General Info/Intro/Main Question(s)
Syncope is a sudden transient loss of consciousness and postural tone followed by complete spontaneous recovery caused by acute hypoperfusion of either both cerebral hemispheres or the brainstem (RAS). The key to the ED evaluation of pediatric syncope is using the history, physical, and ECG to exclude serious pathology.
Recap Basics
Three Major Categories:
- Neurocardiogenic (most common)
- Cardiovascular-mediated
- Non-cardiovascular
History: 6 P’s
- prodrome activities
- prodrome sx
- predisposing factors
- precipitating factors
- passerby witness
- post-ictal phase
Red Flags
- history of congenital heart disease
- lack of prodromal symptoms
- syncope while supine
- syncope during exertion
- FH of sudden death, long QT, sensorineural hearing loss
- pathologic murmur
- chest pain
Physical
- cardiac auscultation supine and standing
- orthostatic vitals
- neuro
- physical features associated w cardiac or neuro disease (eg Marfan habitus, café-au-lait spots, wooly hair)
Diagnostic Evaluation
- ECG
- Urine hcg for menstruating females
Cardiovascular Differential
- Long QT (>450ms)
- QTc = QT/sqrt(R-R) measure beginning of QRS to end of T wave in leads II, V5
- associated congenital syndromes: Romano-Ward and Jervell-Nielsen-Lange (assoc w FH of deafness)
- medications: tricyclic antidepressants, antipsychotics, antibiotics (macrolides), organophosphates, antihistamines, antifungals
- Brugada: ST elevation in V1 and V2
- Heart block
- SVT: HR >220 in infants and children, >180 in older children and adolescents
- WPW: delta wave, shortened PR, widened QRS
- Commotio cordis: dysrhythmia due to direct blow to the chest
- HOCM
- Anomalous left coronary artery from the pulmonary artery (ALCAPA)
- Looks like anterolateral MI
- Q waves and ST changes in I, aVL, V5, V6 (figure 2)
- Abnormal R wave progression in chest leads
- Arrhythmogenic right ventricular dysplasia (ARVD)
- usually exercise-related
- 90% have abnormal ECG
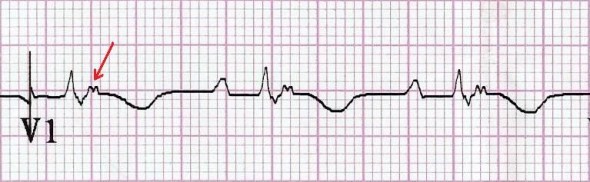
- Epsilon wave (figure 3), T wave inversion V1-3, +QRS in V1
Additional causes to consider
- PE
- Breath-holding spell: 6-18 months
- Seizure
- Psychiatric, hyperventilation, conversion
- Vertebrobasilar migraine
- Tussive syncope
- Drugs/toxins: eg. CO poisoning
Bottom Line/Pearls & Pitfalls
- ECG abnormalities should be discussed with a pediatric cardiologist if possible prior to admission
- T waves in V1 and V3R invert during the first week of life and remain inverted until adolescence
- T waves in V2-3 are inverted in childhood and become upright by age 8-12
- T waves in V5-6 should be upright after the first 3 days of life
- Neurocardiogenic syncope does not occur while supine
- Infant ECG: axis is rightward, QRS and PR are shorter, and QTc longer. These gradually change with age.
- Keep CO poisoning in your differential
Figures
Figure 1: HOCM
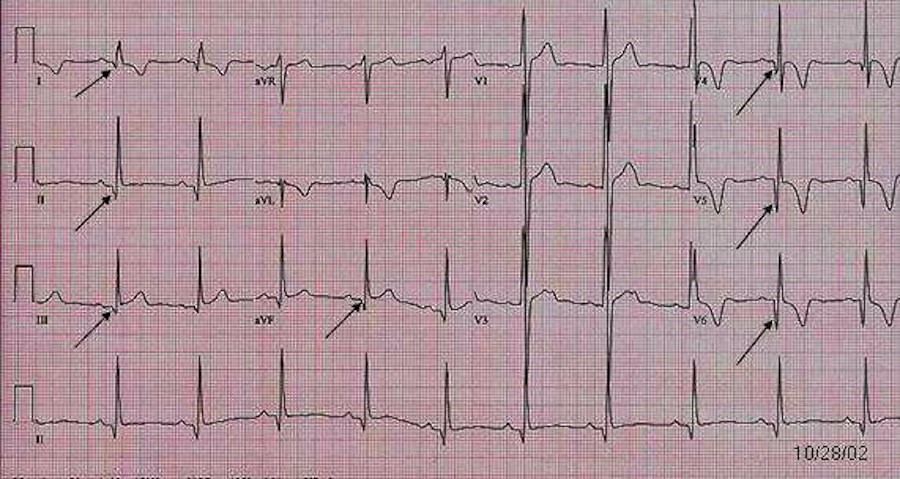
Figure 2: ALCAPA
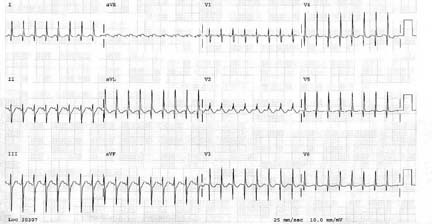
Figure 3: epsilon wave seen in ARVD
Further Reading / References
- Fischer J, Cho C. Pediatric Syncope: Cases from the emergency department. Emerg Med Clinics of North America. 28 (2010) 501-516
- Goble M, et al. ED management of pediatric syncope: searching for a rationale. The Am Journal of Emergency Med (2008) 26, 66-70
- Steinberg L.A., Knilans T.K., Syncope in children: diagnostic tests have a high cost and low yield. J Pediatr, 146 (2005), pp 255-258
- Wathen JE, et al. Accuracy of ECG interpretation in the pediatric emergency department. Ann Emerg Med, 46 (2005), pp 507-511
- Ritter S, Tani LY, Etheridge SP, et al. What is the yield of screening echocardiography in pediatric syncope? Pediatrics 2000; 105(5):E58.
- Massin M, et al. Syncope in pediatric patients presenting to an emergency department. The Journal of Pediatrics. 2004 Vol 145(2); 223-228
- Moodley M. Clinical approach to syncope in children. Seminars in pediatric neurology. 2013 20:12-17.
- Dickinson D. The normal ECG in childhood. Heart. Dec 2005; 91(12): 1626–1630.
- Chan T, Sharieff GQ, Brady W. Electrocardiographic manifestations: pediatric ECG. The Journ of Emerg Med, 2008, Vol. 35, No. 4, pp 421-430
- Rosen’s Emergency Medicine 8th ed
- http://www.ncbi.nlm.nih.gov/pubmed/9814401
- http://www.ncbi.nlm.nih.gov/pubmed/22406025





1 thought on “Pediatric Syncope”
Pingback: emDOCs.net – Emergency Medicine EducationEM in 5: Pediatric EKG - emDOCs.net - Emergency Medicine Education