
Authors: Diana Halloran, MD (EM Resident Physician, Northwestern University, @Diana_Halloran) and Matthew R Klein, MD, MPH (Assistant Program Director, Attending Physician, Northwestern University, @MKleinMD) // Reviewed by: Stephen Alerhand, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Introduction
This post will focus on four common emergency department presentations for which pelvic ultrasound can help promptly identify “can’t miss” diagnoses.
Case 1: The patient is a 32-year-old female presenting with one day of lower abdominal pain and vaginal bleeding. Her last menstrual period was nine weeks ago and she has not yet established care with an obstetrician.
Case 2: The patient is a 23-year-old female with severe left lower abdominal pain associated with nausea and vomiting. She is tender in the left adnexal area on bimanual exam, and you feel a possible mass. Her serum hcg is negative.
Indications
For Case #1 the differential diagnosis includes: vaginal bleeding in early pregnancy, pregnancy loss, and ectopic pregnancy. The “can’t miss” diagnosis in this scenario is an ectopic pregnancy.
For Case #2 the differential diagnosis includes: pelvic inflammatory disease, tubo-ovarian abscess, hemorrhagic cyst, or ovarian torsion. The “can’t miss” diagnosis in this scenario is ovarian torsion.
In all of these cases pelvic ultrasound can aid in the rapid diagnosis of these diagnoses.
Background
Pelvic ultrasounds comprise both point of care ultrasound (POCUS) and formal radiologic ultrasounds. POCUS has a long history in emergency medicine, dating back to The American College of Emergency Medicine’s (ACEP) first position paper on the subject in 1990 (1). POCUS is low risk and can streamline patient visits by reducing length of stay (2). Pelvic ultrasounds assessing for intrauterine pregnancy performed by emergency physicians have been shown to reduce the need for secondary consultative imaging (3). In addition, POCUS use has been shown to save healthcare costs even when POCUS encounters did not change the management of the patient (4). However, POCUS is only indicated in specific instances for pelvic ultrasound – generally early pregnancy evaluation, or ectopic rule out. If the patient presentation is not this specific circumstance, then a formal ultrasound needs to be obtained.
Ectopic Rule Out
In the first case we have identified ectopic pregnancy as the “can’t miss” diagnosis. The true goal of an “ectopic rule out” is actually to “rule in” an intrauterine pregnancy (IUP), if possible. To do this we need two criteria: 1) an hCG level at or above the discriminatory zone, and 2) visualization of certain structures. First is the hCG. In general, an IUP should be visible on transvaginal ultrasound if the hCG is above the discriminatory zone, or >1,500-2000 (5). The second is that to fully diagnose an IUP multiple structures need to be identified, including the gestational sac, yolk sac, and fetal pole.
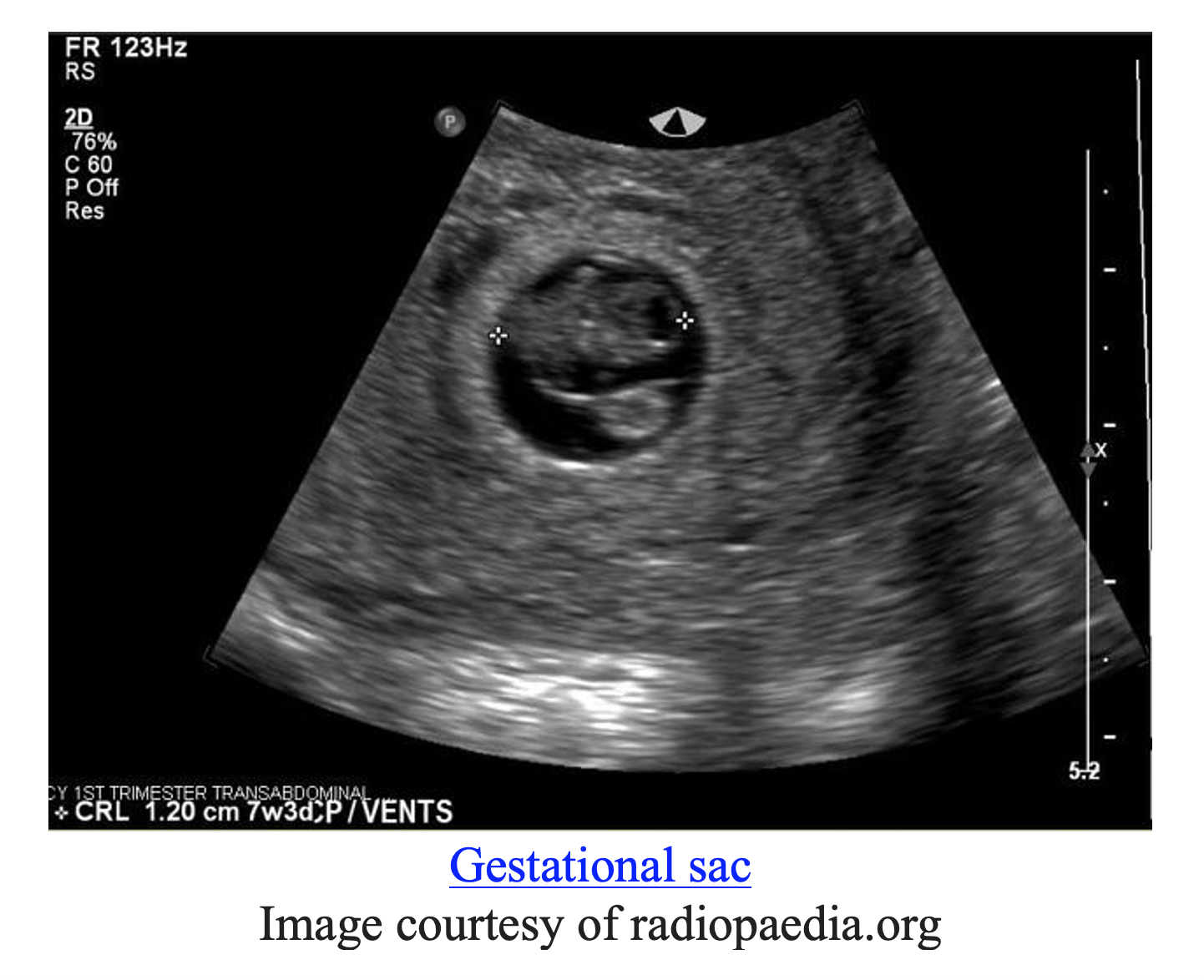
The gestational sac is an intrauterine fluid collection that can be seen on transvaginal ultrasound (TVUS). It is the first sign of early pregnancy on ultrasound and is seen at 5 weeks gestational age. To be a true gestational sac it must be found to be next to the endometrium (6).
