
Authors: Alec Pawlukiewicz, BA (Vanderbilt University School of Medicine) and Drew A. Long, BS (@drewlong2232, Vanderbilt University School of Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
Case Presentation
You are working the night shift in the ED, and you see the next patient is a 38-year-old female complaining of dizziness. Her vital signs include HR 82, BP 115/70, RR 12, O2 saturation 99%, and T 37 C. She describes her dizziness as a sensation of the room spinning, and her dizziness began yesterday and has worsened today. It is associated with severe nausea and vomiting. Her past medical history is notable for type I diabetes. She has never had any previous episodes of dizziness. Is she having a posterior stroke? How can you evaluate this patient for a life-threatening cause of dizziness?
Background
Worldwide, stroke is a major cause of disability and mortality.1 In the U.S., around 795,000 strokes occur every year.2 Posterior circulation strokes account for approximately 20% of ischemic strokes.3 Unfortunately, many of these posterior strokes are initially misdiagnosed or remain undiagnosed.4 Misdiagnosis of posterior circulation strokes presenting with dizziness is common, occurring in up to 35% of cases.5 The common causes of posterior circulation strokes include embolic causes, atherosclerosis (and subsequent stenosis), small vessel disease, and arterial dissection.6-9 The posterior circulation supplies approximately 20% of the brain.10 See Figure 1 for the anatomy of the posterior circulation and Table 1 for the areas supplied.
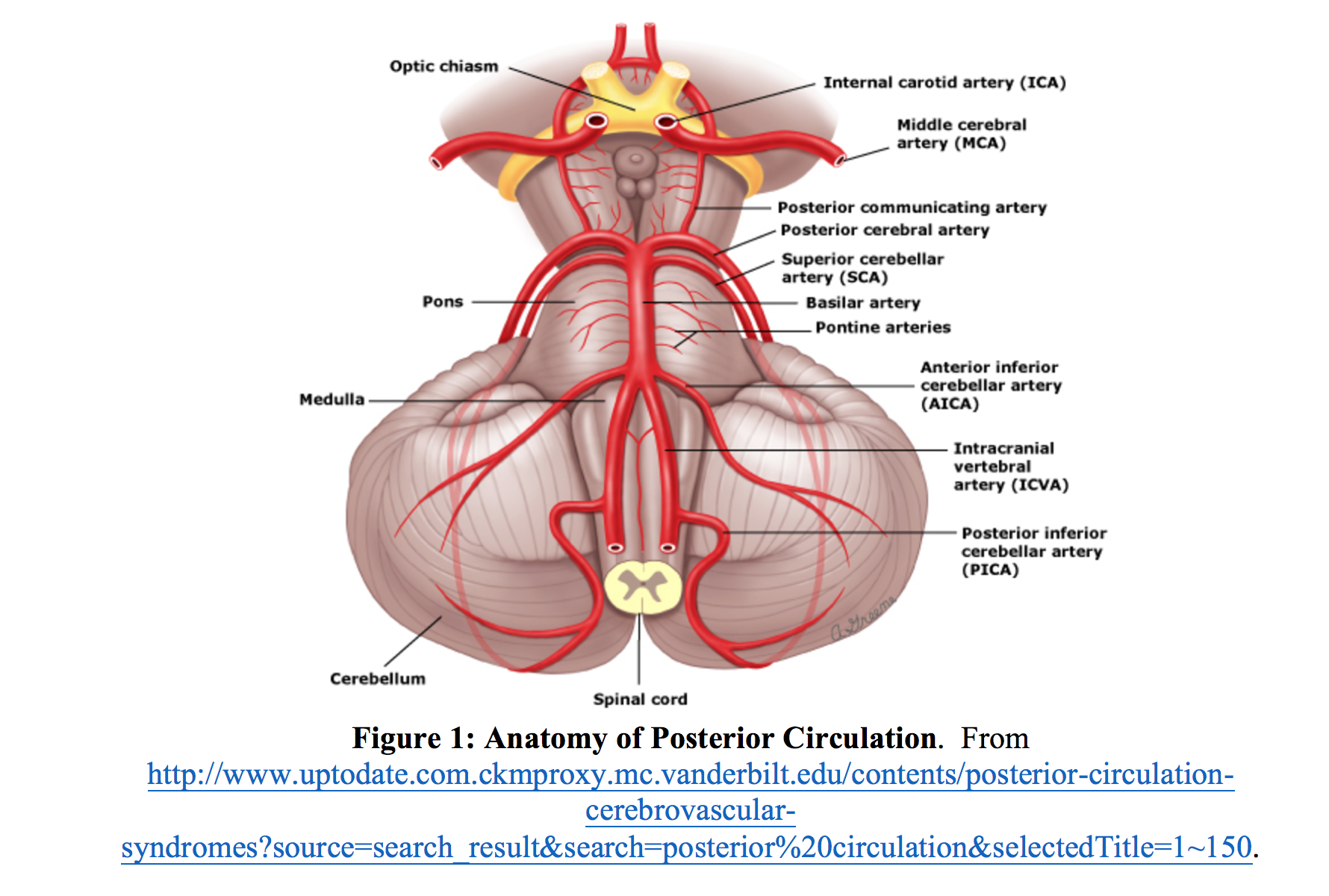
Table 1: Areas Supplied by Posterior Circulation11
| Artery | Area Supplied |
| Vertebral Artery | Brainstem |
| PICA | Cerebellum |
| Basilar Artery | Thalamus |
| Posterior cerebral | Auditory/vestibular structures |
| Medial temporal lobe | Visual occipital cortex |
Clinical Presentation
