Posterior Stroke, HiNTS exam
- Jan 22nd, 2015
- Jason Brown
- categories:
Author: Jason Brown, MD (EM Resident Physician, University of Maryland) // Editor: Alex Koyfman, MD
Background
Posterior strokes make up 1 in every 5 ischemic strokes in the US. That equates to about 150,000 strokes per year involving the posterior circulation with an incidence of 18/100,000. Bottom line: This is a common, emergent diagnosis that every EM physician should be familiar with.
Anatomy
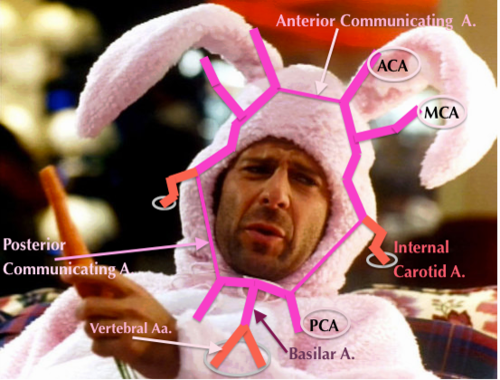 Posterior circulation constitutes the vertebral arteries, basilar artery, and posterior cerebral arteries in addition to all minor perforators. The vascular territory is quite large and perfuses the brainstem, a number of cranial nerve structures, the cerebellum, and the posterior portions of the cerebrum.
Posterior circulation constitutes the vertebral arteries, basilar artery, and posterior cerebral arteries in addition to all minor perforators. The vascular territory is quite large and perfuses the brainstem, a number of cranial nerve structures, the cerebellum, and the posterior portions of the cerebrum.
Signs/Symptoms
Classically, the “Five D’s” were used to describe the signs and symptoms of a posterior stroke: dizziness, diplopia, dysarthria, dysphagia, dystaxia. Additionally, you can have motor and/or sensory deficits, which mimic an anterior circulation stroke. Finally, the clinical findings of “crossed syndromes,” makes the diagnosis very likely.
The Diagnostic Dilemma
Most of the stroke awareness initiative in this country is aimed at the identification of anterior strokes; most famously with the FAST mnemonic (Face drop, Arm droop, Speech disturbance). Studies have shown that using these criteria alone will miss a majority of posterior strokes.
Given such a wide range of presenting symptoms (some of which are very nonspecific), how does an EM physician make this diagnosis?
Diagnostics
First, you must have a high index of suspicion for any patient that presents with a new, focal neurologic deficit. Your history and physical exam are invaluable.
There are imaging modalities that can help you identify acute ischemic strokes; namely, CT angiography and MRI/MRA. The problem here is that both of these studies take quite a bit of time and all CVAs are time-sensitive emergencies.
HiNTS
The HiNTS exam stands for: Head impulse testing, Nystagmus, and a Test of Skew. This exam was designed by Dr Dave Newman-Toker to differentiate central and peripheral causes of vertigo; a common presenting symptom for posterior CVA. This quick battery of tests has been shown to have a 100% sensitivity and 96% specificity for posterior strokes when any one of the three tests are suggestive of a central cause of vertigo.
[table “5” not found /]http://content.lib.utah.edu/cdm/singleitem/collection/ehsl-dent/id/6
Things to Consider
The HiNTS exam takes practice and expertise to properly administer AND interpret.
You should have a high index of suspicion for posterior CVA in patients with vertigo or new neuro deficits.
http://www.ncbi.nlm.nih.gov/pubmed/19762709
http://www.ncbi.nlm.nih.gov/pubmed/24127701
http://www.ncbi.nlm.nih.gov/pubmed/24920847

One thought on “Posterior Stroke, HiNTS exam”