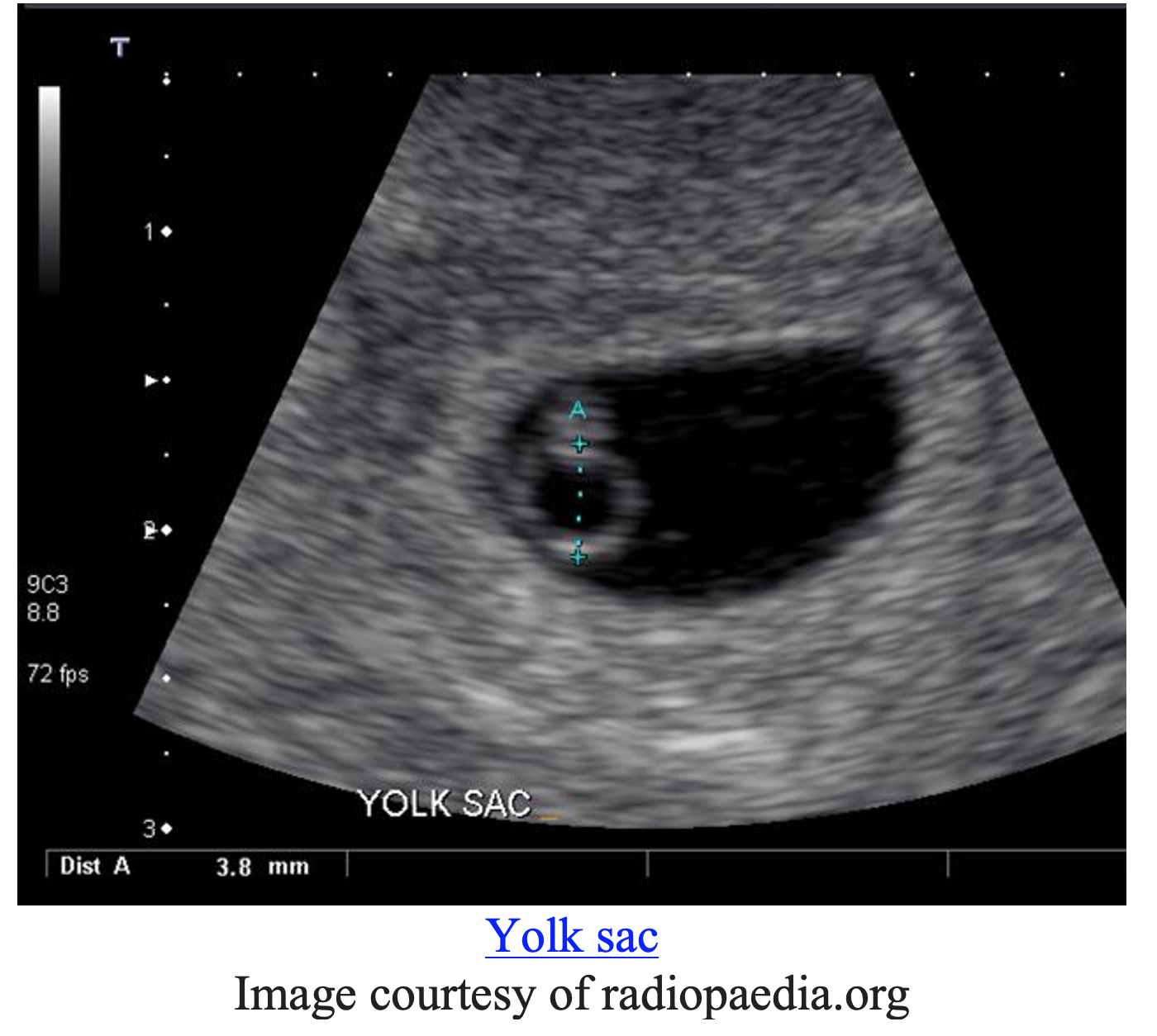
The yolk sac can be seen at about 5 ½ weeks of gestation. It will be seen inside the gestational sac. The presence of the yolk sac inside of the gestational sac does not confirm viability but it does confirm an intrauterine pregnancy (6).

The fetal pole will be seen adjacent to the yolk sac. A fetal pole next to the yolk sac within the gestational sac confirms an intrauterine pregnancy. It appears around 6 weeks of gestational age (6).
Video courtesy of Dr. Victor Bang and The Point of Care Ultrasound Atlas
In comparison to the images above, if no IUP is confirmed and no ectopic is seen then the patient is diagnosed with pregnancy of unknown location. These patients should follow up closely with an OBGYN within 48 hours to have a repeat ultrasound. Free fluid in Morrison’s pouch (a positive FAST) in the setting of a positive pregnancy with a pregnancy of unknown location have been shown to predict the need for operative intervention (7). A FAST exam should be performed in any patient with a suspected ectopic pregnancy.
Ruptured ectopic with positive FAST
Video courtesy of Dr. Stacey Frisch and The Point of Care Ultrasound Atlas
POCUS performed by emergency physicians demonstrates favorable test characteristics when evaluating for ectopic pregnancy: 99% sensitivity and a 99.9% negative predictive (2). As the incidence of heterotopic pregnancy outside of fertility treatments is extremely low, ectopic pregnancy can be ruled out with a negative predictive value of essentially 100% when a normal IUP is visualized (2). Research has also shown that POCUS TVUS to evaluate for an ectopic pregnancy has reduced the incidence of discharged patients returning with a ruptured ectopic pregnancy (8).