The clinical presentation of posterior circulation strokes can vary widely and depends on the location of the infarct. Posterior circulation strokes commonly present with symptoms of altered mental status, vision changes, speech changes, nystagmus, vertigo, ataxia, limb weakness, headache, and a variety of other focal neurological deficits.12,13 Of note, these focal neurological deficits may be absent or subtle, leading to difficulty diagnosing posterior strokes.13,14 One particularly challenging presentation of posterior circulation stroke is patients with acute vestibular syndrome (AVS), which often manifests with vertigo or “dizziness.” This review will focus on dizziness or vertigo and the posterior circulation.
Categorizing Dizziness
A common, classic first step in evaluating a patient with dizziness is to have them characterize what they mean by “dizzy,” as dizziness is an imprecise descriptor. Dizziness is often used by patients to describe a wide variety of experiences, which can be categorized into one of four categories. These include vertigo (illusion of motion, often spinning), near syncope (feeling of impending fainting), disequilibrium (loss of balance while walking), and nonspecific dizziness.15 Unfortunately, having the patient describe what they mean by “dizzy” has been shown to be an unreliable indicator of the underlying pathology.16,17 A study by Newman-Toker et al. found that patients frequently changed their descriptors of the type of dizziness if questioned in a different manner after only 10 minutes.18 These studies bring into question the utility of a patient’s description and characterization of “dizziness.”
A newer method of categorizing “dizziness” deals with the timing and triggers of its onset.14 One study has shown that despite the unreliability of the description of the dizziness, patients often reliably relate the context and timing of its onset.19 These categories are displayed in Table 2.
