 sites involved. In a two year period only 93 children ended up being enrolled, and approximately 50% of these children did not have a stroke. Of the 50% that did have a stroke, only one child met inclusion criteria for tPA and even this child did not receive it.8 The inclusion/exclusion criteria for the study was quite complex, and it would be exceedingly difficult to design a study that would be able to safely enroll enough children.
So the question then becomes “well why can’t I just dose a child as if they were an adult”? The answer is that this dosing scheme would likely be ineffective in children because they metabolize and clear TPA much faster than adults, and this dose would likely be ineffective. The bottom line is that there is no indication for TPA in children unless your institution is enrolled in a select research protocol or you have a pediatric neurologist with experience in giving TPA.
Next is the question of blood thinners and antiplatelet therapy. Again there is very limited evidence to support any of these treatments, and these should only be provided after talking to a neurologist. The AHA does have some recommendations based on the current litereature.9 Again most of these are not going to be started in the ED.
- Ischemic stroke unknown cause: ASA 3-5 mg/kg
- Dissection, cardioembolic, hypercoagulable state: Heparin
- Sickle Cell Disease: Hydration, exchange transfusion
Disposition and Prognosis
Any child, regardless of cause, will obviously be admitted to the hospital, and the treatment course will vary based on the primary team and stroke etiology. Most treatment will be supportive with aggressive physical therapy when the child can tolerate it. If there are reversible causes (antiphospholipid, SCD, etc.) these should be corrected, but this will not likely be a goal of emergency department care. Unfortunately 50% of children experiencing a stroke of any type will have severe neurologic deficits despite interventions.
Summary
Pediatric stroke is a rare, but serious condition that many ED physicians will see at some point in their career. Boys are at a higher risk than girls, and African Americans are at the highest risk of any race due to prevalence of sickle cell disease. There are four main risk categories for pediatric stroke including cardioembolic, hematologic, vasculopathic, and metabolic. Children present atypically, and therefore a high index of suspicion is needed for diagnosis. Finally, there are no randomized controlled trials that have established the efficacy of tPA. Unfortunately, most children will have long-term neurologic deficits despite treatment. Future research is needed to establish better treatment protocols for pediatric stroke.
References / Further Reading
- Giroud M, Lemesle M, Gouyon JB, Nivelon JL, Milan C, Dumas R. Cerebrovascular disease in children under 16 years of age in the city of Dijon, France: a study of incidence and clinical features from 1985 to 1993. J Clin Epidemiol. 1995;48(11):1343-1348. doi:10.1016/0895-4356(95)00039-9.
- Sträter R, Becker S, von Eckardstein A, et al. Prospective assessment of risk factors for recurrent stroke during childhood–a 5-year follow-up study. Lancet. 2002;360(9345):1540-1545. doi:10.1016/S0140-6736(02)11520-0.
- Amlie-Lefond C, Bernard TJ, Sebire G, et al. Predictors of cerebral arteriopathy in children with arterial ischemic stroke;Results of the international pediatric stroke study. Circulation. 2009;119(10):1417-1423. doi:10.1161/CIRCULATIONAHA.108.806307.
- Desk R, Williams L, Health WK. Comments , Opinions and Reviews Moyamoya Disease — A Review. 1983:104-109. doi:10.1161/01.STR.14.1.104.
- DeVeber G. Arterial Ischemic Strokes in Infants and Children: An Overview of Current Approaches. Semin Thromb Hemost. 2003;29(6):567-573. doi:10.1055/s-2004-815624.
- Chadehumbe M a, Khatri P, Khoury JC, et al. NIH Public Access. 2010;24(1):9-12. doi:10.1177/0883073808320756.Seizures.
- Shellhaas R a, Smith SE, O’Tool E, Licht DJ, Ichord RN. Mimics of childhood stroke: characteristics of a prospective cohort. Pediatrics. 2006;118(2):704-709. doi:10.1542/peds.2005-2676.
- Rivkin MJ, deVeber G, Ichord RN, et al. Thrombolysis in Pediatric Stroke Study. Stroke. 2015:880-885. doi:10.1161/STROKEAHA.114.008210.
- Roach ES, Golomb MR, Adams R, et al. Management of stroke in infants and children: A scientific statement from a special writing group of the american heart association stroke council and the council on cardiovascular disease in the young. Stroke. 2008;39(9):2644-2691. doi:10.1161/STROKEAHA.108.189696.
- http://www.ncbi.nlm.nih.gov/pubmed/22974650
- http://www.ncbi.nlm.nih.gov/pubmed/22254140





4 thoughts on “Pediatric Stroke: EM-focused highlights”
Pingback: PEM Review 013 – CANNULATION // ANAPHYLAXIS // FEBRILE CONVULSIONS // COMMUNICATION // ENT | PEMgeek.com – #FOAMed Highlights from the world of Paediatric Emergency Medicine
Pingback: Global Intensive Care | AIR Series: Neurology Module 1 – Bleeds and Strokes