Ovarian Torsion
For case #2 – a women with severe left adnexal pain and associated nausea and vomiting – the “can’t miss” diagnosis is ovarian torsion. Evaluation for ovarian torsion requires evaluation with formal ultrasound. Features on ultrasound most predictive for a possible ovarian torsion include abnormal blood flow and presence of free fluid (9).
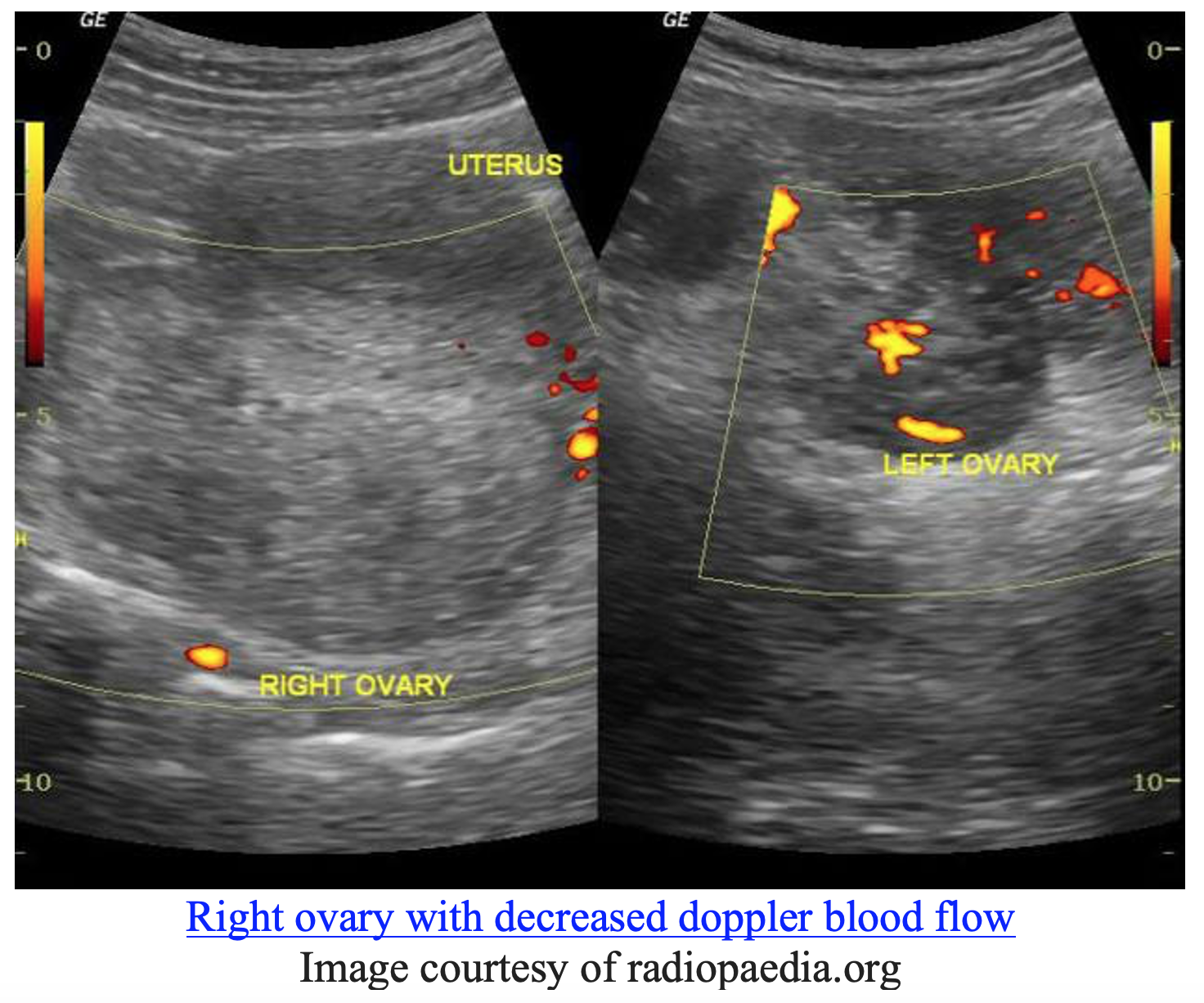
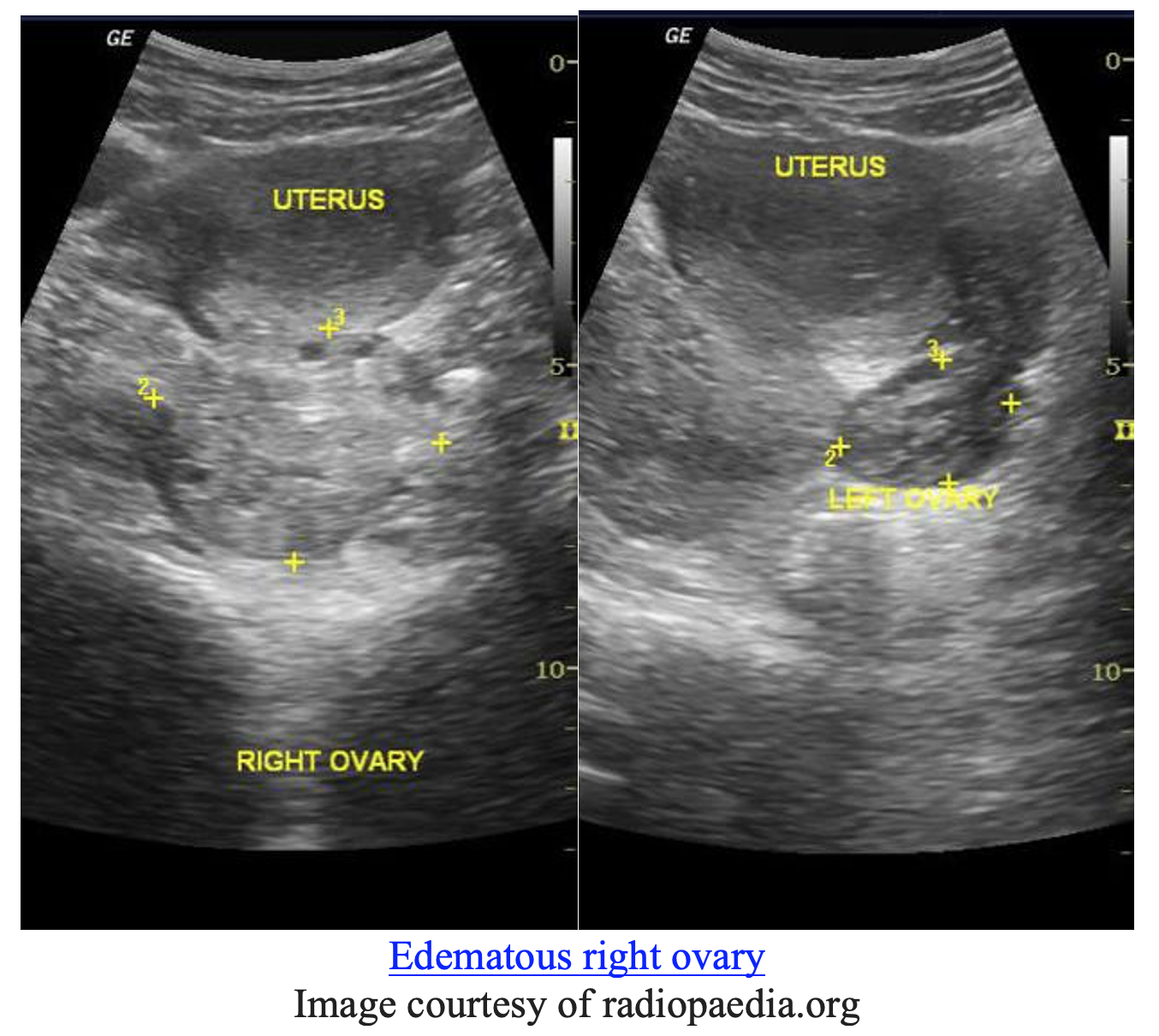
However, the presentation of ovarian torsion can be highly variable. When considering the diagnosis of ovarian torsion, emergency clinicians should remember that patients may present without a palpable adnexal mass, the location and description of the pain can mimic other disorders such as appendicitis and nephrolithiasis, and normal doppler blood flow does not rule out ovarian torsion (10).