Table 2. Categories of Timing and Triggered Based Vestibular Syndromes14
| Vestibular Syndrome | Duration | Asymptomatic Periods | Triggers? |
| Acute Vestibular Syndrome | > 24 Hours | No | No |
| Triggered Episodic Vestibular Syndrome | < 1 minute | Yes | Yes |
| Spontaneous Episodic Vestibular Syndrome | Minutes to hours | Yes | No, but may have exacerbating factors |
Vestibular Syndromes include Acute Vestibular Syndrome (AVS), Triggered Episodic Vestibular Syndrome, and Spontaneous Episodic Vestibular Syndrome. Table 2 lists defining characteristics of these syndromes. Table 3 lists common benign and dangerous causes of these categories of dizziness. The dizziness associated with posterior circulation strokes often falls into the category of AVS. AVS is characterized by a rapid onset of vertigo, in addition to nausea/vomiting and gait unsteadiness. AVS is often associated with head motion intolerance and nystagmus that can last for days to weeks.20
Table 3. Benign and Dangerous Causes of Dizziness14
| Vestibular Syndrome | Common Benign Cause | Dangerous Cause(s) |
| Acute Vestibular Syndrome | Vestibular neuritis | Stroke |
| Triggered Episode Vestibular Syndrome | BPPV | Posterior Fossa Tumor |
| Spontaneous Episodic Vestibular Syndrome | Vestibular migraine | TIA, Cardiac Dysrhythmia |
Peripheral vs. Central Causes of AVS
The differential diagnosis of AVS can be broken into peripheral and central causes. It is imperative the Emergency Physician consider central causes of vertigo. Central causes include those disorders that affect the structures of the central nervous system such as the cerebellum and the brainstem. The most common, dangerous central cause of AVS is a posterior circulation stroke. Peripheral causes are those that affect CN VIII and the vestibular apparatus. The most common peripheral causes of AVS are vestibular neuritis and labyrinthitis.20 A list of signs and symptoms associated with peripheral and central causes is shown in Table 4. The Emergency Physician (EP) must keep in mind many of the distinguishing features of peripheral lesions may also be present in central lesions. For example, while auditory symptoms are typically associated with peripheral processes, their presence does not exclude a central process.21
The evaluation for stroke in AVS is particularly important in those patients who are older, have hypertension or cardiovascular disease, are on anticoagulation, or have other classic stroke risk factors.22 However, the EP must keep in mind younger age is not sufficient reason to exclude the potential diagnosis of stroke. It is estimated one in five strokes causing AVS affects a patient less than 50 years of age and one in ten patients less than 40 years of age.20 One study found 50% of patients misdiagnosed after suffering a posterior circulation stroke were under the age of 50.23 The overall mortality described by this study was 40%, with a 50% prevalence of significant neurological disability among the survivors.23 These findings convey the significance of thorough assessment for central pathologies in patients with AVS.
Table 4: Signs/ Symptoms Differentiating Peripheral and Central Vertigo22
| Peripheral | Central | |
| Onset | Sudden or Insidious | Sudden |
| Severity of Vertigo | Intense Spinning | Ill-defined, may be severe or less intense |
| Prodromal Dizziness | Occurs in up to 25%, often single episode | Occurs in up to 25%, recurrent episodes suggest TIA’s |
| Intolerant of head movements/Dix-Hallpike Maneuver | Yes | Varies, but often intolerant |
| Associated Nausea/Diaphoresis | Frequent | Variable, but often frequent |
| Auditory Symptoms | Points to peripheral causes | May be present |
| Proportionality of Symptoms | Usually proportional | Often disproportionate |
| Headache/Neck Pain | Unusual | More likely |
| CNS signs/symptoms | Absent | Usually present |
| Head Impulse Test | Abnormal | Often normal |
| Nystagmus | Horizontal | Vertical/direction-changing |
| HINTS Testing | Negative | Abnormal in at least 1 out of 3 tests |
Physical Exam
A focused neurological exam, including gait assessment, speech, and cranial nerves, in patients presenting with AVS is needed. Focal neurological deficits are consistent with a central cause of AVS. However, the absence of neurological deficits does not exclude a central cause. One review of AVS secondary to strokes found focal neurological deficits were present in 80% of cases.24 Additionally, Dix-Hallpike testing, while effective in diagnosing BPPV (a cause of triggered episodic vestibular syndrome), provides no diagnostic utility in the assessment of AVS.14 A potential tool for the Emergency Physician in evaluating patients with AVS is the HINTS examination.
