Featured on #FOAMED REVIEW 26TH EDITION – Thank you to Michael Macias from emCurious for the shout out!
Author: Alex Koyfman, MD (Assistant Professor of Emergency Medicine at UT Southwestern Medical Center) // Editor: Justin Bright, MD
Your next 3 patients…
#1: Gastric bypass pt with SIRS criteria
#2: Gastric bypass pt with psychiatric complaints
#3: Gastric bypass pt with nausea/vomiting
The Basics
-Morbid obesity continues to rise significantly (epidemic)
-Increasing # of weight-loss surgeries w/ physical/psych effects => increasing ED visits for postoperative complications
-Increased laparoscopic techniques; each surgical option w/ potential complications
-2 main strategies of surgery: gastric restriction (early satiety) => banding / gastroplasty; intestinal malabsorption (bypass parts of small intestine) => distal gastric bypass / biliopancreatic diversion +/- duodenal switch
-Hospital stays: 3-4 days
Clinical Pearls
–Challenging / unreliable abdominal exam => more extensive work-ups including CT abdo/pelv w/ oral + IV contrast (drink over several hours)
-May not fit into CT scan
–Often don’t manifest symptoms/signs of serious intra-abdominal pathology i.e. signs of peritonitis masked by large amount of intra-abdominal fat
-Lack cardiopulmonary physiologic reserve => quick deterioration; get surgery involved early
-Concern for band migration: need swallow study under fluoroscopy
-Roux-en-Y pts are tricky b/c part of small intestine is bypassed; signs/sxs not classic and abdo XR not reliable
–Fever + tachycardia + increasing abdominal / back pain in Roux-en-Y pt in 1st several weeks post-surgery, pursue anastomotic leak/intra-abdominal abscess; need UGI series vs surgical exploration
-Upper endoscopy has a role in diagnosing bleeding / stricture / stenosis
–Internal hernia: tough dx; many w/ normal labs / XR / UGI series / CT; surgical exploration needed
Surgical options
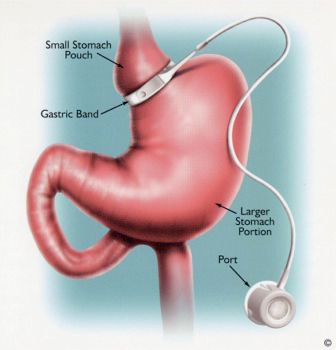
Laparoscopic Adjustable Gastric Banding (LAGB)
-restrictive procedure; very popular outside of US
-adjustable band positioned around upper portion of stomach, then connected to port implanted under skin (allows for loosening/tightening)
-easily reversed; adjust for goal weight loss; lower operative risk/complications
–many sent home same day or next day; return to have band inflated as needed
–favorable long-term results in Europe, less in USA
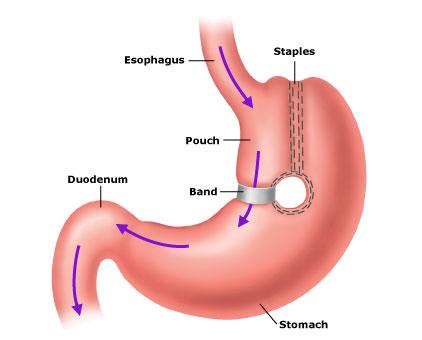
Roux-en-Y Gastric Bypass (RYGBP)
–restrictive procedure and subclinical malabsorption; most popular in US
–laparoscopic (technically challenging) or open; small proximal gastric pouch created, then connected to small bowel (portion of small bowel is bypassed) => malabsorption of calories + dumping syndrome
–sustained long-term weight loss (50-80%) + decrease in co-morbidities (HTN, DM, HLD, etc.)

Biliopancreatic Diversion with or without duodenal switch (BPD, BPD-DS)
–restrictive procedure and surgical malabsorption
-decrease size of stomach (limited gastrectomy) and bypass of duodenum / jejunum +/- duodenal switch
-prevents development of dumping syndrome
-High long-term success (60-80%)

Vertical Banded Gastroplasty (VBG)
–restrictive procedure; less commonly utilized currently
-small pouch created along lesser curvature of stomach using staples, followed by non-adjustable band constricting outlet from pouch
-long-term follow-up: not very effective at keeping off weight (50%); many pts go on to have another weight-loss procedure
Risks/Complications
-Nausea / vomiting: most common chief complaint
-GERD
-Surgical site infection
-Wound dehiscence
–GI bleed
-Acute gastric distention => n/v, bloating, LUQ pain; w/in several days post-op
-who to consider in: Roux-en-Y
–DVT / PE: 2nd most common cause of death
-Chronic abdominal pain
–Incisional hernia
–Bowel obstruction => perforation
-GI-skin fistula
-Metabolic complications => nutritional deficiencies (vitamin B12, folate, calcium, vitamin D, iron, fat-soluble vitamin deficiencies, selenium, zinc, potassium, magnesium, thiamine, protein-energy malnutrition); secondary hyperparathyroidism; pts given multivitamin + Ca supplementation
–who to consider in: Roux-en-Y and biliopancreatic diversion (higher)
–Gastric band breaking / migrating / eroding into GI tract
-Gastric erosion/necrosis/perforation
-Port-site infection / tubing issue
-Anastomotic stricture / stenosis: 1st 6 month after surgery; postprandial pain/n/v; endoscopy is diagnostic/therapeutic
–Internal hernia
-who to consider in: Roux-en-Y
-Marginal/stomal ulcer: w/in 2-4 months; endoscopy
–Anastomotic leak => peritonitis: most common cause of death; w/in 1 month after surgery; tachycardia / dyspnea / AMS / restlessness
-who to consider in: Roux-en-Y and biliopancreatic diversion
-Hepatic dysfunction
–who to consider in: biliopancreatic diversion
-Gallstones/cholecystitis: rapid weight loss + bile stasis
–Dumping syndrome: up to 18 months after surgery; early satiety, nausea/vomiting/loose stools, crampy abdominal pain
-Neuropathy / myopathy / Wernicke’s encephalopathy
-Splenic injury: iatrogenic
-Depression
References
– http://lifeinthefastlane.com/ccc/problems-after-bariatric-surgery/
– http://www.ncbi.nlm.nih.gov/pubmed/24218226
– http://www.ncbi.nlm.nih.gov/pubmed/24373182
– http://www.ncbi.nlm.nih.gov/pubmed/19344551





2 thoughts on “Power Review: Management of the Post-Bariatric Surgery Patient”
There is another Procedure done called the gastric sleeve
Again a partial gastrectomy and no other banding or bypassing done
There is another Procedure done called the gastric sleeve
Again a partial gastrectomy and no other banding or bypassing done