Hemorrhagic Cyst
Ovarian torsion is not the only diagnosis to consider in a patient with pelvic pain and an adnexal mass. The classic presentation for a hemorrhagic cyst is sudden onset pelvic pain often resulting after sexual intercourse. However, in any case of pelvic pain, emergency clinicians must always maintain a high index of suspicion for ectopic pregnancy and ovarian torsion. A negative hCG would rule out ectopic pregnancy, and a pelvic ultrasound can be used to evaluate both for ovarian torsion and a hemorrhagic cyst.
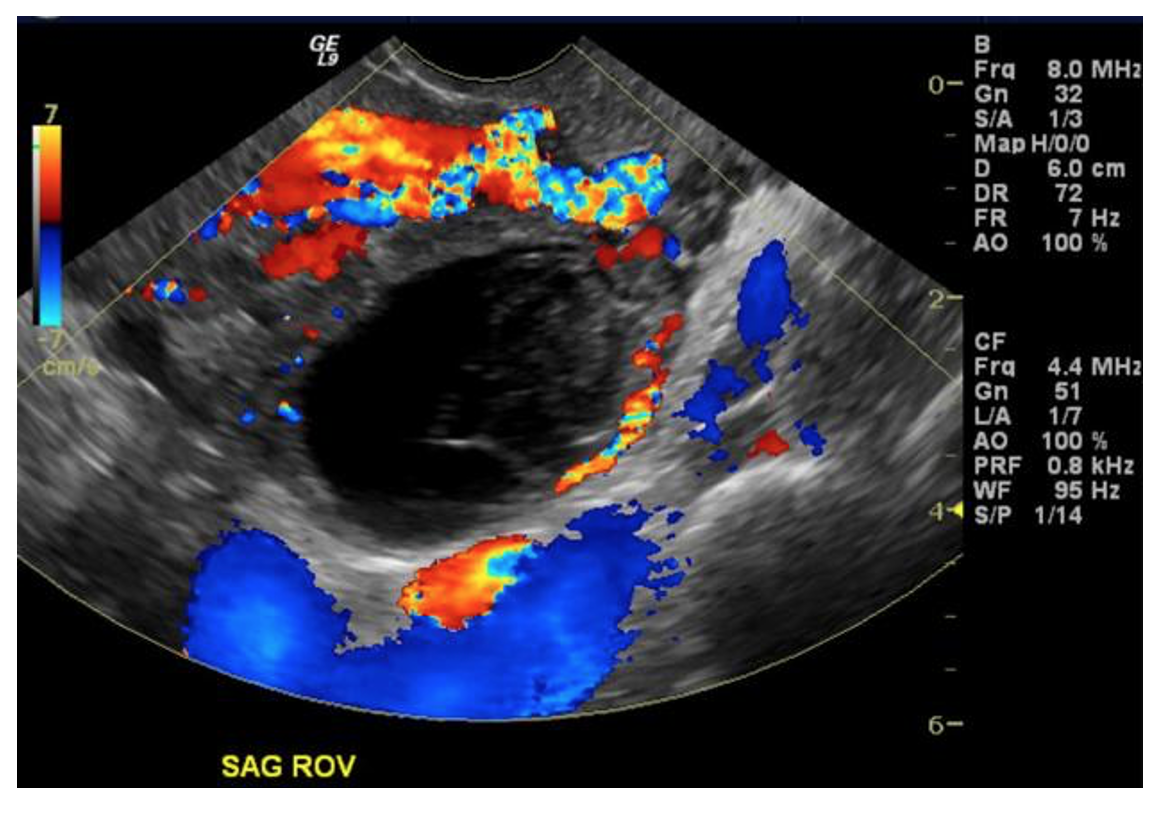
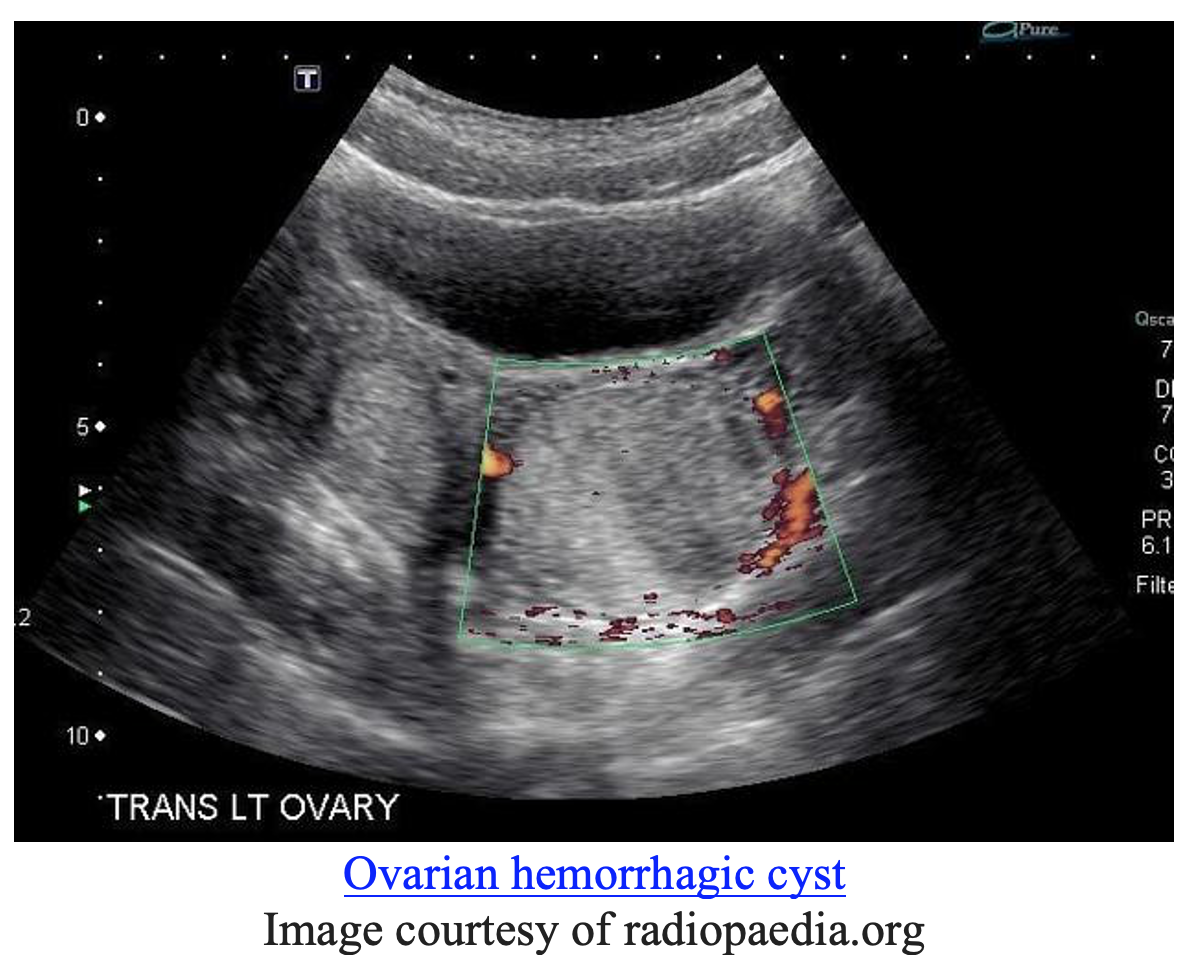
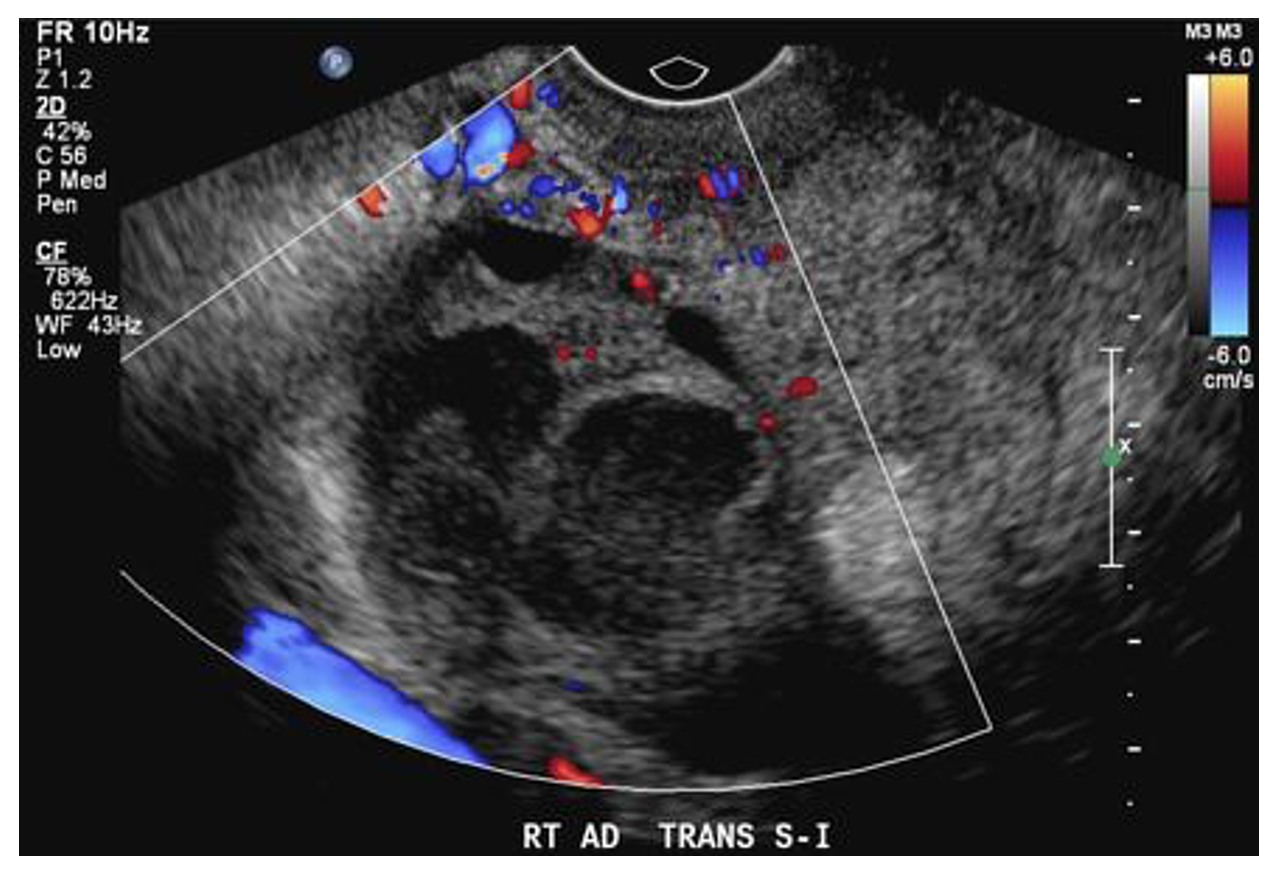