HINTS Testing
HINTS testing is a three-part examination that consists of head impulse testing, nystagmus assessment, and test of skew. This test is the gold standard for diagnosis of posterior circulation strokes, as its sensitivity is higher than any imaging modality in the first 24-48 hours after symptom onset. The HINTS test should be used in patient complaining of continuous feelings of vertigo or dizziness, where concern for AVS is present. It is not useful in patients with momentary position-related vertigo or patients with TIAs who are not dizzy when examined.25 For a great overview, see EMCrit at https://emcrit.org/podcasts/posterior-stroke/.
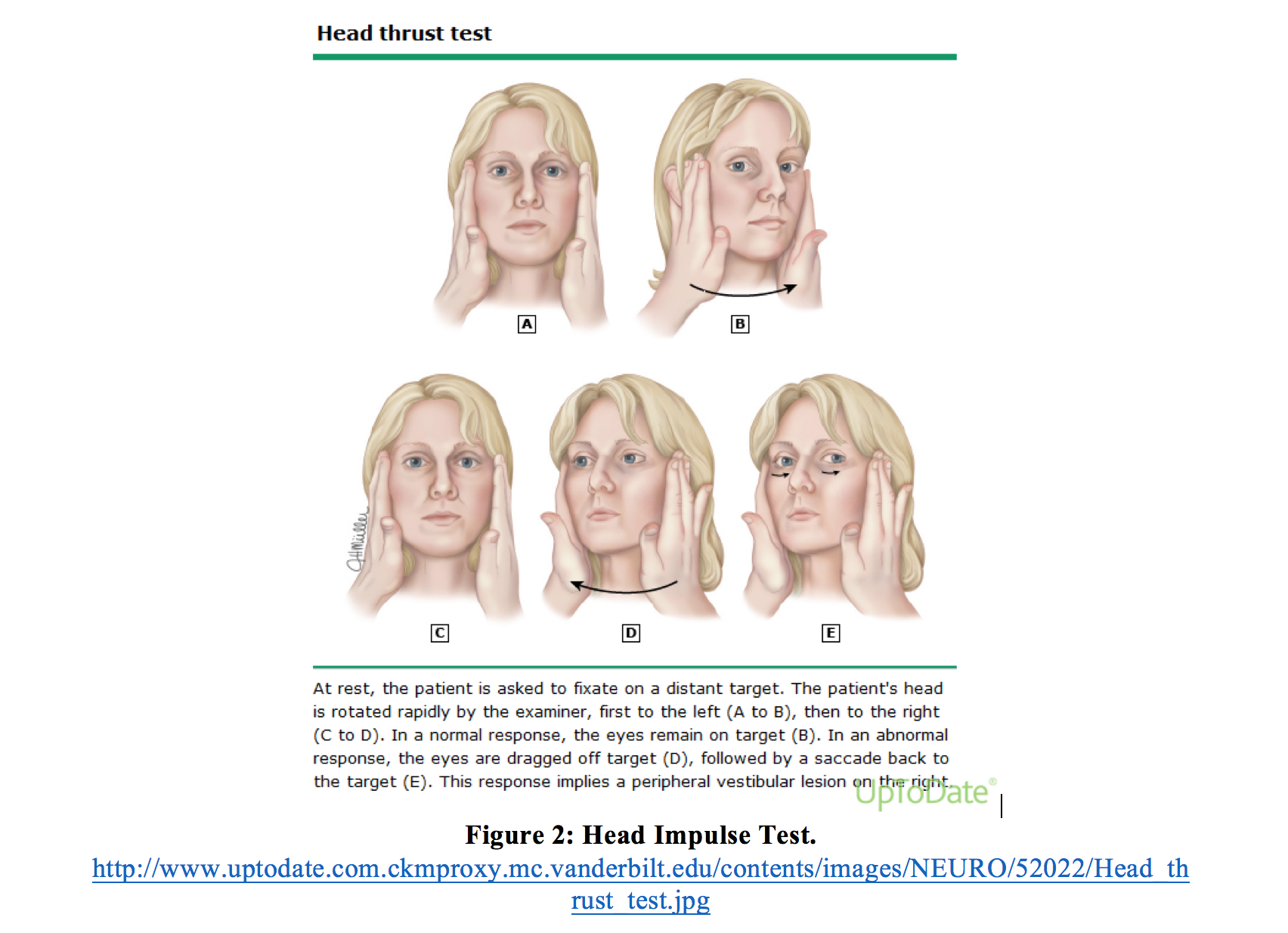
The first component of the HINTS test is head impulse testing. Head impulse testing consists of having the patient visually fixate on a target followed by a rapid 40 degree head turn. This process is then repeated in the other direction. A unilateral abnormal finding (saccade) is consistent with a peripheral process and a normal response (no saccade) to this testing is consistent with a central process (Kattah, Edlow).14,20 This test is depicted in Figure 2 and an abnormal response is shown in Video 1.
Video 1: Abnormal Head Impulse Test
The second component of the HINTS test is assessment of nystagmus, which analyzes the characteristics of nystagmus during lateral gaze at 45-60 degrees, not at end-gaze. Direction changing nystagmus is consistent with a central cause of AVS and unidirectional horizontal nystagmus is more consistent with a peripheral cause. Assessment of nystagmus is specific but not sensitive for a central cause of AVS.22 Vertical or torsional nystagmus in a patient with AVS is a sign of a central etiology. However, strokes presenting with AVS may have a normal (horizontal) finding of nystagmus.20 A study by Lee et al. found that approximately half of pseudolabyrinthine strokes present with unilateral, horizontal findings of nystagmus.26
The final component of the HINTS test is the test of skew, which assesses ocular misalignment. This is determined using the alternating cover test, which consists of covering one eye and then assessing for any movement/re-fixation when the eye is uncovered. Any realignment is consistent with a central process. An abnormal test of skew is shown in Video 2. This test is also specific but not sensitive for central causes of AVS.22
Video 2: Abnormal Test of Skew
A helpful mnemonic for the HINTS testing results that are consistent with central causes is INFARCT (Impulse Normal, Fast-phase Alternating, Refixation on Cover Test).20
Table 5. INFARCT mnemonic for HINTS findings suggestive of central cause of vertigo.20
| INFARCT mnemonic |
| Impulse Normal |
| Fast-phase Alternating |
| Refixation on Cover Test |
Buyers Beware…
Many of the studies evaluating the HINTS exam utilized neuro-ophthalmologists with specialized equipment and training, often in patients not in the ED. Thus, translating this to regular ED practice must be done with caution. A slow-motion camera (there are several apps available for phone use) can assist in detecting subtle ocular findings. More studies are needed evaluating the HINTS exam conducted by emergency physicians on ED patients. For more potential pitfalls in the ED, please see EMCrit at https://emcrit.org/emnerd/adventure-veiled-lodger/.
Imaging
What is the role of imaging in the ED evaluation of patients with vertigo? Patients with physical exam findings concerning for a central process require urgent imaging to assess for hemorrhage, infarction, or tumor.22 In regards to the type of imaging, MRI in addition to CT is preferred due to poor visualization of the posterior fossa with CT.27 The sensitivity of brain CT for posterior circulation infarcts is only 7-42%.28-31 However, even a negative MRI does not rule out a posterior circulation stroke in patients with a high clinical suspicion for a central cause. MRI with DWI within the first 48 hours of infarction may miss up to 10-20% of posterior circulation strokes.32
The most important tool to evaluate for a central cause in patients with AVS is the HINTS exam performed by an experienced physician. In the evaluation of posterior circulation stroke, Kattah et al. examined the various methods for diagnosis, shown in Figure 3.20 An abnormal HINTS test has been shown to be 100% sensitive and 96% specific for the detection of central causes of AVS, making it more sensitive than even MRI in the first 24-48 hours.20 Furthermore, a brain MRI takes at least 5-10 minutes to conduct not considering wait time, in addition to thousands of dollars in cost. The HINTS test can be done in minutes at no additional cost.