In cases of hemorrhagic cysts, ultrasound might reveal large thin walled cysts in the ovaries with no internal blood flow. A “ring of fire”, or peripheral circumferential blood flow, might be seen as above (11). A FAST exam could help us evaluate for a brisk bleed if there was concern for hemodynamic instability.
Most hemorrhagic cysts resolve without intervention but patients with significant hemoperitoneum and blood loss warrant admission. A laparoscopy would be indicated in the hemorrhage needs to be controlled or if the patient becomes unstable (12).
Tubo-ovarian Abscess
If our patient in Case #2 had fevers and chills accompanied with vaginal discharge our differential might have tubo-ovarian abscess (TOA) move up to the top of the list. Patients with TOA might have adnexal tenderness, cervical motion tenderness, and possibly signs of systemic infection such as tachycardia and hypotension. Pelvic ultrasound should be obtained. For TOA a mix of TVUS and transabdominal ultrasound can be utilized.
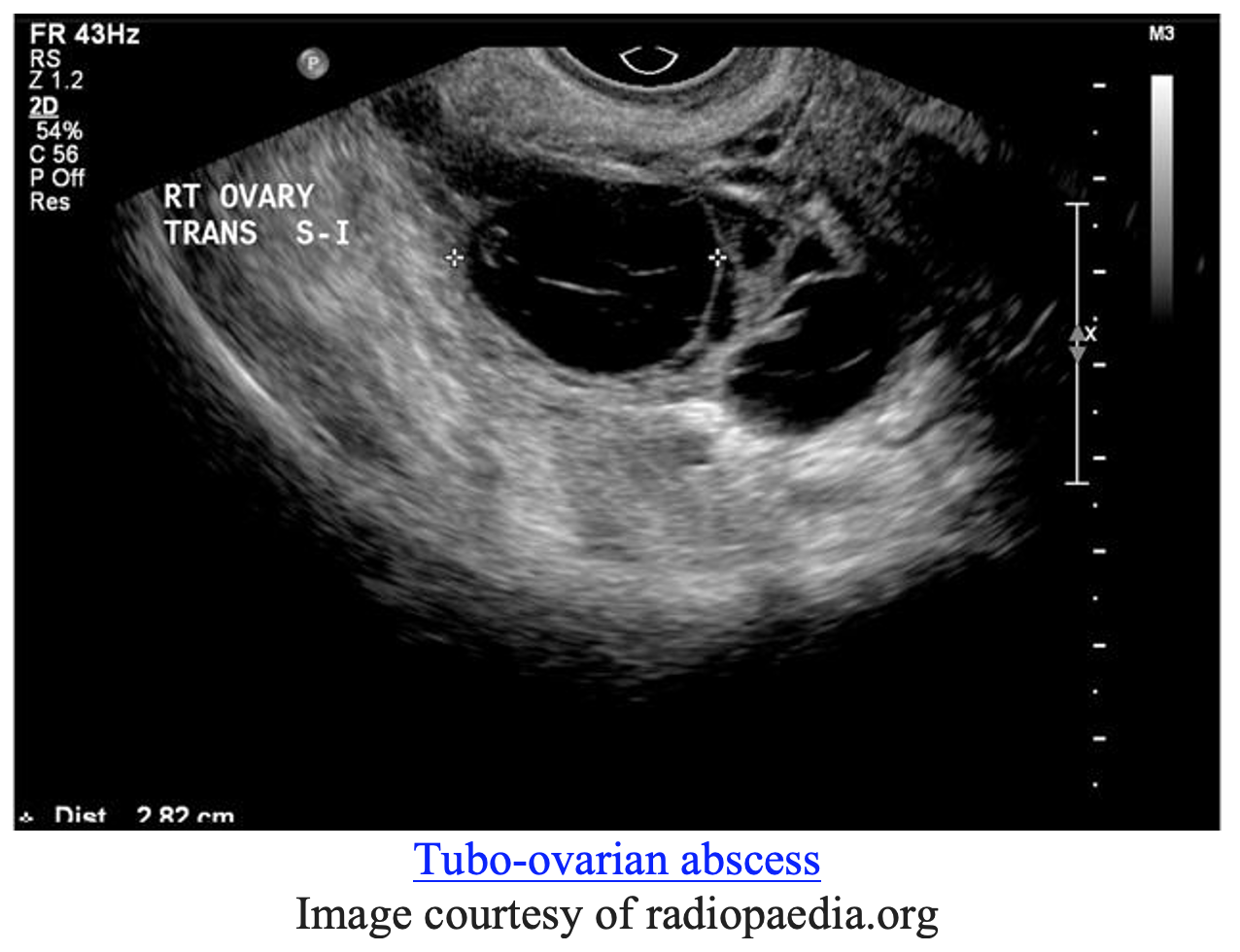
On ultrasound we might see a “tubo-ovarian complex”, where the ovary can become adherent to the tube and form one inflammatory mass as above (13). Free fluid might be seen within the pouch of Douglas, the deepest point of the peritoneal cavity posterior to the uterus. The ovary may take on a polycystic appearance from edema (13). The TOA might be seen unilaterally or bilaterally. Early initiation of broad-spectrum antibiotics, GYN consultation, and hospitalization are indicated for patients with TOA.