Figure 3. Diagnostic Modalities for Posterior Circulation Stroke20

Disposition
In considering the disposition of these patients, Edlow et al. in 2015 recommended disposition criteria.14 They recommended a patient presenting with AVS is likely safe to go home if:
- Patient is able to sit and stand independently
- Patient has no cranial or cerebellar signs
- Patient has HINTS testing suggestive of a peripheral process
HINTS exam results indicative of peripheral vertigo are unidirectional, horizontal nystagmus, unilaterally abnormal head impulse test, and normal vertical eye alignment (no skew). Together, these findings reduce the odds of a stroke by at least 50 fold.24
Pearls and Pitfalls
Pearls
- Clarify what the patient means by dizziness regarding timing and triggers of the onset of symptoms. Distinguish dizziness from syncope or other mimicking conditions, as these will require a different work-up.
- Suspect a central etiology in patients with acute vestibular syndrome. Evaluate with the HINTS exam.
- Use the HINTS test in patients presenting with Acute Vestibular Syndrome, as this is more sensitive than both CT and MRI for posterior circulation strokes.
- Nystagmus is assessed during lateral gaze at 45-60 degrees, not at end-gaze. An abnormal response in a patient with AVS is vertical or torsional nystagmus.
- The HINTS exam should only be used in patients presenting with Acute Vestibular Syndrome, not patients with Triggered or Spontaneous Episodic Vertigo Syndrome.
Pitfalls
- Symptoms that worsen with movement do not confirm a peripheral process. Symptoms with movement may also exacerbate symptoms from a central process.
- A normal head CT is not sufficient in excluding ischemic stroke.
- MRI should not be relied upon in the initial 24-48 hours after symptom onset to rule out a posterior circulation stroke, as it may miss up to 10-20% of posterior circulation strokes.
- Younger age does not exclude central causes of Acute Vestibular Syndrome. A stroke should still be suspected in patients younger than 50 if the physical exam is concerning for a central process.
- Many of the classic distinguishing features of peripheral lesions are also found in central lesions.
Case Resolution
You return to the room of the 38 y/o female with dizziness to gather a more detailed history and physical. You determine that the patient’s dizziness began yesterday morning after she awoke, was constant all day yesterday, and has not resolved today. She has experienced difficulty walking since yesterday and is still feeling dizzy currently. Astutely categorizing this patient as exhibiting AVS, you conduct a HINTS exam in addition to a neurologic exam. The HINTS exam is notable for direction-changing nystagmus and a positive test of skew. Concerned for a central etiology of this patient’s vertigo, you order a brain MRI in addition to consulting neurology for further workup and management.
This post is sponsored by www.ERdocFinder.com, a supporter of FOAM and medical education, who with their sponsorship are making FOAM material more accessible to ER physicians around the world.

References/Further Reading
- Lozano R, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010.
Lancet. 2012 Dec;380(9859):2095-128. - Mozaffarian D et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association
- Savitz S, Caplan L. Vertebrobasilar Disease. N Engl J Med 2005;352:2618-26
- Ferro JM, Pinto AN, Falcao I, et al. Diagnosis of stroke by the nonneurologist: a validation study. Stroke 1998;29:1106-9.
- Kerber KA, Brown DL, Lisabeth LD, Smith MA, Morgenstern LB. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: a population-based study. Stroke. 2006;37: 2484–2487.
- Caplan LR, Wityk RJ, Glass TA, et al. New England Medical Center Posterior Circulation Registry. Ann Neurol 2004;56:389-98.
- Bogousslavsky J, Van Melle G, Regli F. The Lausanne Stroke Registry: analysis of 1,000 consecutive patients with first stroke. Stroke 1988;19:1083-92.
- Moulin T, Tatu L, Vuillier F, Berger E, Chavot D, Rumbach L. Role of a stroke data bank in evaluating cerebral infarction subtypes: patterns and outcome of 1,776 consecutive patients from the Besancon Stroke Registry. Cerebrovasc Dis 2000;10:261-71.
- Vemmos K, Takis C, Georgilis K, et al. The Athens Stroke Registry: results of a five-year hospital-based study. Cerebrovasc Dis 2000;10:133-41.