If the pelvic ultrasound is inconclusive then further imaging should be pursued. If the pelvic pain is localized to the right lower quadrant a CT can be useful to assess for appendicitis. CT can also help determine if an adnexal mass might represent ovarian malignancy (13). If there is concern for malignancy or if the patient is not responding to antibiotics, then surgical intervention might be indicated. Prompt surgical intervention is also required for cases of TOA rupture (14).
Pearls & Pitfalls
Ectopic Rule Out
- Failure to Visualize Necessary Structures
- To confirm an IUP three structures must be visualized: gestational sac, yolk sac, and fetal pole.
- While the gestational sac below may evolve into a normal IUP, a gestational sac alone does not confirm a current IUP. This patient would still need close follow up and repeat imaging.
Gestational sac not diagnostic for IUP
Video courtesy of The Point of Care Ultrasound Atlas
- Relying too much on discriminatory zone
- The discriminatory zone is not perfect.
- There have been cases of patients having an hCG >2000 with no evidence of an IUP but then developing into a normal IUP upon follow up (15).
Ovarian Torsion
- Ovarian torsion remains a clinical diagnosis. Presence of blood flow on doppler does not rule out torsion.
- The ovary has dual blood supply and therefore can appear to have normal doppler flow on ultrasound even in the setting of ovarian torsion (10, 16).
- The definitive diagnosis is therefore made by direct visualization via laparoscopy. Early GYN consultation can be helpful in equivocal cases.
- While ultrasound is frequently the imaging study of choice for suspected ovarian torsion, CT may also help identify this condition.
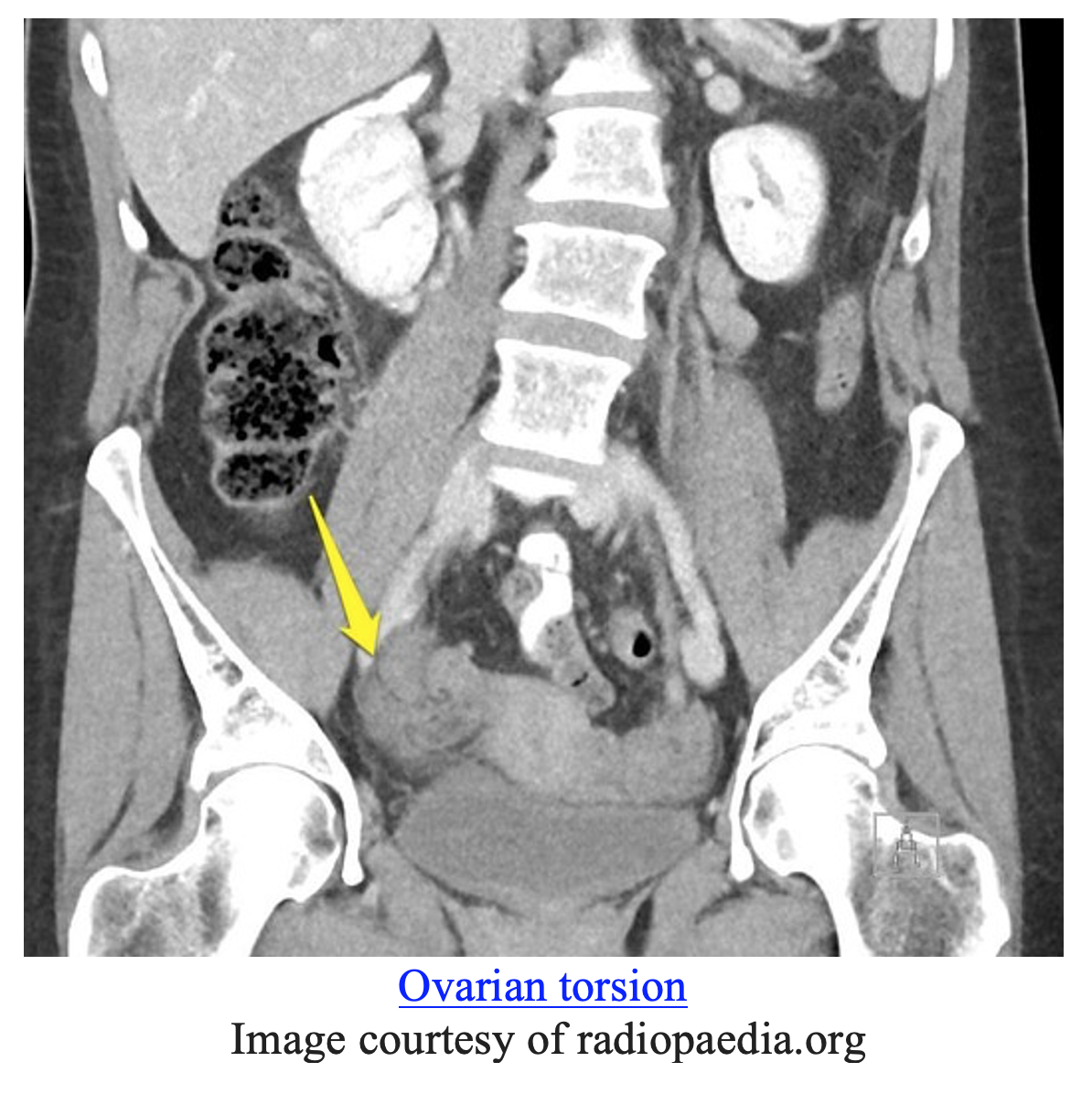
- CT scan might reveal a “whirl sign”, seen below (16).
- Other signs of ovarian torsion on CT include uterine deviation to the side of the torsion, ascites, and an enlarged ovary (16).
Hemorrhagic Cyst
- Remember the “ring of fire” to aid in diagnosis of hemorrhagic cysts (11).
- Serial examinations are important – if the patient becomes hemodynamically unstable or if there is concern for continued brisk bleeding OB/GYN should be consulted early for possible surgical management.
Tubo-ovarian Abscess
- TOA can present as a “tubo-ovarian complex” on ultrasound due to the inflammation and local irritation of tissues.
- If there is hemodynamic instability or concern for TOA rupture then prompt surgical management is needed.
- Don’t forget about other possible diagnoses that might present similarly to a TOA such as appendicitis or ovarian malignancy.
Limitations of Pelvic Ultrasound
- POCUS is operator dependent, meaning imaging acquisition and interpretation vary based on operator’s skill and training, is by definition a limited study intended to answer a specific clinical question, and does not replace a formal radiology study.
- POCUS is only indicated for pelvic pain within the scope of early pregnancy. Radiology services are required outside of this indication.
- Pelvic ultrasound can be limited by pain or comfort level of the patient.
Take Home Points
- POCUS should be performed to assess for ectopic pregnancy and free fluid; other causes of pelvic pain require formal ultrasonography.
- To diagnose IUP you need: gestational sac with a fetal pole and yolk sac all within the uterus.
- If a patient is diagnosed with a pregnancy of unknown location with a hCG of 1,500-2,000 then ruling out ectopic pregnancy and counseling the patient on close follow up for repeat ultrasound is the best course of action.
- Ultrasound with doppler is the first step of imaging for ovarian torsion, but if unrevealing and strong clinical concern exists then obtain a GYN consultation.
- Most hemorrhagic cysts do not need operative management.
- CT is indicated in possible cases of TOA if ultrasound is equivocal.
References / Further Reading
- American College of Emergency Physicians: Council Resolution on Ultrasound. ACEP News. November 1990.
- Whitson MR, Mayo PH. Ultrasonography in the emergency department. Critical Care. 2016;20(227). doi:10.1186/s13054-016-1399-x
- Panebianco NL, Shofer F, Fields JM, et al. The utility of transvaginal ultrasound in the ED evaluation of complications of first trimester pregnancy. The American Journal of Emergency Medicine. 2015;33(6):743-748. doi:10.1016/j.ajem.2015.02.023
- Schaik GWWV, Schaik KDV, Murphy MC. Point‐of‐Care Ultrasonography (POCUS) in a Community Emergency Department: An Analysis of Decision Making and Cost Savings Associated With POCUS. Journal of Ultrasound in Medicine. 2018;38(8):2133-2140. doi:10.1002/jum.14910
- Braffman BH, Coleman BG, Ramchandani P, et al. Emergency department screening for ectopic pregnancy: a prospective US study. Radiology. 1994;190(3):797-802. doi:10.1148/radiology.190.3.7509494
- Doubilet PM, Benson CB, Bourne T, Blaivas M. Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester. New England Journal of Medicine. 2013;369(15):1443-1451. doi:10.1056/NEJMra1302417
- Moore C, Todd WM, O’Brien E, Lin H. Free Fluid in Morison’s Pouch on Bedside Ultrasound Predicts Need for Operative Intervention in Suspected Ectopic Pregnancy. Academic Emergency Medicine. 2008;14(8). doi:10.1197/j.aem.2007.04.010
- Mateer JR, Valley VT, Aiman E, Phelan MB, Thoma ME, Kefer MP. Outcome Analysis of a Protocol Including Bedside Endovaginal Sonography in Patients at Risk for Ectopic Pregnancy. Annals of Emergency Medicine. 1996;27(3):283-289. doi:10.1016/s0196-0644(96)70260-3
- Mashiach R, Melamed N, Gilad N, Ben-Shitrit G, Meizner I. Sonographic diagnosis of ovarian torsion: accuracy and predictive factors. Journal of Ultrasound Medicine. 2011;9. doi:10.7863/jum.2011.30.9.1205
- Robertson JJ, Long B, Koyfman A. Myths in the Evaluation and Management of Ovarian Torsion. Journal of Emergency Medicine. 2017;52(4). doi:10.1016/j.jemermed.2016.11.012
- Sayasneh A, Ekechi C, Ferrara L, et al. The characteristic ultrasound features of specific types of ovarian pathology (Review). International Journal of Oncology. 2015;46(2):445-458. doi:10.3892/ijo.2014.2764
- Teng S-W, Tseng J-Y, Chang C-K, Li C-T, Chen Y-J, Wang P-H. Comparison of Laparoscopy and Laparotomy in Managing Hemodynamically Stable Patients with Ruptured Corpus Luteum with Hemoperitoneum. The Journal of the American Association of Gynecologic Laparoscopists. 2003;10(4):474-477. doi:10.1016/s1074-3804(05)60147-8
- Munro K, Gharaibeh A, Nagabushanam S, Martin C. Diagnosis and management of tubo-ovarian abscesses. The Obstetrician & Gynaecologist. 2018;20(1):11-19. doi:10.1111/tog.12447
- Pedowitz P, Bloomfield RD. Ruptured adnexal abscess (tuboovarian) with generalized peritonitis. American Journal of Obstetrics and Gynecology. 1964;88(6):721-729. doi:10.1016/0002-9378(64)90604-0
- Mehta TS, Levine D, Beckwith B. Treatment of ectopic pregnancy: is a human chorionic gonadotropin level of 2,000 mIU/mL a reasonable threshold? Radiology. 1997;205(2). doi:10.1148/radiology.205.2.9356647
- Chang HC, Bhatt S, Dogra VS. Pearls and Pitfalls in Diagnosis of Ovarian Torsion. 2008;28(5). doi:10.1148/rg.285075130