- Crocco T, Goldstein J. Stroke. In Marx J, Hockberger R, Walls R. Rosen’s Emergency Medicine. 2014; 8: 1363-1374.
- Go S, Worman D. Stroke Syndromes. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. New York, NY: McGraw-Hill; 2016.
- Searls DE, Pazdera L, Korbel E, Vysata O, Caplan LR: Symptoms and signs of posterior circulation ischemia in the New England Medical Center Posterior Circulation Registry. Arch Neurol. 2012; 69: 346.
- Bradley WG, Daroff RB, Fenichel GM, Marsden CD (eds): Neurology in Clinical Practice, 4th ed. Philadelphia, PA: Butterworth-Heinemann; 2004.
- Edlow JA, Newman-Toker D. Using the Physical Exam to Diagnose Patients with Acute Dizziness and Vertigo. J Emerg Med. 2016 Apr 50(4): 617-28.
- Drachman DA, and Hart CW: An approach to the dizzy patient. Neurology 1972; 22: pp. 323-334
- Kerber KA, Newman-Toker DE. Misdiagnosing dizzy patients: common pitfalls in clinical practice. Neurol Clin 2015;33:564–76
- Newman-Toker DE, Edlow JA. TiTrATE: a novel approach to diagnosing acute dizziness and vertigo. Neurol Clin 2015;33:577–99.
- Newman-Toker DE, Cannon LM, Stofferahn ME, Rothman RE, Hsieh YH, Zee DS. Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting. Mayo Clin Proc 2007;82:1329–40.
- Bisdorff A, Staab J, Newman-Toker D. Overview of the international classification of vestibular disorders. Neurol Clin 2015;33: 541–50.
- Kattah JC, Talkad AV, Wang DZ, et al.: HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009; 40: 3504.
- Lee H, Kim JS, Chung EJ, et al.: Infarction in the territory of anterior inferior cerebellar artery: spectrum of audiovestibular loss. Stroke. 2009; 40: 3745.
- Goldman B. Vertigo. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. New York, NY: McGraw-Hill; 2016.
- Savitz SI, Caplan LR, Edlow JA: Pitfalls in the diagnosis of cerebellar infarction. Acad Emerg Med. 2007; 14: 63.
- Tarnutzer AA, Berkowitz AL, Robinson KA, et al.: Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ. 2011; 183: E571.
- Caplan LR. Posterior circulation cerebrovascular syndromes. https://www.uptodate.com/contents/posterior-circulation-cerebrovascular-syndromes. Accessed February 22, 2017.
- Lee H, Sohn SI, Cho YW, et al. Cerebellar infarction presenting isolated vertigo: frequency and vascular topographical patterns. Neurology 2006;67:1178–1183.
- Kerber KA, Schweigler L, West BT, et al.: Value of computed tomography scans in ED dizziness: analysis from a nationwide representative sample. Am J Emerg Med. 2010; 28: 1030.
- Chalela JA, Kidwell CS, Nentwich LM, et al. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet 2007;369:293–8.
- Hwang DY, Silva GS, Furie KL, Greer DM. Comparative sensitivity of computed tomography vs. magnetic resonance imaging for detecting acute posterior fossa infarct. J Emerg Med 2012;42:559–65.
- Kabra R, Robbie H, Connor SE. Diagnostic yield and impact of MRI for acute ischaemic stroke in patients presenting with dizziness and vertigo. Clin Radiol 2015;70:736–42.
- Ozono Y, Kitahara T, Fukushima M, et al. Differential diagnosis of vertigo and dizziness in the emergency department. Acta Otolaryngol 2014;134:140–5.
- Saber Tehrani AS, Kattah JC, Mantokoudis G, et al. Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms. Neurology 2014;83:169–73.






3 thoughts on “Posterior Circulation Strokes and Dizziness: Pearls and Pitfalls”
Pingback: Stroke; the best reviews – Poor Evidence
Pingback: Episode 99 Highlights from EMU 2017 - Emergency Medicine Cases
Pingback: Vertigo – EM Clerkship